
Research Article | DOI: https://doi.org/10.31579/2692-9406/023
*Corresponding Author: Mohammed Ahmed A. Ahmed and Kamal Omer Abdalla, Faculty of Medicine & Health Sciences, University of Gadarif, P. O. Box 449, 32211 Gadarif, Sudan.
Citation: M bashir, J O. Alagbe, A M Betty, Omokore E.A. (2020) Etiology and Clinical Features of Acute Flaccid Paralysis among Children in Gadarif, Sudan. Biomedical Research and Clinical Reviews. 1(4); DOI: 10.31579/2692-9406/023
Copyright: ©2020 Mohammed Ahmed A. Ahmed and Kamal Omer Abdalla, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 September 2020 | Accepted: 12 October 2020 | Published: 17 October 2020
Keywords: acute flaccid paralysis; features; etiology; sudan
Acute Flaccid Paralysis (AFP) is a rare but a serious neurological condition characterized by sudden weakness or paralysis of one or more extremities, the respiratory or bulbar muscles and reduced muscle tone without other obvious cause. Death occurs in about 7.5% of AFP affected patients worldwide. AFP is the most common sign of acute polio. Therefore, AFP studies are important for surveillance during polio outbreaks to differentiate polio cases from AFP cases. There is a lack of information about the clinical features & causative factors of AFP among children in Gadarif, Sudan. The identification of AFP cases and its causative factors are important in the management & prevention of the disease. This study assessed the etiology and the clinical features of AFP among children in Gadarif, Sudan aiming at effective management & prevention of the disease. It was a prospective cross sectional study conducted at Gadarif Pediatrics Teaching Hospital during the period of January 2017-December 2019. It comprised 73 children with confirmed AFP, ages 6 months to < 15 years old. Our study revealed that Poliomyelitis was not the cause of AFP. AFP was significantly affected children with youngest ages 0-5 years old and from the rural areas. Guillain-Barré syndrome (GBS) was the leading cause of AFP followed by meningitis, traumatic neuritis and hypokalemia and we believed that infections were the main triggers of GBS. Gender did not affect the prevalence of the AFP. Fever and paraplegia were the most prevalent clinical signs at onset of the weakness. Over 50% of the AFP victims showed symmetric paralysis. It is obviously that AFP-based awareness, provision of high-quality health services and fighting of illiteracy and poverty in the rural areas of Sudan are urgently needed for effective management of AFP.
Acute Flaccid Paralysis (AFP) is a neurological condition characterized by sudden weakness or paralysis of one or more extremities, the respiratory or bulbar muscles and reduced muscle tone without other obvious cause (Alberta Government Health and Wellness, 2005). AFP is often used to describe a sudden onset as might be found with polio. AFP is a rare disease but it is a serious condition. The disease can impair patient’s life and can be life-threatening if it affects the respiratory muscles (Kelly et al., 2006). Recovery from AFP if appropriate therapy is applied may take weeks to years, with about a third having some permanent weakness (Ferri, Fred F., 2016); NIAMS., 2016). Globally, death occurs in about 7.5% of AFP affected patients (NIAMS. 2016). AFP is the most common sign of acute polio. Therefore AFP studies are important for surveillance during polio outbreaks as it helps to eradicate poliomyelitis and to determine the real causes of AFP to prevent its occurrence.
AFP affects the nervous system, specifically the area of the spinal cord gray matter, which causes the muscle reflexes in the body to become weak. AFP is a heterogonous disorder that can be caused by several etiologies. AFP may be caused by disease or by trauma affecting the nerves associated with the involved muscles (Alberta et al., 2005). Clostridium botulinum bacteria that cause botulism can cause flaccid paralysis through producing a toxin that blocks the release of acetylcholine that results in blocking the exocytosis of presynaptic vesicles containing acetylcholine and that prevent the muscle contraction (Saladin, Kenneth S, 2012). If the C. botulinum affects the respiratory muscles, then it can lead to respiratory failure and ultimately death. By a similar mechanism of C. botulinum, a poison found in Curare a pant belongs to the species Chondrodendron tomentosum and various species of the genus Strychnos, native to South America can also cause AFP (Blueplanetbiomes.org; Saladin, Kenneth S, 2012). Other causes of AFP include poliomyelitis (polio), transverse myelitis, Guillain–Barré syndrome, enteroviral encephalopathy, traumatic neuritis and Reye's syndrome (Idris M et al., 2007; Kelly H et al., 2006). Many studies showed that AFP was caused by oral polio vaccinations (www.cdc.gov 2001; Suzanne Humphries and Roman Bystrianyk. 2013; Vashisht et al., 2015). Some venomous snakes and chemical warfarenerve agents such as VX can also cause complete flaccid paralysis (GJ Müller et al., 2012; Sidell, Frederick R. 1997).
The clinical diagnosis of AFP has geographical variations, due to environmental and genetic factors differences (Saraswathy TS., et al., 2008). In Australia 63–72% of AFP cases were attributed to either Guillain-Barré´ syndrome or transverse myelitis (D’Souza et al., 1999). Morris et al., 2003 reported acute disseminated encephalomyelitis, tick-bite paralysis and infant botulism as some causes of AFP in children in Australia. In Malaysia, Guillain-Barré syndrome, central nervous system infections and transverse myelitis were the main causes of AFP (Hussain et al., 1999). While in South West Nigeria, traumatic sciatic nerve palsy, acute polyneuritis, neuropathy and anterior poliomyelitis were the main causes of AFP among children in that country (Fawole, 2003).
From the reviewed literatures mentioned previously, Guillain–Barré syndrome (GBS) was the common main cause of AFP globally wise. GBS is a rapid-onset muscle weakness caused by autoimmune disorders resulted in the immune system damaging the peripheral nervous system (NIAMS, 2016). GBS often affects the arms and upper body. During the acute phase, GBS can be life-threatening, with about 15% of people developing weakness of the breathing muscles (Ferri, Fred F., 2016). Some are affected by changes in the function of the autonomic nervous system, which can lead to dangerous abnormalities in heart rate and blood pressure (NIAMS, 2016). Sometimes the immune dysfunction in GBS is triggered by an infection or, less commonly by surgery and rarely by vaccination. Guillain–Barré syndrome is rare, at one or two cases per 100.000 people every year (Sejvar, James J. et al., 2011). Both sexes and all parts of the world have similar rates of the disease (Ferri, Fred F. 2016). GBS has also been reported in association with COVID-19, and may be a potential neurological complication (Zhao H., et al 2020; Carod-Artal FJ., 2020). There are a number of subtypes based on the areas of weakness, results of nerve conduction studies and the presence of certain antibodies. It is classified as an acute polyneuropathy (Ferri, Fred F., 2016).
In 2002 AFP’s rate in Sudan was found 2.6% (WHO, 2004). AFP is a costly disease as it can cause death with high mortality rate or cause permanent impairment of patient’s life (NIAMS. 2016). There is lack of information available about the clinical features & causative factors of AFP among children in Gadarif in particular and Sudan in general. The identification of AFP cases and its causative factors are important in the management of the disease and its prevention. Ideal treatment and prevention of AFP is based on determination of the etiologic factors. Moreover, regular surveillance and monitoring of common causes of AFP and its regional variations are important to provide physician’s knowledge on the updated and most effective empirical treatment of AFP. The aim of this study was to assess the etiology and the clinical features of Acute Flaccid Paralysis (AFP) among children in Gadarif, Eastern Sudan aiming at better management of AFP and its complications. In this respect this study is important.
This study was a descriptive cross sectional hospital based study that was conducted at Gadarif Pediatrics Teaching Hospital in Eastern Sudan during the period from January 2017 to December 2019. The study comprised 73 children with ages ranging from 6 months to less than 15 years old with confirmed diagnosis of AFP disease. The study aimed to evaluate the etiology and clinical features of AFP in Gadarif aiming at effective management & prevention of the disease. Informed consents were taken from the parents or guardians of the patients. The study was approved by the Health Research and Ethical Committee of the Ministry of Health of Gadarif State.
Inclusion Criteria:
Children from 0 months to less than 15 years old with acute flaccid paralysis in one or more limbs without signs of upper motor neuron lesion were included.
Exclusion Criteria:
Children with signs of upper motor lesion were excluded from the study.
Statistical Analysis
Data was entered into a computer database and SPSS software (SPSS Inc., Chicago, IL, USA, version 21.0) and double checked before analysis. Analysis of variance was used to compare means and x2 was used for categorical variables. Uni-variable and multivariable logistic regression were used to identify factors associated with complications. For associated factors, odds ratios (OR) were determined with 95% confidence intervals [95% CI].
Results:
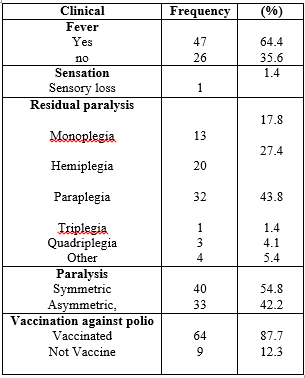
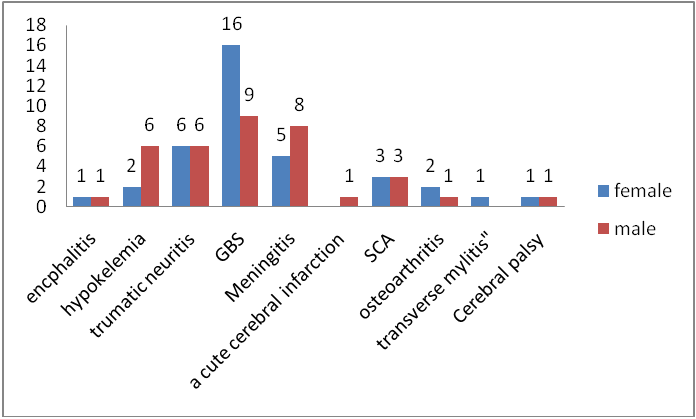
A total of 73 cases of AFP were diagnosed in children less than 15 years old during the 3-year period of the study, of these cases 38 (52.1%) were male and 35 (47.9%) were female (figure1) gave male to female ratio of 1.1:1. The age ranged between 6 months to 15 year with mean 4.1, the majority of patients were seen in 0-5 year’s age group 53 (72.6%) of the AFP cases. The age distribution is shown in (figure2). 65(89%) of cases were of rural residence (figure 3). 40 (54.8%) cases showed symmetrical paralysis of muscles (table1), neck muscles weakness was observed in 2 (2.7%) cases. Paraplegia was high 32 (43.8%) and 47 (64.4%) of cases had fever at onset of weakness. Guillain-Barre Syndrome (GBS) was the main cause of AFP 25(34.2%) of patients, followed by Meningitis (Figure 3).

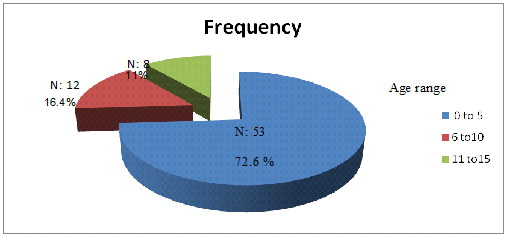
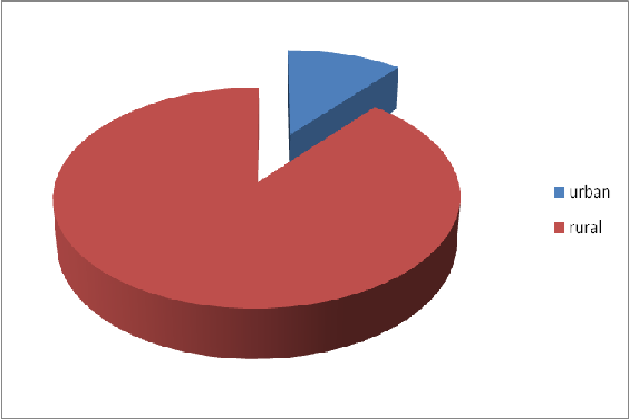
Our study showed that in Gadarif, the frequency of AFP cases was little bit higher among male children 52.1% compared to female children; this difference was not statistically significant (p>0.000). Similar findings to ours were reported in studies conducted in Malaysia, Turkey and Nepal (Saraswathy TS., et al., 2008; Sevencan F., et al., 2013 & Sharma K S., et al., 2011). This fact indicates that gender does not significantly affect the incidence rate of AFP. Our study also revealed that AFP prevalence was higher in children with youngest ages of 0-5 years old as 72.6% of the AFP cases were found within this age range. Similar data to ours were published by Memon et al., 2010 and Sevencan et al., 2013. The fact that AFP is more prevalent among children with smaller ages is believed to be due to their relatively high susceptibility to infections in this age group and the increased susceptibility to the young myelinated peripheral nerves to demyelination (Koulet al, 2010; Rantalaet al, 1994). Generally, children are among human groups who need special care. Children have not well developed immune system, have low nutrient reserves & high metabolic needs; these make children exceptionally more vulnerable to wide arrays of diseases and even slight nutritional deprivation. Children require nutrients and energy to support their growth and development (Kamal Abdalla, 2020). Our study also revealed that rural residents 65(89%) were more susceptible to AFP disease compared to the urban residents 8 (11%), (P < 0.000). This might attributed to high poverty and illiteracy among the rural residents of Sudan compared to urban citizens.
The clinical characteristics showed by this study were fever at onset of the AFP, the lower limbs affected more significantly compared to the upper ones, symmetrically increased in the distal limbs. In this study, more than half of the studied children 87.7% had got completed vaccines against polio. Partial vaccination and non-vaccination of children in Sudan more spread among children of the rural areas due to ignorance of the parents about the importance of vaccination and difficulties to reach city hospitals and health centers where vaccines are normally available. In rural areas of Sudan, still there are big sectors of pregnant women who give delivery by traditional methods far from medicine due to lack or appropriate health facilities.
This study revealed that Guillain-Barre Syndrome was the main cause of AFP among children in Gadarif 34.2%, followed by Meningitis 17.8%. These findings were in agreement with international reviewed literatures published on GBS as mentioned previously in the introduction of this study. GBS is the most common cause of AFP worldwide (Momen and Shakurnia, 2016). This calls for international cooperative efforts to manage the GBS especially to eliminate its causative factors. Sometimes the immune dysfunction in GBS is triggered by an infection or, less commonly by surgery and rarely by vaccination. GBS has also been reported in association with COVID-19, and may be a potential neurological complication (Zhao H., et al 2020; Carod-Artal FJ., 2020). In Sudan, a country with high illiteracy ratios, poverty and poor health knowledge especially among the rural residents of the country, we believe that infections are the major triggering cause of GBS and consequently AFP prevalence among children in Gadarif. Prevention of infections and proper treatment of it during early ages of children between 0-5 years old particularly in rural areas will contribute well in the prevention of AFP. Traumatic neuritis & hypokalaemic paralysis contributed to third & fourth causative factors respectively of AFP among children in Gadarif. These findings were agreement in a report published by Sharma et al., 2011. Also, this calls for joint international efforts to manage traumatic neuritis & hypokalaemic paralysis towards eradication of AFP.
In conclusion, this study revealed that Poliomyelitis was not the cause of AFP. AFP was significantly affected children with youngest ages 0-5 years old and from the rural areas. Guillain-Barré syndrome (GBS) was the leading cause of AFP followed by meningitis, traumatic neuritis and hypokalemia and we believed that infections were the main triggers of GBS. Gender did not affect the prevalence of the AFP. Fever and paraplegia were the most prevalent clinical signs at onset of weakness. Over 50% of the AFP victims showed symmetric paralysis. It is obviously that AFP-based awareness, provision of high-quality health services and fighting of illiteracy and poverty in the rural areas of Sudan are urgently needed for effective management of AFP.
Acknowledgements
The authors sincerely thank the parents and the guardians who consented to participate their children in the study. We also sincerely thank AFP surveillance team for assisting in accomplishing this study.
Conflict of interests
None
Funding
None.
Authors’ Contributions
All authors contributed substantially to the study conception and design, data collection and analysis, and drafting and revision of the article. All authors approved the final version to be published.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
