
Research Article | DOI: https://doi.org/10.31579/2643-6612/009
1 Professor of Dental Biomaterials, Faculty of Dentistry, Umm Alqurra University, Makkah, KSA
2 Professor of Dental Biomaterials, Faculty of Dentistry, Mansoura University, Mansoura, Egypt
3 Assistant Professor of Endodontic, Faculty of Dentistry, Umm Alqurra University, Makkah, KSA
*Corresponding Author: Ibrahim M. Hamouda, Professor of Dental Biomaterials, Faculty of Dentistry, Umm Alqurra University, Makkah, KSA.
Citation: Ibrahim M. Hamouda and Majed A. Almalki, Evaluation and correlation of depth cure and degree of conversion of bulk-fill posterior restorative composite resins, J Dentistry and Oral Maxillofacial Surgery. DOI: 10.31579/2643-6612/009
Copyright: © 2019 Ibrahim M. Hamouda, this is an open-access article distributed under the terms of the
Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 April 2019 | Accepted: 22 April 2019 | Published: 26 April 2019
Keywords: Bulk-fill composite resin; Packable composite resin; Depth of cure; Degree of conversion
Background: The problem of composite resin filling is the longer time consumed for incremental application. Bulk-fill composite resins were introduced to the market as substitutes for dental amalgam for restoration of posterior teeth.
Objectives: The aim of this study was to evaluate the curing depth and degree of conversion of two bulk-fill composite resins.
Materials and methods: . Specimens of specific dimensions were prepared from Glacier and SureFil (universal shade, A2), they classified as bulk-fill composite resins. Depth of cure, degree of conversion at different thicknesses for each material (2,3,4,5 and 6 mm) for each thickness separately. The curing depth was determined by the scrapping method (ISO 4049, 2000). The degree of conversion was measured by the Buker FTIR Spectroscopy.
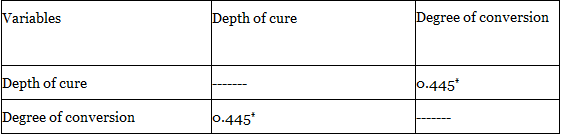
Results: The results indicated that, Glacier composite resin has greater curing depth than that of SureFil composite resin. Glacier composite resin was cured above 6 mm thickness, while SureFil composite resin was cured above 5 mm. In general, the degree of conversion was different at the different thicknesses of the materials. SureFil composite resin showed highest degree of conversion at 3 mm followed by 2 mm thickness, while the lowest degree of conversion was noted at 6 mm thickness. Glacier composite resin has the highest degree of conversion at 3 mm followed by 2 mm thickness, while the lowest degree of conversion was noted at 6 mm thickness. SureFil showed positive correlation between the depth of cure and the degree of conversion. Glacier composite resin showed no significant correlation between the depth of cure and degree of conversion.
Conclusions: The studied bulk-fill composite resins, cured up to 5mm to 6mm thicknesses. 2 and 3mm thicknesses adequately polymerized than 4 mm, 5 mm and 6 mm thicknesses. The degree of conversion of 2 mm and 3 mm thicknesses was greater than that of the other thicknesses. There was positive correlation between the degree of conversion and curing depth of SureFil composite resin. On the other hand, Glacier composite resin showed no significant correlation between the depth of cure and degree of conversion.
Condensable or packable composite resins were discovered in 1980 as an alternative for amalgam. The manufacturers of the bulk-fill composite resin materials claim that their physical properties and handling characteristics are better than those of traditional hybrids and microfills. Some manufacturers and some investigators claim that packable composites can bulk polymerized to a depth of 5 or 6 mm and can be used as amalgam substitutes[1]. The physical, mechanical and aesthetic properties and the clinical behavior of composite resins depend on its structure. Condensable composites are composite resins with a high percentage of filler[2].
The advantages of condensable (bulk-fill) composite resins are condensability (like silver amalgam), ease in achieving a good contact point and better reproduction of occlusal anatomy[3]. The main disadvantages of the bulk-fill are, difficulties in adaptation between one composite layer and another, difficult handling and poor aesthetics in anterior teeth. The main indication of these materials is Class II cavity restoration because they produce better contact points[2].
The degree of conversion is an important factor that affects clinical performance of composite resin restorations[4]. Several methods have been used to determine the degree of conversion of composite resins. Fourier transformation infrared spectroscopy (FTIR) has been widely used as a reliable method for examining the degree of conversion. It detects the C=C stretching vibrations directly before and after curing of materials[5]. FTIR spectra of both uncured and cured samples were analyzed using an accessory of the reflectance diffusion. However, to measure the degree of conversion of bulk resin composite by FTIR, the procedure is time consuming as the polymerized specimens need to be pulverized[6].
Bulk fill technique has been widely used due to the development of material with improved depth of curing[7]. Incremental application of composite resins for cavity filling are reduced by using the bulk-fill techniques when compared with conventional composite resin. Bulk-fill composite resin recommends 4–5 mm increment for cavity filling in contrast to 2 mm increment for conventional composite resin. This technique simplifies the restorative procedure by saving operator time[8]. Bulk fill composite resin was found to be more successful than Hybrid & Micro fill composite resin with respect to depth of cure. The bulk‑fill composite resin showing the highest depth of cure[7].
Incomplete curing of composite resins can lead to early degradation, wear, and less functional durability, and followed by restoration failure. The depth of cure is affected by particle size of the resin composite, light intensity, and curing time[9].
Depth of cure and degree of conversion of composite resins were studied because they are important and clinically relevant measures of the quality of cure. The aim of this study was to investigate the curing depth and degree of conversion of two packable composite resins.
Materials and Methods
The materials used in this study were two types of bulk-fill composite resins, (1) Glacier (Southern Dental Industries Limited, Australia). It is a radiopaque, light cured, microfilled-hybrid composite resin, shade A2 and (2) SureFil (Dentsply Caulk, Lakeview & Clark Avenues, Milford, DE 19963-0359, USA). It is a high-density posterior restorative, hybrid composite, radiopaque, light-cured, highly viscous and packable consistency.
Testing of the curing depth:
20 samples were prepared from both materials by means of a scraping technique described by the International Organization of Standardization (ISO 4049,2000)[10]. Each specimen was prepared by placement of the restorative material past into a cylindrical transparent Perspex mold with 10 mm diameter and 10 mm height. A transparent Mylar strip was placed on the top and bottom of the mold, and excess material extruded by squeezing the mold between two microscope slides. The slides were removed and the mold was placed on a black background with the tip of the light curing unite (SPRING Power LITE 75, USA) applied to the matrix strip on the mold aperture at zero distance. The samples were then light cured from one end (top surface) for 40 seconds (single sided). Immediately after setting, the samples were removed from their molds. The uncured material (on the bottom surface) was scraped off using using a plastic spatula until the set material was reached. The thickness of the cured material was measured at the central portion of the resulting cylinder using a micrometer to an accuracy of ± 0.01 mm. Each sample was measured three times and the mean value of the three readings was recorded as the depth of cure[11,12].
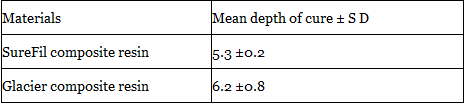
Table 1. Depth of cure (mm) and standard deviations of both composite resin materials.
5 disc-shaped transparent Perspex molds measuring 10 mm diameter and 2,3,4,5 and 6 mm thicknesses were used to prepare 25 samples from SureFil composite resin, 5 samples for each thickness. Also, 25 samples were prepared from Glacier composite resin, 5 samples for each thickness. Samples were prepared and cured between two transparent strips and at zero distance from the curing tip for 40 seconds. The samples were removed from their molds and stored in deionized water for 24 hours at 37Co in dark environment before testing. Each cured specimen was ground into fine powder by using diamond disc mounted on a slow speed hand-piece motor. The fine powder was collected and subjected to the FTIR spectrophotometer for analysis. 10 mg of the composite powder was mixed with 100 mg of potassium bromide (KBr) powder salt. The mixture was placed into a pelleting device and pressed in a hydraulic press to obtain a pellets. The pellets were placed in a holder attachment within the spectrophotometer for FTIR spectrophotometer assessment. Monomer conversion was calculated using changes in the ratios of aliphatic (C=C) to aromatic (C–C) absorption peaks in the uncured (monomer) and cured (polymer) states obtained from the infrared spectra(13). The degree of conversion percent (DC) was calculated for both cured and uncured resin samples using Fourier Transformation Infrared Spectroscopy (Bruker FTIR Spectroscopy, Vector 22, Germany).Testing the Degree of conversion
Statistical analysis
The data collected from this study was exposed to Two-way analysis of variance (ANOVA) to detect any significant difference among the tested groups. When a significant difference was detected, the least significance difference (LSD) was used to detect the significant difference between these groups.
Results:
The results of the depth of cure of the studied bulk-fill materials are presented in Table 1. The depth of cure of SureFil composite resin restorative material was 5.3 mm. Also, the depth of cure of Glacier composite resin restorative material was 6.2 mm. Both studied materials were recorded as bulk-fill restorative materials showed greater depth of cure than that of the conventional composite resin materials.
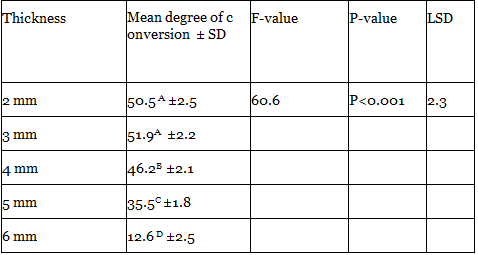
The results of degree of conversion of SureFil composite resin are presented in Table 2. The statistical analysis of the results showed a significant difference among the tested groups of the different thicknesses from the restorative material (P<0>0.05). There were significant differences between 4 mm and 5 mm and 6 mm thickness (P <0>
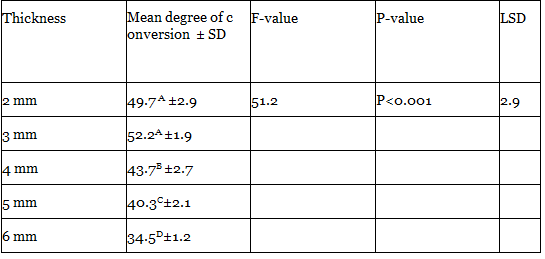
The results of degree of conversion of Glacier composite resin are presented in Table 3. The statistical analysis of the results showed a significant difference among the tested groups of the different thicknesses from the restorative material (P<0>0.05). There were significant differences between 4 mm and 5 mm and 6 mm thickness (P <0>
Bulk-fill composite resins are recently introduced on the market, and the manufacturers, stated that, they could be used in 4- or 5-mm thick increments for restoration of teeth. This would a major technique simplification when compared to the incremental technique [14].
Characteristics of condensable composites are: (1) contain modified ceramic fibers (Aluminum oxide & Silicone dioxide) along with conventional inorganic filler particles that are more coarse and textured (gives these composites the condensable or pack able characteristic), (2) spaces within the fibrous network (resin matrix) are filled with Bis-GMA or UDMA, (3) lower polymerization shrinkage than conventional resin composites due to a higher filler load (>80% by wt). They offer the advantages of having handling characteristics similar to those of amalgam, being able to be light cured in thicker increments than traditional resin composites, and having less shrinkage[15].
Bulk-fill composite resins were found to be more successful than hybrid and microfill composite resin regarding to the depth of cure [7]. The higher depth of cure of the bulk fill materials may be due to the incorporation of more efficient initiator systems and higher translucency of composites. Even though SonicFill is considered to be a bulk fill composite, the true depth of cure was less than 4 mm in this study[16]. It has been demonstrated that filler size and content in dental composites may reduce light penetration and is directly related to depth of cure[17]. The presence of pigments in shaded composite materials should also have an effect on depth of cure because pigments are opaque particles that will limit light penetration and reduce the degree of polymerization at greater depths within a cavity preparation[12].
It is desirable for dental resin composite to convert all of its monomer to polymer during the polymerization reaction. Adequate polymerization is a crucial factor in obtaining optimal physical properties and clinical performance of resin composite restorative materials. However, with high molecular-weight monomers such as BisGAMA or urethane dimethacrylate (UDMA), there is always an incomplete and significant concentration of unreacted C=C remaining within the resin when it is cured with visible light at the oral temperature. In addition to the unreacted monomer, additional unreacted C=C structures may be present, from diluents such as TEGDMA or similar substances. This is believed to be mainly because of limitations on the mobility of reactive groups imposed by the rapid formation of a cross-linked polymeric network[18].
The depth of cure of bulk-fill composite resin is an important factor due to insufficient curing of the deepest part of the composite filling leads to increase of released monomer, decreased strength and stiffness, and weak bonding to the teeth[19]. The depth of cure has been studied by several methods such as scraping test(10), hardness and degree of conversion measurements[19], quantification of released monomers[20], penetrometer test[21], and discoloration test[22]. Bulk-fill composite resin may be easier for dentist to handle than the conventional composite resin. The physical properties of bulk-fill composite resins were superior to those of the micro-filled composite resins but it is not superior to the conventional small-particle hybrid resin-based composite[23].
The present study indicated that, the depth of cure measurements carried out using composite resins shade A2 and curing time 40 seconds because they are clinically relevant. The tip of the curing unit was placed directly over the transparent strip (zero distance) to get the maximum depth of cure and light intensity. The depth of curing is depends on the materials (shade, composition, filler type, amount and size), exposure time, location of light source and quality of the curing unit (type and wavelength of the laboratory photo-curing unit). The depth of curing is directly related to the thickness of the material and the light intensity[24]. This study showed that, the curing depth of bulk-fill Glacier composite resin was greater than that of SureFil, this difference may be due to the difference in the composition of these materials regarding the filler volume, size and shape. The increase in temperature during polymerization of composite resin samples would gave rise to an increase in degree of conversion of the deeper parts of specimen.
The degree of conversion is a measure of the percentage of consumed carbon-carbon double bonds. In other words, the degree of conversion of bis-GMA-based resin composites is the amount of methacrylate groups have polymerized [25]. The degree of conversion obtained from this study was in the range of 34-52%. These results are in agreement with a previous study; the maximum degree of conversion of dimethacrylate-type resins was shown lies close to 50% [26]. In other study the degree of conversion was in the range of 47% to 60% for different types of composite resins. In relation to the samples thickness, there was a statistically significant decrease of degree of conversion. The degree of conversion versus sample’s thickness data was about 45% (2mm thick), 40% (3mm thick), 15% (4mm thick)[27].
The degree of conversion was significantly affected by three variables of material, depth from the surface, and light source and energy level. Degree of conversion showed inverse correlation with specimen depth [18]. There are different methods for the determination of the degree of conversion, such as spectroscopic (e.g. Fourier transform infrared spectroscopy [FTIR] and Fourier transform Raman spectroscopy [FT-Raman]), while others are based on measuring the amount of heat generated during curing (e.g. differential scanning calometry, DSC). The spectroscopic measurements primarily measure the conversion level at the studied surface, while DSC measures the amount of heat that is released by the entire bulk of the material. The degree of conversion after light curing for 40 seconds about 57.34 % (2mm thick), 49.84 % (4mm thick) and 22.55 % (6mm thick) [28].
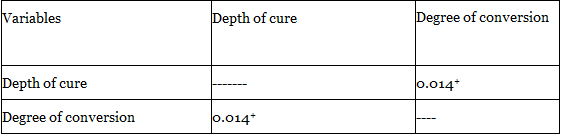
The results of this study showed that, SureFil bulk-fill resin composite has positive correlation between the depth of cure and degree of conversion. On the other hand, there was no correlation between the depth of cure and degree of conversion of Glacier composite resin. The bulk-fill resin composites have similar or more severe cytotoxicity than non-packable resin composites and that cytotoxicity increased when the material applied in a 5 mm bulk increment[29].
Clinical significance
Although, bulk-fill resin composites can be polymerized up to 5-6mm thicknesses but still showed decreased bottom depth of cure and degree of conversion when cured above 4 mm thickness.
Within the limitations of this study, the following conclusions can be obtained:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
