
Research Article | DOI: https://doi.org/10.31579/2692-9759/066
1 Department of Medicine, Faculty of Medicine and Health Sciences, Nile Valley University, Atbara, Sudan.
2 Department of Medical Microbiology, Faculty of Medical Laboratory Sciences, Shendi University, Sudan.
3 Head of Parasitology Department, College of Health and Allied Sciences, St. Joseph University in Tanzania, Dar Es Salaam, Tanzania.
*Corresponding Author: Mosab Nouraldein Mohammed Hamad, Head of Parasitology Department, College of Health and Allied Sciences, St. Joseph University in Tanzania, Dar Es Salaam, Tanzania.
Citation: Tarig M A Mohamed, Ghanem M Mahjaf, Mosab N Mohammed Hamad*. (2022). E Evaluate the adequacy of Warfarin Treatment Among Patients who were on long term Anticoagulation Therapy in Ahmed Gasim Cardiac Center, Khartoum- Sudan. Cardiology Research and Reports. 4(6); DOI: 10.31579/2692-9759/066
Copyright: © 2022 Mosab Nouraldein Mohammed Hamad,This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 June 2022 | Accepted: 12 June 2022 | Published: 17 July 2022
Keywords: warfarin; adequacy; anticoagulation; therapy; khartoum, Sudan.
Warfarin therapy for the prevention and treatment of thromboembolic diseases is safe and effective when it is maintained with a narrow therapeutic window measured by the international normalization ratio (I.N.R).Failure to provide adequate anticoagulation consistently predict thromboembolic events( eg stroke and pulmonary embolism), while excessively anticoagulated patients were at risk of bleeding. The management of therapy within this narrow window is complicated by numerous factors including drug interaction, comorbid acute, and chronic diseases, diet, and a variety of patient responses to warfarin therapy. The study was conducted in Ahmed Gasim cardiac center outpatient anticoagulation clinic. The study was carried out in the period from January to December 2012. Patients admitted or attending Ahmed Gasim cardiac center for follow-up of their long-term anticoagulation therapy. From all these results during the follow-up period. We found the percentage of those who were adequately controlled at the normal therapeutic I.N.R range was (54.7%) versus (45.3%) for uncontrolled patients. Of those who were controlled, we found(133) patients (60.7%) of them were fully educated about the interaction between diet and medications, while (31) patients (38.3%) were not receiving education about such interaction. On the other hand, those who were not controlled according to their therapeutic I.N.R (50) patients (61.7%) were not having educated and (86) patients (39.7%) were educated and have knowledge about dietary and drug interaction. P-value (0.01).The study of the adequacy of anticoagulation shows suboptimal control in (45.3%) of patients on patients attending INR clinics, however, the adequacy varies with age group with elderly patients poorly anticoagulated. Finally, the overall research conclude that the adequacy of anticoagulation was suboptimal with (54.6%) adequately controlled versus (45.3%) uncontrolled. In conclusion, the INR range of anticoagulation at the referral clinic mostly falls in the “under anticoagulated range”. Areas to be considered are patient attendance, staffing and at the same time increasing the efficiency of services. Improvement should be directed not only toward attaining better patient attendance at the clinic but also to educate patients on the importance of adequate control.
Warfarin therapy for the prevention and treatment of thromboembolic diseases is safe and effective when it is maintained with a narrow therapeutic window measured by the international normalization ratio (I.N.R).Failure to provide adequate anticoagulation consistently predict thromboembolic events( eg stroke and pulmonary embolism), while excessively anticoagulated patients were at risk of bleeding. The management of therapy within this narrow window is complicated by numerous factors including drug interaction, comorbid acute, and chronic diseases, diet, and variety of patient responses to warfarin therapy [1]. The integrity of the circulation is maintained by blood flowing through intact vessels lined by endothelial cells. Injury to the vessel wall exposes collagen and together with tissue injury sets in motion a series of events leading to homeostasis [2]. Hemostasis is a complex process depending on interactions between the vessel wall, platelets, and coagulation, and fibrinolytic mechanisms[2].
Platelet adhesion:- When the vessel wall is damaged, the escaping platelets come into contact with and adhere to collagen and the von Will brand factor that is bound below the endothelium. This is mediated through glycoprotein Ib (GPIb) Glycoprotein IIb–IIIa is then exposed, forming a second binding site for VWF. Within seconds of adhesion to the vessel wall platelets begin to change shape, from a disc to a sphere, spread along the subendothelium, and release the contents of their cytoplasmic granules, i.e. the dense bodies (containing ADP and serotonin) and -granules containing platelet-derived growth factor, thrombomodulin, fibrinogen, VWF, fibronectin, thrombospondin, and other factors) [2]. Platelet release:- The release of ADP leads to a conformational change in the fibrinogen receptor, the glycoprotein IIb–IIIa complex (GPIIb–IIIa), on the surfaces of adherent platelets allowing it to bind to fibrinogen. Platelet aggregation:- As fibrinogen is a dimer it can form a direct bridge between platelets and so binds platelets into activated aggregates (platelet aggregation) and further platelet release of ADP occurs. A self-perpetuating cycle of events is set up leading to the formation of a platelet plug at the site of the injury. Coagulation:- After platelet aggregation and release of ADP, the exposed platelet membrane phospholipids are available for the assembly of coagulation factor enzyme complexes (tenase and prothrombinase); this platelet phospholipid activity has been called platelet factor 3[2,3].
There is both parenteral and oral anticoagulant currently the parenteral anticoagulant include heparin and low molecular weight heparin and the oral anticoagulant vitamin K antagonist warfarin. For long-term chronic management, oral anticoagulation is preferred over the intravenous or subcutaneous routes due to patient convenience and cost. Warfarin has been in clinical use for over six decades and it is still one of the most widely used oral anticoagulant agents. Warfarin and other vitamin K antagonists (VKAs, eg, acenocoumarol, phenprocoumon, fluindione) are the standard oral anticoagulants used in a variety of clinical settings[4].
Commercially-available warfarin is a racemic mixture of S and R enantiomers. The more potent S form of the drug is metabolized primarily by the CYP2C9 hepatic microsomal enzyme system. This enzyme system is inducible by many drugs and has several genetic variants, both of which may profoundly alter warfarin in vivo activity. Warfarin is strongly protein-bound, primarily to albumin; only the non-protein-bound fraction is biologically active. Accordingly, any agent that is also bound to albumin may displace warfarin from its albumin binding sites and increase its biological activity. Warfarin is water-soluble and completely absorbed after oral administration. The majority of the drug is absorbed in the proximal small bowel, although successful use of the sublingual route has been described in two patients. Excretion is via the urine, primarily as drug metabolites. The long half-life of 20 - 60 hours. The mean half-life is approximately 40 hours. The duration of effect is 2 - 5 days. The maximum effect of a dose occurs up to 48 hours after administration and the effect lasts for the next 5 days. Steady State requires 5-7 days [4].
The anticoagulant effect of warfarin is mediated through inhibition of the vitamin K-dependent gamma-carboxylation of coagulation factors II, VII, IX, and X [4]. This effect of warfarin results in the synthesis of immunologically detectable but biologically inactive forms of these coagulation proteins. Warfarin also inhibits the vitamin K-dependent gamma-carboxylation of proteins C and S, which have anticoagulant properties through their inhibition of activated factors VIII and V [4]. Because of these competing effects, vitamin K antagonists such as warfarin create a biochemical paradox by producing an anticoagulant effect due to the inhibition of procoagulants (factors II, VII, IX, and X) and a potentially thrombogenic effect by impairing the synthesis of naturally occurring inhibitors of coagulation (proteins C and S). The ultimate anticoagulant effect of warfarin is delayed until the normal clotting factors, especially prothrombin, are cleared from the circulation. The peak effect does not occur until 36 to 72 hours after drug administration, especially because the plasma half-life of factor II (prothrombin) is approximately 3 days During the first few days of warfarin therapy, prolongation of the prothrombin time mainly reflects its action on the extrinsic coagulation pathway, through the depression of factor VII, which has a half-life of four to six hours. The other vitamin K-dependent factors within the common and intrinsic coagulation pathways (i.e., factors II, IX, and X) remain relatively unchanged during the first few days. Accordingly, the patient is not fully anticoagulated with warfarin until these other components are also reduced[5].
Equilibrium levels of factors II (prothrombin), IX, and X, approximately 10 to 35 percent of normal at therapeutic INR levels (11), are reached about one week after the initiation of therapy. For this reason, parenteral anticoagulants and warfarin should OVERLAP by four to five days when warfarin is initiated in patients with the acute thrombotic disease (eg, venous thromboembolism, heparin-induced thrombocytopenia) [5].
Many medicines can interact with anticoagulants. Some medicines can increase the effect of anticoagulants, thus increasing the chances of bleeding. Some medications can decrease the effect of anticoagulants, thus increasing the chances of blood clots[6].
Polymorphisms in the genes for the following two enzymes have been associated with altered sensitivity to warfarin [7].
Hepatic cytochrome P-450 2C9 (CYP2C9), is involved in the metabolic clearance of warfarin. Vitamin K epoxide reeducates complex 1 (VKORC1), which recycles vitamin K and is required for gamma-carboxylation of vitamin K-dependent coagulation factors. Cytochrome P-450 2C9 -A well-studied cause for individuality in patient responses to warfarin is the presence of genetic variation (polymorphisms) in the hepatic cytochrome P-450 2C9 (CYP2C9) isoenzyme, which inactivates both warfarin and acenocoumarol[8,9].
Study design:
Retrospective and prospective observational hospital-based study.
Study area and time:
The study was conducted in Ahmed Gasim cardiac center outpatient anticoagulation clinic. The study was carried out in the period from January to December 2012.
Study population:
Patients admitted or attending Ahmed Gasim cardiac center for follow-up of their long-term anticoagulation therapy. Ahmed Gasim center is the cardiac center which is a treachery hospital in North Khartoum for surgical and medical treatment of cardiac problems.
Study sample:
A sample size of 300 patients was studied.
Inclusion criteria:
Patients who were on long-term anticoagulant therapy for more than three months.
Exclusion criteria:
Interrupted or stopped for any reason oral anticoagulant medication. Patients who were treated with medication other than oral anticoagulant therapy e.g., antiplatelet tablet, or those on heparin treatment alone. Period of anticoagulation less than 3 months duration.
Data collection:
Personal and demographic data from all patients are collected using a direct questionnaire (attached)including the indication for anticoagulation, the frequency of follow up
Main outcome measure:
The percentage of international normalized ratio (I.N.R) tested below, within, and above the therapeutic range were determined. The patient was classified as adequately anticoagulated if the measured INR was within the therapeutic range for the indicative cause of anticoagulation. On the other hand, the patients were regarded as over anticoagulated or under-coagulated if the measured result of INR lagged by (0.5) above and below the therapeutic range respectively. In addition, the quality of education given to the patient at the start of using anticoagulant therapy was assessed, together with the frequency of bleeding and other complication encountered.
Data processing:
Collected data from the forms entered into a computer at the end of the study and analyzed using the software program SPSS v16. The means, standard deviations, and frequencies were defined. The correlation between the patient's anticoagulation measures to the targeting I.N.R is tested using a chi-square test. The difference between means is tested using an independent t-test. P-value >0.05 is said to be significant.
Ethical consideration &clearance:
Verbal consent was taken from all patients after explanation of the study, Ethical clearance from the authorities is taken before the start of the study.
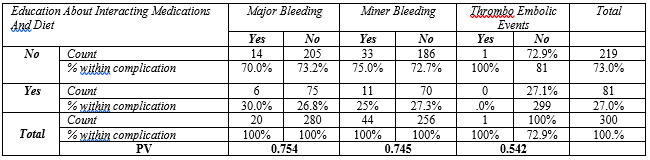
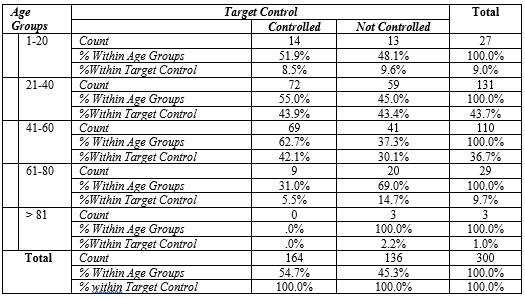
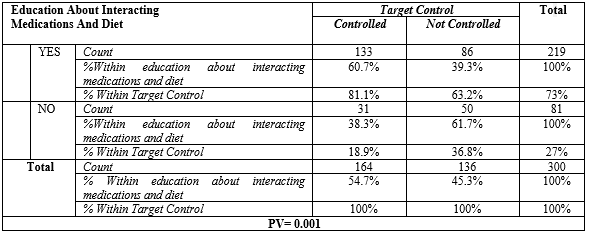
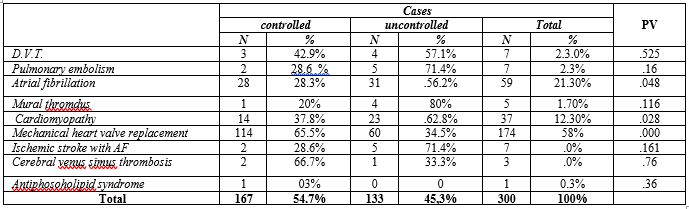
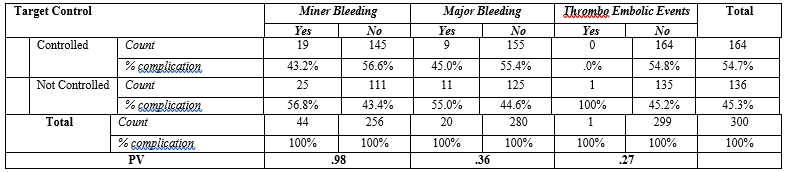
During the study period (300) patients were enrolled, among them (193) were females (64.33 %) and (107) were males (35.67%). The majority of patients (131) ( 43.7%) were between the age of (21-40) years followed by (110) patients (37.6%) aged between (41-60) years. There were (29 ) patients (9.7%) between (61-80 ) years, (27) patients (9% ) at age less than 20 years and (3) patients (1%) < 80>P-value of (0.75). For patients who develop minor bleeding (33)patients(75%)were not educated (11)patients (25%) were educated P-value (0.74). We found only one patient who develop a thromboembolic event (stroke) who was anticoagulated for prosthetic valve and was not fully educated (Table1). According to age group, all elderly patients above 80 years (3) patients were uncontrolled. In patients between (61-8o) age group (20) patients (69%) were uncontrolled versus (9) patients (31%) who were controlled. On the other hand, for patients aged (41-60), most of the patients (69) patients (62.7%) were adequately controlled versus (41) patients (37.3%) uncontrolled. In patients in (the 21-40) age group which pick the majority of patients studied we found (72) patients (55%) controlled versus (59) patients (45%) uncontrolled. In patients in (1-20 )age group we found (14) patients (51.9%) controlled versus (13) patients (48.1%) uncontrolled .P value (0.001) (Table2). In this study, 300 patients were followed for three consecutive follow-ups, during each follow up their results of I.N.R were recorded. During the first visit, we found (151) patients (50.3%)within the normal therapeutic I.N.R, while( 92) patients (30.7%) were having lower than normal therapeutic I.N.R. and (57) patients (19%) having higher than therapeutic I.N.R. In the second visit there were (169) patients(56.3%) have resulted within normal therapeutic I.N.R, while (81) patients(27%) were having lower than normal therapeutic I.N.R and (50) patients (16.7%) having higher than normal therapeutic I.N.R . In the third visit there were (176) patients(58.7%) have resulted within the normal I.N.R, while (77) patients(25.7%) were having lower than normal therapeutic I.N.R and (47) patients(15.7%) having higher than normal therapeutic I.N.R (15.7%). Regarding the clinical indication of anticoagulation we found that in patients with mechanical valve replacement, the percentage of controlled I.N.R is higher (65.5%) versus those uncontrolled (34.5%). On the other hand, the percentage of uncontrolled patients was high among those anticoagulated because of cardiomyopathy (62.8%) while only (28.3%) were adequately controlled .also in patients with pulmonary embolism (71.4%) were uncontrolled versus (28.6%) of controlled one. In patients with D.V.T, there were (57.1%) uncontrolled versus (42.9%) controlled. The uncontrolled patients predominate over-controlled ones in patients with atrial fibrillation (56.2%) versus (28.3%). From all these results during the follow-up period. We found the percentage of those who were adequately controlled at the normal therapeutic I.N.R range was (54.7%) versus (45.3%) for uncontrolled patients.Of those who were controlled, we found(133) patients (60.7%) of them were fully educated about the interaction between diet and medications, while (31) patients (38.3%) were not receiving education about such interaction. On the other hand, those who were not controlled according to their therapeutic I.N.R (50) patients (61.7%) were not having educated and (86) patients (39.7%) were educated and have knowledge about dietary and drug interaction. P-value (0.01)(Table3). Regarding the effect of the adequacy of INR control on patients who develop complications during the period of follow up, we found that the percentage of complications of major bleeding was increased in patients with inadequate INR control (55%) versus (45%) with adequately controlled I.N.R. P-value (0.36) (Table4). Also the percentage of minor bleeding was increased in patients with inadequate I.N.R (56.8%) versus (43.2%) with adequately controlled I.N.R P-value (0.98). On the other hand, the only one patient who developed a thromboembolic event during the follow-up was found an inadequate INR control P-value (0.27).(Table5).
anticoagulation control during initiation and maintenance of warfarin treatment is generally unsatisfactory. Compared to a study conducted in 2008 in Canada about the quality of anticoagulation in long term care, where (107) patients who were receiving warfarin (72%) of them were female with a mean age of( 65—90 years) (89), Our study also shows female predominance (64.3%) but with younger mean age (mean range 20—40 years). The main indications of anticoagulation were stroke prophylaxis for atrial fibrillation (67%) followed by DVT (18%). While in our study anticoagulation for mechanical valve replacement predominate (58%) followed by anticoagulation for atrial fibrillation (21%). The difference in the predominant age group and the incidence of being mostly in the young age group with anticoagulation for the prosthetic valve is related to the high prevalence of rheumatic heart disease among the young age group in Sudan and hence increase in the rate of prosthetic valve intervention for destructed valves due to R.H.D. During the study period in that research, it is found that the overall result was suboptimal anticoagulation with an INR result (54%) in the therapeutic range while in (46%) was subtherapeutic. This result was similar in range to the suboptimal therapeutic INR result found in our study (54.7%) controlled versus (45.3%) uncontrolled INR. A similar range of results indicates that it is related to facilities other than the presence of well-equipped centers for follow up which is different from our overcrowded small center .it is related to the patient's compliance and education about medication of anticoagulation. In another study conducted in Alberta hospital in Canada about the adequacy of anticoagulation in patients with A.F, Of (375) patients taking warfarin coming to the hospital and having an INR documented in the clinic,( 167) patients (44.5%) were subtherapeutic, (137) patients (36.5%) were therapeutically controlled, and (71) patients (18.9%) were supra therapeutic [10]. In our study of (300) patients taking warfarin, the INR results reveal (that 151) patients (50.3%) were therapeutically controlled, and (92) patients (30.7%) were sub-therapeutic and (57) patients (19%) were supra therapeutic. In a study conducted in Africa in Tanzania, about the adequacy of anticoagulation among patients with MVR, it. is found that only (35.5%) of the measurements were within the recommended therapeutic (normal) range, (33.4%) above therapeutic, and (31.1%) below it [11]. Our study shows a much better percentage in patients with MVR (65.5%) controlled versus (34.5%) uncontrolled. table (3.4). In our study( 65) patients from(300) patients develop complication,(44) patients(14.7%) develop minor bleeding ,while (20) patients(6.7%) develop major bleeding and in one patient(0.3%) thromboembolic event was encountered. In another study conducted in South Africa, It is found that in studying (309) patients there were( 50 ) episodes of complications encountered following anticoagulation after MVR(16.2%), (38) bleeding events with (30) patients(9.7%) develop minor bleeding, and,( 8) patients (2.6%) develop a major bleeding complication. there were also (12) patients(3.1%) who get a thromboembolic complication[13]. In a meta-analysis study of (45) studies conducted in the U.S about hemorrhagic and thromboembolic complications in patients on long term anticoagulation control, it is found that(23) reported both hemorrhages and thromboembolic; (14) that reported hemorrhages only; and( 8) thromboembolic only) involving a median of 208 patients. Of these studies, (64%) were conducted at community practices; the remainder were at anticoagulation clinics. About (69%) of the studies were classed as having moderate or high quality. Overall,( 44%) of hemorrhages occurred when INRs were above the therapeutic range, and (48%) of thromboembolic took place when below it [14]. The involvement of patients in the management of anticoagulation therapy was studied in some trials. It was found that patient awareness of the INR values correlated with improved accuracy of anticoagulation control[15]. Our study confirms these data. The patients who had received satisfactory education on anticoagulation had the highest quality of anticoagulation and were less prone to complications. Our study has some limitations including a limited sample size, we conducted the study at a single center, thereby potentially limiting the ability to generalize our data, limiting our ability to explore additional factors that may have contributed to sub-optimal INR such as acute co-morbidities and variability in dietary vitamin K intake One of the most important findings of our study was the significance of the patient’s knowledge about anticoagulation. Patient education is generally performed by the medical staff and includes the purposes of anticoagulation, risk of complications, and information about INR values. The poor quality of such education was the most significant risk factor for complications and the ineffectiveness of anticoagulation. Moreover, insufficient education was more devastating than the total lack of education. Low-quality education resulted in the highest rate of bleeding complications and over coagulation. Poor education on anticoagulation was the most reliable risk factor for adverse outcomes in our study. P-value (0.001). Limitations of the study were that it was not an intervention trial and that the education process was not standardized.
The study of the adequacy of anticoagulation shows suboptimal control in (45.3%) of patients on patients attending INR clinics, however, the adequacy varies with age group with elderly patients poorly anticoagulated. The main indication of anticoagulation is MVR which shows a higher percentage of adequately controlled INR (65.5%) Fallowed by anticoagulation due to AF and cardiomyopathy which on the other hand shows a higher percentage of sub-therapeutic control of INR (65.2%) and (62.8%) respectively. The adequacy of anticoagulation is directly proportionate to the educational aspect about the interaction of medication and diet to warfarin therapy with a higher percentage under control in patients who were not educated (61.7%).versus control rate (38.3%). The complication of warfarin use in form of major and minor bleeding was encountered in a higher percentage of patients with uncontrolled high INR (55%) and (56.8%) respectively .with one patient who develop thromboembolic who was under control. Finally, the overall research conclude that the adequacy of anticoagulation was suboptimal with (54.6%) adequately controlled versus (45.3%) uncontrolled. In conclusion, the INR range of anticoagulation at the referral clinic mostly falls in the “under anticoagulated range”. Areas to be considered are patient attendance, staffing and at the same time increasing the efficiency of services. Improvement should be directed not only toward attaining better patient attendance at the clinic but also to educate patients on the importance of adequate control.
There was no specific grant for this research from any funding agencies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
