
Research Article | DOI: https://doi.org/10.31579/2690-4861/606
1Department of Physical Therapy, College of Health Professions, Wichita State University, United States.
2Department of Biomedical Sciences, Oklahoma State University Center for Health Sciences, United States.
3Department of Biomedical Engineering, College of Engineering, Wichita State, United States.
4Department of Health and Human Performance, College of Education and Human Services, Cleveland State University, United States.
*Corresponding Author: Ken Pitetti, Department of Physical Therapy, College of Health Professions, Wichita State University, 1845 Fairmount St. Box 210, Wichita, KS, United States.
Citation: Ken Pitetti, Jaya Chakka, Ruth Ann Miller, Michael Loovis, (2024), Evaluating the Postural Control of a Youth with Malan Syndrome: Case Report, International Journal of Clinical Case Reports and Reviews, 20(4); DOI:10.31579/2690-4861/606
Copyright: © 2024, Ken Pitetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 November 2024 | Accepted: 02 December 2024 | Published: 14 December 2024
Keywords: malan syndrome; postural control; portable force platform; test-retest reliability
Background
Malan syndrome (MALNS) is an ultra-rare autosomal dominant genetic disorder (< 1/1,000,000 births) identified as an overgrowth syndrome. Recent research has identified new features of MALNS that include high risk of bone fractures in childhood due to osteopenia coupled with an unsteady gait, the latter leading to frequent fall.
Purpose:
To characterize the postural control (PC) of a 16-year-old with Malan syndrome (MALNS).
Methods:
Evaluations involved two, 30-sec trials for each of 6 stances: two-feet eyes open/eyes closed on firm and foam surfaces (total 4); and tandem and one-foot stances, eyes open, on firm. Postural control (PC) was determined by the median velocity (mm/sec) and total pathlength (mm) of the center-of-pressure on a force plate Results were compared to his age and sex matched peers with intellectual disability, Down syndrome, and neurotypical students.
Results:
For the participant with MALNS, significant, moderate test-retest reliability was seen for all 6 stances, and he demonstrated similar PC as his peers with Down syndrome.
Conclusion:
Given that osteopenia, advanced bone aging, hypotonia, and increased risk for bone fractures are commonly associated with MALNS, the outcome of this study should encourage clinicians to evaluate the PC of youth with MALNS.
Malan syndrome (Online Mendelian Inheritance in Man [OMIM] #614753), an ultra-rare autosomal dominant genetic disorder (< 1>
Recent research has identified new features of MALNS that include high risk of bone fractures in childhood due to osteopenia coupled with an unsteady gait, the latter leading to frequent falls.[4] The unsteady gait and frequent falls are thought to be due to hypotonia. The clinical guidelines to manage high recurrence of pathologic fractures, especially of the long bones, only included dual-energy X-ray absorptiometry (DXA) assessment and vitamin D supplements during puberty.[4] Guidelines for evaluating postural control (i.e., balance) in youth with MALNS to determine risk of falling has not been addressed.
Postural control (PC): is the ability to maintain balance during a desired posture or activity; is necessary to achieve, maintain, and restore one’s center of pressure (COP) within a base of support (BoS) while standing;[5,6] and provides the starting point for the successful and safe execution of activities of daily living such as walking and running.[7,8] Main factors contributing to PC consist of the body responding to the sensory input of vision, vestibular (semicircular canals and otolith organs), and somatosensory (proprioception and cutaneous input) information, with motor adjustments that involve coordination of musculoskeletal reflexes to maintain an upright position during standing.[9,10] Evaluation of postural control is relevant to youth with intellectual disability (ID) because it has been demonstrated that they exhibit reduced postural control when compared to their neurotypical (NT) peers.[11-15] Due to the rarity of MALNS, PC has never been studied for this disorder.
There are many commercially available posturographic systems, with many different static and dynamic tests.[16,17] Although posturographic systems have been used to evaluate PC in youth with many types of developmental disabilities, they have not been used to evaluate youth with MALNS. Therefore, the first purpose of this study was to determine the feasibility and reliability of a youth with MALNS performing balance assessments on a force plate.
To properly evaluate the PC, normative data is vital to interpret the results. Usually, comparing PC test results to neurotypical youth assists in determining whether PC anomalies exist. When considering adolescents, normative database should control for sex and age.[18-22] That is, during the maturation process from childhood to adolescence, PC characteristics depend on gender, [14,23] successive periods of ontogenesis (from earliest stage to maturity),[18] and changes in the sensory weighting strategies (vision vs proprioception vs vestibular).[24] In addition, for youth with ID, level of IQ (i.e., severe vs moderate vs mild ID) significantly affects maintenance of balance.[14]
A syndrome with physical characteristics similar to MALNS whose postural control has been studied is Down syndrome. [13,25-28] Down syndrome (DS) is the most common genetic cause of ID and is characterized by the presence of 1 extra copy of human chromosome 21.[29] Characteristics of DS that have also been reported for MALNS include excessive joint range of motion due to joint laxity, [30,31] pronation (flat feet), hypotonia (weak muscle tone), [32,33] and low muscle strength.[34,34] Of importance: 1) it has been demonstrated that joint laxity, pronation, and hypotonia can negatively impact postural stability;[36,37] and 2) youth and young adults with DS have demonstrated suboptimal PC when compared to neurotypical controls.[38,39]
In addition, about 30% to 50
History
The focus of this case report is a 16-year-old male born with Malan syndrome (figures 1 and 3). He was born vaginally with an uncomplicated delivery between 37-40 weeks gestation to non-consanguineous healthy parents after an uneventful pregnancy. In infancy he demonstrated dysmorphic features including macrocephaly, tall forehead, down-slanting eyes, low-set ears, pointed chin, and hypotonia. At 6 months, an MRI showed diffuse mild thinning of white matter including the corpus callosum. He was diagnosed with mild obstructive hydrocephalus, which was corrected surgically at 7 months of age with a ventricular shunt placement and cerebral spinal fluid diversion. He was also prescribed corrective lenses at 6 months due to extensive optic nerve damage (suspected to be related to the hydrocephalus).
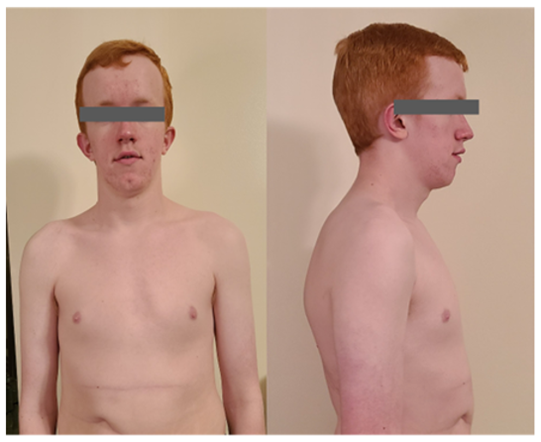
Figure 1: Patient at 16 years and 7 months of age showing elongated face, macrocephaly, and pectus excavatum
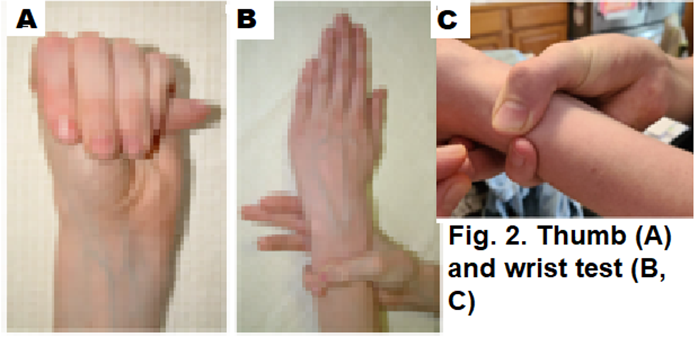
Figure 2: (A)Thumb sign: thumbs extend far beyond edge of their hands; and (B) and (C) Wrist sign: thumb overlaps the fifth finger when grasping the contralateral wrist

Figure 3: Wingspan to height ratio > 1.0. Note that participant is unable to extend arms to their full length due to hypomobility at the elbow joint.
Due to the difference in leg length of 1.9 cm, he underwent distal femur and proximal tibia epiphysiodesis surgery on his left leg at 14 years and 5 months. He wore orthotics and compression shorts as a child in response to hypotonia, and his guardians reported that he is prone to fatigue due to low muscle endurance, even when performing activities he enjoys.
He began using a walker around 20 months, started walking independently at 24 months, and initiated running around 30 months. He used rudimentary sign language to communicate by 24 months and began speaking in short sentences by 3-4 years. At 16 years, he speaks in full sentences; his speech is consistent with developmental milestones expected of a 4-5-year-old. Due to his global developmental delay, he has received speech, occupational, and physical therapy starting at age 1 year. He was enrolled in inclusive education classes within the high school at the time of this study.
Clinical Features
At 16 years and 7 months of age the participant demonstrated macrocephaly, elongated face, and pectus excavatum (Figure 1) and his measurements were: height 190.0 cm (74.8 inch), weight 78.4 kg1(172.8 lbs), with a BMI of 21.7 (healthy BMI). At this time, dysmorphic features included:
Other conditions include mild myopia (near-sightedness); 20/60 OD, 20/30 OS).

Figure 4: Scoliosis is related to uneven leg length (Left leg 2.5 cm longer)
Participants
The male youth (16 yrs) with MALNS was matched in age and sex to 4 students with DS, 5 students with ID but without DS, and 4 neurotypical (NT) students (i.e., without developmental disabilities) for comparative purposes (see table 1 for demographic characteristics). All participants were from the same midwestern, metropolitan area (population ~ 350,000) in the United States and matriculated in school districts that provided inclusive physical educational (PE) classes. That is, all the students were participating in regular PE classes that provided teaching strategies and support systems which encourage students with ID to have the same experiences as their peers who did not have a disability. Intellectual levels (i.e., mild or moderate) of participants with ID with and without DS were classified by school administrators per model of diagnosis by the American Association on Intellectual and Developmental Disability (AAIDD).[46] The participant with MALNS was classified per model of diagnosis by the Wechsler Intelligence Scale for Children.[47] The AAIDD defines persons with mild and moderate ID as IQ ranges of 50 to 70-75 and 35 to 49, respectively.[46] The Wechsler Intelligence Scale for Children characterizes mild and moderate ID and IQ ranges of 55 to 69 and 40 to 54, respectively.[47] The participant with MALNS had an IQ of 50, and IQ’s for the participants with Down Syndrome and ID without Down syndrome ranged from 50 to 65.
The Institutional Review Board of the university associated with this study approved the study prior to active recruitment of participants. For all participants, informed parental consent was acquired before participation in this study. The inclusive criteria for all participants consisted of not having any known acute or chronic musculoskeletal conditions (e.g., cerebral palsy) that would affect evaluation maneuvers.
Procedures and Instruments
Anthropometric variables (standing height in centimeters [cm] and weight in kilograms [Kg]) were measured with participants not wearing shoes by using a stadiometer (Seca 214 Portable Height Rod, Hamburg, Germany) and scale (Health o Meter®Scale, Model #HDM037-01, Boston, MA). Body mass index (BMI) was determined as weight in kilograms divided by height in square meters. Descriptive statistics are found in Table 1.
The PC evaluation was performed during student’s regular physical education (PE) class in a classroom separate from the gymnasium. Postural control was assessed using a portable force platform (AccuSway, Advanced Mechanical Technology Inc. [AMIT], Watertown, MA, USA). Postural data were acquired and recorded using Balance Clinic software version 2.03.00(AMTI) loaded on a Dell laptop. The acquisition sampling frequency was set at 1000 Hz and was filtered using a fourth-order zero phase Butterworth low-pass filter with a cut-off frequency of 10 Hz.[48] The force platform records the position of a participant’s center of pressure (COP). In an upright standing position, all individuals sway naturally in the antero-posterior and lateral directions, with the resulting shifts of COP providing an index of a participant’s ability to maintain balance.
Six (6) test conditions were used to assess PC: two visions (EO vs EC) and two surface conditions (firm vs foam) for two- foot stance (2FT; total of four stances, Figures 5A and B); tandem EO (TD, EO; Figure 5 C) and one-foot EO (1FT, EO; Figure 5 D) on firm.
In the two-foot stance, participants either stood directly on the force platform (Firm surface; Figure 5 A) or on a 30 x 41 x 6 cm foam (Figure 5 B; Airex® Balance Pad, Airex AG, Sins, Switzerland) placed on top of the force platform (foam surface). The big toes (hallux) of both feet were positioned on a tape that ran perpendicular to the plate (see figure 5 A), with the distance between the feet (i.e., intermalleolar distance) was approximately shoulder width and the angle of the feet selected by the participants. That is, in the two-foot stance, participants were allowed to select the distance between feet and angle of feet, since it has been demonstrated that constraining participants’ feet orientation results is greater sway.[49]
For the one-foot, eyes open, standing on the platform (1FT/EO/firm) stance, the foot was placed on tape extending through the middle of the pressure plate (figure 5 D). To determine the supporting leg, participants were asked what foot they would use to kick a soccer ball. The nonsupporting leg was flexed 30º to 90ºat knee level and participants were instructed not to allow the non-supporting leg to make contact with the supporting leg.
During the tandem, eyes open, standing on the platform (TD/EO/firm) the toe of the trail foot was placed in contact with the heel of the lead foot with both feet placed on the tape running through the middle of the force plate (figure 5 C). For the tandem stance, the lead extremity was chosen by the participant. The participants were tested in a single session, which lasted approximately 50 minutes.
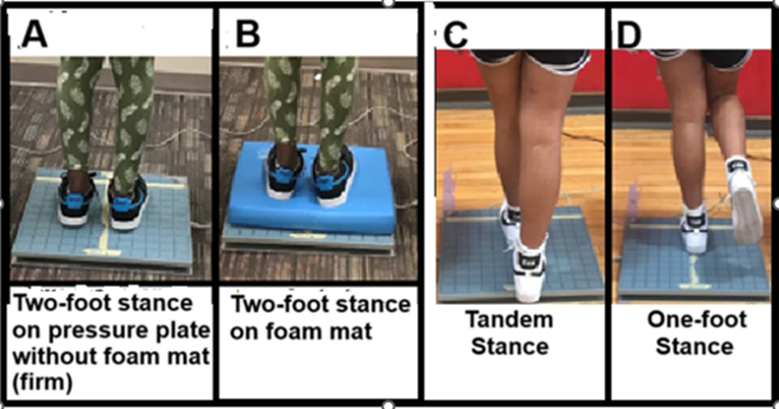
Figure 5: (A) Two feet stance on pressure plate without foam mat (firm); (B) Two feet stance on pressure plate with foam mat; (C) Tandem stance on pressure plate, feet aligned heel-to-toe; and (D) One-foot stance with non-supporting leg flexed 30º to 90ºat knee level
Force plate data was collected from two blocks of testing. Each block consisted of 6 consecutive 30-s trials in each stance, yielding 12 trials. In the first block, the order of the six stances was randomized and the sequence was reversed in the second block. During testing, participants stood in their normal physical education class footwear (e.g., tennis shoes) and were encouraged to stand as still as possible throughout the 30-sec trial. Participants sat for 60-90-s between trials. When vision was allowed, participants were instructed to look straight ahead at the X marked in tape at approximately eye level on a wall 1.5 m away. For all participants with ID, when vision was not allowed, a staff member stood directly in front of the participants, repeating “keep your eyes closed…keep your eyes closed”, and ensuring that the eyes were closed throughout the 30 second trial. Ankle or hip (‘ankle strategy’ or ‘hip strategy’) sway, which is commonly described as fix-support (COP is moving but feet remain in contact with the floor) was allowed.[50] Arm movement was also allowed. Some participants ‘lost the stance’ during the one foot and tandem stances. In these cases, participants were asked to regain stance as quickly as possible and continue the trial. The loss of stance segment(s) of the 30-second trial was(were) visually identified while the start and stop times (using a stopwatch) were recorded. The data from the ‘out of stance’ segment(s) of the 30-second trial were removed and not used in calculation of postural parameters.
Median velocity (MVelocity, mm/sec) and pathlength (mm) were calculated using the R median function.[51] Median velocity (MVelocity) and pathlength have been identified as two of the most reliable parameters when determining PC capacity.[52] The literature states that smaller values of MVelocity and pathlength imply better balance. That is, the higher the MVelocity, the more net neuromuscular activity is needed to keep stance.[53] In addition, MVelocity has been demonstrated to have the greatest reliability among trials [54] and is considered the most sensitive parameter in comparing individuals with different neurological conditions.[55,56] Pathlength is a proxy for postural sway magnitude whereby the smaller the total pathlength the less the postural sway and, therefore, the better the individual’s postural control.[57] However, the greater the static sway (i.e., greater pathlength) the higher the probability of swaying during walking resulting in an increased risk of falls and injuries.[58] Of the two trials, the lowest scores for MVeloscity and pathlength were chosen for data analysis.
All evaluations were proctored by the lead author to insure proper measurements. Participants had the stances demonstrated to them; then they practiced the six stances, especially the one foot and tandem stances, until they were familiar with the positioning of the feet and the concept of holding the stance for 30 seconds. The familiarization/practice period lasted for approximately 10 minutes for the neurotypical (NT) participants and 15 to 20 minutes for the participants with ID which included the participant with MALNS. Immediately following the familiarization/practice period the participants performed the tests.
Means and standard deviations were determined for demographics, MVelocity (mm/sec), and path length (mm) statistics for the participants.
To determine test-retest reliability for the participant with MALNS, normality of test scores for MVelocity, pathlength (mm), and time in stance were determined using a Kolmogorov-Smirnov test. This test confirmed that the distributions of these variables were not normally distributed. Therefore, the nonparametric Kendall’s Tau (τ) correlation coefficient was used to assess the strength of the relationship between Trial 1 and Trial 2 for the MVelocity, pathlength (mm), and time in stance for the participant with MALNS.
Interpretation of Kendall’s Tau correlation coefficients is based on previous recommendations[59-61] with 0.00 to ±0.19 to be very weak to negligible, ±0.2 to ±0.39 to be weak to low correlation, ±0.4 to ±0.69 to be moderate correlation, ±0.7 to ±0.89 to be strong to high correlation, and ±0.9 to ±1.0 to be very strong to very high correlation.
Statistics were not used to compare the MVelocity (mm/sec) and pathlength (mm) of the participant with MALNS to the other three groups of participants (i.e., with DS, with ID without DS, and NT) because summary statistics cannot be performed on one data point. A ratio was calculated between the MVelocity and pathlength for the individual with MALNS and the mean of the MVelocity and pathlength for each of the three groups.
Means and standard deviations for demographics are found in table 1. The participant with MALNS was more than 3 standard deviations taller than other 3 groups. Correspondingly, the participant with MALNS demonstrated a BMI classified as healthy weight as opposed to participants with DS and ID without DS being classified as obese and overweight, respectively.[62] The mean BMI for NT participants were in the healthy range.[62]
For the participant with MALNS, significant, moderate test-retest reliabilities were seen for MVelocity (τ = 0.601; p = 0.037), pathlength (τ = 0.690; p = 0.017), and time in stance (τ = 0.778; p =0.014) for all 6 stances (Table 2).
When comparing MVelocity, whereby the smaller the value the better PC, of the participant with MALNS to the mean of the MVelocity for the other groups, the participant with MALNS demonstrated (see Table 3):
When comparing pathlength (mm) of the four 2FT stances, whereby the smaller the pathlength the better PC, the participant with MALNS pathlength was (see Table 4):
For the pathlength, comparisons for tandem and 1FT stances could not be made due to differences in ‘time in stance’; that is, pathlength is strongly correlated to time in stance.
| Malan (n=1) | Down Syndrome (n=4) | Intellectual Disability without Down syndrome (n=5) | Neurotypical (n=5) | |
| Sex | MALE | MALE | MALE | MALE |
| Age (years) | 16 | 16±1 | 16.5±0.4 | 16.0±0.8 |
| Body height (cm) | 190.4 | 159.4±3.5 | 171.5±4.1 | 175.1±5.3 |
| Body mass (Kg) | 78.9 | 85.3±35.8 | 73.1±9.9 | 73.1±21.9 |
| BMI (kg/m2) | 21.8 | 33.9±28.6 | 24.9±4.1 | 23.8 |
Table 1: Descriptive Statistics
| Stance | MVelocity mm/sec | Path Length (mm) | Out of Stance (sec) | |||
| Stance | Trial 1 | Trial 2 | Trial 1 | Trial 2 | Trial 1 | Trial 2 |
| 2FT, Eyes Open, Firm | 26.5 | 48.1 | 791.5 | 275.8 | 0 | 0 |
| 2FT, Eyes Closed, Firm | 26.3 | 28.6 | 794.4 | 877.2 | 0 | 0 |
| 2FT, Eyes Open, Foam | 45.8 | 44.1 | 925.6 | 894.3 | 0 | 0 |
| 2FT, Eyes Closed,Foam | 42.8 | 48.7 | 1307.0 | 1448.3 | 0 | 0 |
| 1FT, Eyes Open, Firm | 60.9 | 53.2 | 1307.0 | 1226.2 | 12.6 | 10.5 |
| Tandem, Eyes open, firm | 58.7 | 63.7 | 1451.3 | 1161 | 8.7 | 15.3 |
| Means | 43.5 ±13.7 | 47.7 ±10.5 | 1096.1 ±267.1 | 980.5 ±371.1 | 3.6±5.1 | 7.6±8.1 |
Kendall’s Tau for MVelocity (mm/sec): τ = 0.601; p = 0.037
Kendall’s Tau for Pathlength (mm): τ = 0.690; p = 0.017
Kendall’s Tau for Time out of stance (secs) τ =0.289; p = 0.408
Table 2: Kendall’s Tau Correlation Between Trials for MVelocity (mm/sec), Pathlength (mm) and Time of Stance
| Participants | 2FEO Firm | 2FEC Firm | 2FEO Foam | 2FEC Foam | TDEO Firm | 1FTEO Firm |
| Malan n=1 | 26.0 | 26.6 | 29.0 | 42.8 | 63.8 | 53.2 |
| DS n=4 | 16.7±5.6 | 24.5±8.6 | 29.3±7.9 | 52.7±9.6 | 62.4±15.0 | 87.1±12.7 |
| ID n=5 | 16.1±5.6 | 15.3±5.3 | 16.9±6.5 | 26.5±5.2 | 35.2±5.3 | 49.8±12.6 |
| NT n=5 | 8.6±0.7 | 10.5± 1.2 | 10.2±1.1 | 17.7±2.6 | 20.6±1.0 | 26.0±4.5 |
EO = Eyes open; EC = Eyes closed; 2F = Two-foot stance, 1F= One-foot stance, TD=Tandem stance; Firm=standing directly on pressure plate, Foam = standing on foam mat over pressure plate
Malan = participant with Malan syndrome; DS = Down syndrome; ID = Intellectually disabled without DS; NT = Neurotypical.
Table 3: Mean of the Median Velocity (MVelocity, mm/sec) of Center of Pressure (COP) for all Six Stances
2FEO Firm | 2FEC Firm | 2FEO Foam | 2FEC Foam | TDEO Firm | 1FTEO Firm | |
Malan n=1 | 791.6 | 502.7 | 884.3 | 1352 | 2122.7 <22s> | 1307 (12s) <20> |
DS n=4 | 540.7±174.4 | 781.6±244.9 | 980.2±302.7 | 1771.6±310.1
| 1858.2±454.6 | 1950±241.9 |
ID n=5 | 569±218.1 | 590.9±201.1 | 577.2±249.3 | 819.4±196 | 1186±222 | 1556.1±399 |
NT n=5 | 269.7±25.2 | 332.4±81.6 | 309.1±44.9 | 557.2±99.4
| 635.8±42.2 | 1950±241.9 |
EO = Eyes open; EC = Eyes closed; 2F = Two-foot stance, 1F= One-foot stance, TD=Tandem stance; Firm=standing directly on pressure plate, Foam = standing on foam mat over pressure plate
Malan = participant with Malan syndrome; DS = Down syndrome; ID = Intellectually disabled without DS; NT = Neurotypical.
Table 4: Mean of Pathlength (mm) of Center of Pressure (COP) for Six Stances
Malan syndrome was first described in 2010 by Dr. Valarie Malan and, as of 2022, less than 90 patients have been differentially diagnosed. Therefore, for this ultrarare syndrome, limited clinical information exists which would provide guidelines for management of evolutive complications. Given that osteopenia, advanced bone aging, hypotonia, and increased risk for bone fractures are medical problems commonly associated with MALNS, [1-4] a possible evolutive complication would be poor postural control (PC) resulting in increased risk of falling. The result of this study demonstrated that evaluating the PC of a youth with MALNS on a portable force platform was feasible, and the test data produced in the two trials for the six stances was moderately, and significantly reliable.
The integration of visual, somatosensory, and vestibular components plays a leading role in maintenance of stable vertical posture,[9,10] and the consolidation of these components reaches adult level at approximately the age of 12 years.[63,64] The visual system is considered a primary sensory system especially in children and adolescents, and it is suggested that input from the visual system principally decreases sensitivity to sensory information from the two remaining systems.[65] Figure 5 A, with EO, is a “standard” or “base” test condition where all three sensory systems are available to help in sustaining balance. Therefore, the smallest amount of postural sway (i.e., lowest MVelocity and shortest pathlength) is expected when compared to the other five stances. Such was the case for the participant with MALNS and all three groups (see Tables 3 and 4).
In the stance depicted in figure 5 A, with eyes closed, visual feedback is eliminated, and this stance increases the reliance on proprioceptive and vestibular systems. Since balance and PC relies on proprioception more than the vestibular system, this condition largely measures the proprioceptive contribution to balance.[66] For the participant with MALNS, only a slight increase in median velocity (MVelocity) (table 3) and a reduction (rather than increase) in pathlength (table 4) was seen, indicating that the proprioceptive system (i.e., dorsal column-medial lemniscus tract) was intact. For both MVelocity and mean pathlength, participants with DS and NT demonstrate a greater reliance on vision, which compliments what has been demonstrated in the literature, [12,13,67] while participants with ID without DS demonstrate similar responses as the participant with MALNS.
In the stance depicted in figure 4 B, with eyes open, the visual and vestibular systems are available, but the proprioceptive system is challenged by having the participant stand on a compliant foam surface. In this stance the visual system is assessed given its preference over vestibular feedback for balance. Given the optic nerve damage and mild myopia for the participant with MALNS, the possibility existed that a greater reliance on proprioception rather than vision would be evident. However, for the participant with MALNS, as well as the participants with ID without DS, only a slight increase in MVelocity and moderate increases in mean total pathlength are seen when compared to 2FEOfirm (tables 3 and 4). The latter suggest that vision plays an equal role with proprioception feedback for PC for these participants. Participants with DS and NT participants demonstrate much higher MVelocity and mean total pathlength increases when compared to 2FEOfirm. The later results, poorer PC with eyes closed, again complement the literature. [11,68-72]
In the stance depicted in Figure 10 B with eyes closed on foam, the visual and proprioceptive systems are challenged, moving the dependency of PC to the vestibular system as the primary sensory source used to maintain balance. As expected, given that vision and proprioception have preference over vestibular feedback for balance, the greatest increases in MVelocity and pathlength were seen for the participant with MALNS and all three participant groups, indicating a low reliance on the vestibular system for PC.
In the two-foot stance (Figure 5 A) the medial-lateral base of support (BOS) is twice as large as the single-legged and tandem stances. In healthy, physically able youth, this stance will produce the most stable PC. In the tandem stance (figure 5 C) the anterior/posterior(A/P) BOS is larger than in 2-FT and 1FT stances, but the base of support diminishes substantially in the medio-lateral direction. This posture is often used during clinical balance evaluations in order to predict a patient’s risk of falling under demanding postural conditions that challenges the medio-lateral limits of stability.[73] Specifically, this stance tests the ability of the tibialis anterior, soleus, and peroneus longus of both legs to keep the COP within the narrow base width.[74] For all three groups, this stance produced the second highest mean of the MVelocity of the six stances, which is consistent with the literature[11,68] For the participant with MALNS, the MVelocity in the tandem stance was the highest of the 6 stances. The later result could have been due to the participant’s uneven leg length. That is, in the tandem stance, the participant with MALNS employed his right leg as the lead leg. The left leg, the trialing leg, was 1.9 cm longer, might have added an increase challenge to PC in the anterior-posterior direction.
The single-leg stance (IFT)(figure 5 D) introduces an additional challenge to the postural-control system by reducing the base of support thus demanding more adjustments to prevent loss of stance.[75] This stance is essential during daily living activities as a single task as well as a component of other more complex tasks. In clinical practice it is widely used as a testing task because it helps quantify balance deficits of the single limb otherwise concealed during the performance of double limb tasks.[75,76] It is likewise used to assess risk of falls.[77] Single-leg balance involves ankle stabilizers (peroneal muscles, tibialis anterior, and tibialis posterior muscles), lower leg muscles (gastrocnemius and soleus), and muscles to stabilize the knee (vastis lateralis, rectus femoris) and hip (gluteus muscles). Although the MVelocity of the participant with MALNS was much higher than NT participants, it was less than and similar to participants with DS and ID without DS, respectively. This suggests that the PC of the single-leg stance for the participant with MALNS was comparable to his peers with ID.
Whether or not the results of the participant with MALNS in this study are representative of the PC of youth with MALNS is currently unknown. It is hopeful that the outcome of this study will encourage other clinicians to report the PC of youth with MALNS using a pressure plate given their associated risk of falls.
We would like to thank the administrators, faculty, and staff of the Derby middle schools and high school, Derby, Kansas, for their assistance in conducting this research. We especially wish to thank the family of the participant with Malan syndrome for allowing us to report on a very special child in their lives.
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in writing of the manuscript, and in the decision to publish the results.
No funding was secured for this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
