
Research Article | DOI: https://doi.org/10.31579/2640-1045/058
1House Physician, Islamabad Medical & Dental College.
2Medical specialist, fazia medical college, senior registrar, Krl hospital Islamabad.
3House Surgeon, KRL Hospital Islamabad, Internee, Urology Department Guys & St Thomas Hospital London GBR.
4Senior registrar Fazaia medical college, consultant physician KRL hospital Islamabad.
5Assistant professor of medicine, consultant physician
6House Surgeon, Holy Family Hospital Rawalpindi.
7Resident physician, Internal Medicine Holy family Hospital Rawalpindi, CIBNP Fairfield USA.
8House Surgeon, Holy Family Hospital Rawalpindi, CIBNP Fairfield USA.
*Corresponding Author: Hassan Mumtaz, House Surgeon, KRL Hospital Islamabad, Internee, Urology Department Guys & St Thomas Hospital London GBR.
Citation: Hafeez A., Muhammad F. Ali, Mumtaz H., Fakhra S. Zeb, hafiz Md. Zubair, Meer F., Muhammad A. Shafiq and Fatima T. (2020) Etiology & Outcome of Acute kidney Injury in Intensive Care Unit Settings of a Tertiary Care Hospital J. Endo and Dis; 4(2); DOI:10.31579/2640-1045/058
Copyright: © 2020, Hassan Mumtaz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 November 2020 | Accepted: 28 November 2020 | Published: 30 November 2020
Keywords: etiology; infectious causes; cardiac pathology; GI causes; drugs, mortality; acute kidney injury
Introduction: Acute kidney injury (AKI) is defined as a rapid loss of kidney function occurring over few hours or days. In intensive care unit settings, acute kidney injury (AKI) is a very prevalent condition as most of the patients who are admitted in intensive care units are critically ill. The incidence of acute kidney injury is increasing throughout the world mainly because of aging population and co morbidities which are associated with aging. In intensive care unit settings, the incidence of AKI may reach up to 67%. Though AKI effects depend on clinical situation yet associated with high morbidity and mortality. The rationale of this study is that, as acute kidney is one of major factors contributing in mortality and morbidity of ICU patients, this study will be helpful in identifying important risk factor for development of acute kidney injury in ICU settings, leading to its early detection and thus decreasing associated morbidity and mortality.
Objective: To determine the frequency of etiology and outcome of acute kidney injury in medical intensive care unit of KRL Hospital.
Setting: Medical ICU, KRL Hospital, Islamabad.
Duration: six months from 17th May 2017 to 17th November 2017.
Study design: Descriptive case series.
Material and method: In this study 118 patients were observed. After screening and application of exclusion criteria, a total of 118 patients who were fulfilling the inclusion criteria were selected as the study sample and were included in the final analysis regarding prevalence of risk factors associated with AKI and the outcome associated with AKI. AKI was further classified using acute kidney injury network (AKIN) classification system. Patient age, gender, serum creatinine, etiology and outcome in form of recovery or mortality was recorded.
Results: Overall incidence of AKI in ICU settings in this study was 37.8% (n=118). Out of 118 patients who had AKI, 59.3% (n=70) were male, whereas 40.7% (n=48) were females. Most common risk factor associated with development of AKI was sepsis secondary to infectious illnesses and 39% (n=46) of the patients who developed AKI were suffering from infectious illnesses. Gastrointestinal, drugs and cardiac causes constitutes the 32.2 % (n=38), 18.6% (n=22) and 10.2% (n=12) respectively of the AKI in ICU settings. In terms of outcome, mortality rate in patients with AKI was significantly higher as compared to patients without AKI(P =<0.001) and 56.8%(n=67) of the patients who had AKI died during their ICU stay as compared to 30.4%(n=59) in patients without AKI.
Conclusion: Our study concludes that the frequency of etiology including infectious causes was 39%, cardiac pathology 10%, GI causes 32%, drugs was 19% and mortality was 56.8% in patients with acute kidney injury.
Acute kidney injury (AKI) is defined as a rapid or abrupt loss of kidney function occurring over few hours or days [1]. The hallmark of acute kidney injury is raised serum creatinine levels and a raised blood urea nitrogen (BUN) concentration [2]. The clinical features of acute kidney injury (AKI) are very variable and there may be decrease in urine output or qualitative differences in urine solute concentrations in the absence of oliguria. In 50-60% of the patients diagnosed as having acute kidney injury (AKI), there is no decrease in urine output. Presence or absence of oliguria is related to prognosis of acute kidney injury (AKI). Complications of Acute kidney injury (AKI) include increase potassium level, metabolic acidosis, body fluid imbalance, uremia and patient may require dialysis.
Acute kidney injury (AKI) is an important health disorder affecting people through out the world. It is considered as an important risk factor associated with development of complications and poor prognosis in hospitalized patients. Estimates from literature, regarding prevalence of acute kidney injury showed that 2000-3000 of per million population per year is the incidence of less severe AKI. For severe AKI requiring dialysis, this incidence is 200-300 per million population per year.
Various classification systems have been developed for diagnosis and staging of acute kidney injury (AKI). 2 major classification systems for acute kidney injury (AKI) are Risk, Injury, and Failure; and Loss; and End-stage kidney disease (RIFLE) classification which was developed in 2004 and Acute Kidney Injury Network (AKIN) classification system, which is a modified version of RIFLE classification system and was developed in 2007.
In patients admitted in intensive care units (ICU) of a hospital, AKI is one of common and major complication, associated with poor clinical outcomes. According to literature review, 66 -67 % of patients admitted in intensive care unit settings are likely to suffer from acute kidney injury (AKI) defined by RIFLE classification3.
Acute kidney injury (AKI) is mainly divided into three main categories which are pre-renal, intrinsic and post-renal AKI. The etiology of acute kidney injury is multifactorial. Important risk factors which are associated with development of acute kidney injury include sepsis, drugs, gastrointestinal losses and cardiac causes. Anaphylaxis can also lead to acute kidney injury (AKI).
In studies which were conducted on Hospital acquired acute kidney injury (HAAKI),it was found that , acute tubular necrosis (ATN) and pre-renal cause were the most common form of HAAKI in both medical and surgical ICUs associated with high mortality and morbidity3. Drugs were found as the most common cause of AKI in admitted hospital medical patients, whose incidence was 39.2%4.
In another study sepsis was found as the most common cause of AKI followed by gastroenteritis as the second most common cause of AKI. Surgical, cardiac and hepatic causes were also found as a major contributor towards acute kidney injury. It was also found that mortality rate among patients with AKI was about 37.6%5.
Though AKI effects depend on clinical situation yet associated with high morbidity and mortality6. Some other studies also emphasizes that patients having AKI before or during their ICU stay carry a significantly worse outcome as compared to similar patients without AKI 7.
The rationale of this study is that, as acute kidney is one of major factors contributing in mortality and morbidity of ICU patients, this study will be helpful in identifying important risk factor for development of acute kidney injury in ICU settings, leading to its early detection and thus decreasing associated morbidity and mortality.
Materials and methods
This Descriptive case series was done in Medical ICU, KRL Hospital, Islamabad during six months from 17th May 2017 to 17th November 2017.Sample size was calculated as 116 patients with 95 % confidence of interval and 6% margin of error and 12.4 % expected percentage of AKI stage 1 in patients admitted in ICU with digestive system disorders.
However in this study, screening of all the 312 patients admitted in medical ICU during 6 months of the study period for development of AKI was done and all 118 patients who were fulfilling the inclusion criteria after application of exclusion criteria were included in the final analysis for risk factors prevalence associated with AKI.
Sampling technique done was Non probability consecutive sampling.
Inclusion criteria was Patients of both gender, who develop acute kidney injury during ICU stay for at least ≥ 48hrs with age ranging between 18 and 70 will be included in study.
Exclusion criteria was Patients having previous history of chronic kidney disease, Patients having history of obstructive uropathy, Metastatic diseases affecting patient’s survival, AKI in pregnancy, Surgery related causes of AKI, Patients not willing to participate in the study.
Data collection was done. After approval of hospital ethical committee, all the patients admitted in medical ICU of KRL Hospital, Islamabad during the study period were screened for the presence of AKI and complete history and examination was done by the resident doctor. After screening and application of exclusion criteria, a total of 118 patients who were fulfilling the inclusion criteria were selected as the study sample and were included in the final analysis regarding prevalence of risk factors associated with AKI and the outcome associated with AKI. AKI was further classified using acute kidney injury network (AKIN) classification system. Patient age, gender, serum creatinine, etiology and outcome in form of recovery or mortality was recorded. Confounding factors as laboratory error were double checked with pathology department. Intake/output record will also be double checked with nursing staff. Statistical analysis was done in SPSS version 19. Post stratification chi-square test was applied. P value ≤0.05 was considered significant.
In this study, screening of all the 312 patients, 183 males (58.6%) and 129 females (41.4%) admitted in medical ICU during 6 months of the study period for development of AKI was done and all 118 patients who were fulfilling the inclusion criteria were included in the final analysis for risk factors prevalence associated with AKI. These patients were also assessed regarding outcome associated with AKI in form of mortality or recovery during their ICU stay.
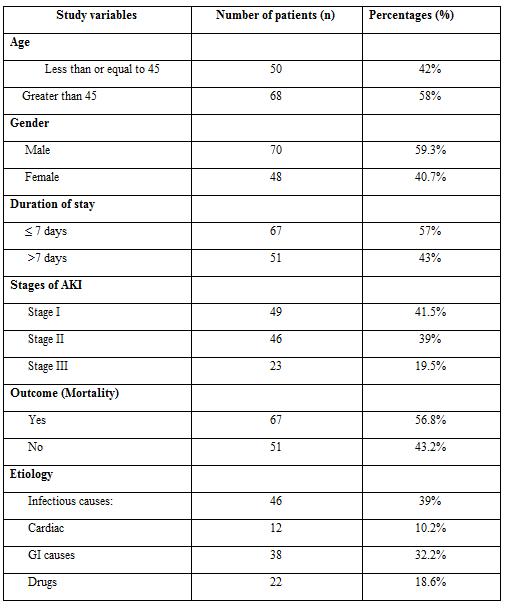
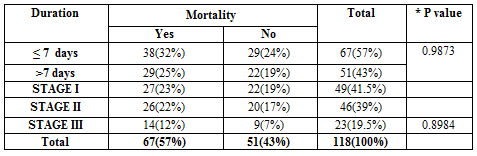
Ages of the patients were between 18 and 70 years and mean age and standard deviation (SD) was calculated as 52.88+13.39 years (Table-1). Gender distribution among 118 patients was analyzed as 70(59.3%) patients were male and 48(40.7%) patients were female. Duration of ICU stay was among 118 patients was analyzed as 67(57%) patients had stayed at ICU for <7 days and 51(43%) patients had stayed for more than 7 days. Status of AKI among 118 patients was analyzed as stage 1, stage 2 and stage 3 AKI were 41.5% (n=49), 39.0% (n=46) and 19.5% (n=23) respectively.
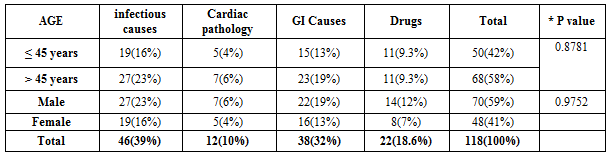
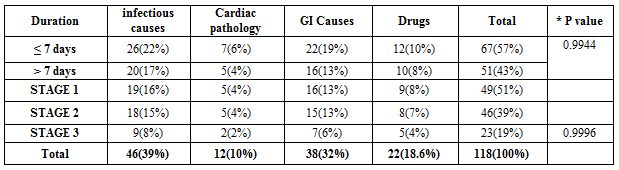
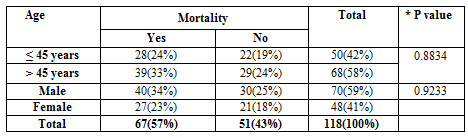
Results regarding etiology of AKI in our study, (Table No 1) showed that, most common risk factor associated with development of AKI was sepsis secondary to infectious illnesses and 39% (n=46)of the patients who developed AKI were suffering from infectious illnesses. Two most common type of infections leading to AKI were respiratory tract infections including community acquired pneumonia, hospital acquired pneumonia and aspiration pneumonia and the urinary tract infections. Other type of infectious illnesses leading to AKI included liver abscess, acute pancreatitis and infection from bed sores. Gastrointestinal diseases were found as the 2nd most common cause of AKI and 32.2% (n=38) of the patients who had AKI developed it secondary to gastrointestinal causes including gastrointestinal losses, gastrointestinal bleeding and liver dysfunction. Among these most common gastrointestinal cause was acute gastroenteritis followed by gastrointestinal bleeding. 18.6% (n=22) and 10.2% (n=12) of the AKI was secondary to drugs and cardiac causes respectively Outcome (mortality) among 118 patients was analyzed as 67(56.8%) patients had mortality while 51(43.2%) didn’t had mortality. Stratification of age with gender, duration of ICU stay and stage of AKI is given in tables 2,3,4,5.
Acute kidney injury (AKI) is defined as a rapid loss of renal function occurring over few hours or days. Complications of acute renal impairment include increase potassium level, metabolic acidosis, body fluid imbalance, uremia and patient may require dialysis. AKI is one of common and major complication, associated with poor prognosis in patients which are admitted in intensive care unit settings. Although incidence of AKI is increasing throughout the world, data regarding its prevalence and prognosis in intensive care unit (ICU) in low resource setups is very little.
This study was planned to find out the incidence of AKI in ICU settings and also to know about the frequency of risk factors which are associated with development of AKI. Study was also aimed at finding out the clinical outcomes which are associated with AKI.
In this study, screening of all the 312 patients admitted in medical ICU during 6 months of study duration was done regarding presence of inclusion criteria and all 118 patients who fulfilled the inclusion criteria after application of exclusion criteria were included in the study. These 118 patients were studied regarding etiology of AKI and the outcome associated with it.
The results of this study that overall incidence of AKI in medical ICU of KRL Hospital Islamabad was 37.8% (n=118). Out of these 118 patients who developed AKI, frequency of stage 1, stage 2 and stage 3 AKI was 41.5% (n=49), 39.0% (n=46) and 19.5% (n=23) respectively.
Although this study showed a high incidence of AKI in ICU settings but it was lower than the incidence of AKI found in an ICU study from Democratic Republic of Congo conducted in 2015, which showed an AKI incidence of 52.7% in ICU settings [1]. A study from Sri Lanka showed an even higher incidence of AKI in ICU settings, which was 60.2% [8]. However a review article suggested an overall all incidence of AKI in ICU settings ranging between 20-50% [6]. The difference in prevalence of AKI is attributed to the different geographical distribution of risk factors leading to AKI and also due to usage of different diagnostic criteria and classification systems regarding evaluation of AKI.
Regarding etiology, the most common risk factor leading to AKI in this study was sepsis secondary to infectious causes and 39% (n=46) of the patients who developed AKI were suffering from infectious illnesses as the primary disease. This finding was consistent with many previous studies including a study from India conducted in 2014, which showed that most common cause of AKI was sepsis, accounting for 38,6% of the patients [5]. Also a recent study from Democratic Republic of Congo suggested infectious illnesses as a leading cause of AKI [1].
In this study ,gastrointestinal diseases accounted for the 2nd most common cause leading to AKI and it included both gastrointestinal bleeding and gastrointestinal losses related illnesses and 32.2%(n=38) of the AKI patients had a gastrointestinal illness as the primary diagnosis. This result was similar to the result of study conducted in India, which also showed the gastroenteritis as the 2nd leading cause of AKI [5]. However some other studies showed a lower incidence of gastrointestinal causes in AKI patients [1].
In our study, drugs was also found as a risk factor significantly associated with development of AKI and 18.6% (n=22) of the AKI developed secondary to the side effects of nephrotoxic drugs. This finding is supported by some previous studies which showed that nephrotoxic drugs lead to AKI in 19–25% of cases in the ICU [9-10].
Only 10.2% (n=12) of the AKI in our ICU was secondary to renal hypo perfusion caused by cardiac contractility dysfunction which was suggested by severe left ventricular systolic dysfunction on echocardiography in these patients. This incidence of AKI secondary to cardiac dysfunction was higher than study results from India, in which cardiac causes constitutes 6.8% of the AKI in ICU settings [2] but it was lower as compared to study conducted in Democratic Republic of Congo (DRC) [1].These differences are attributed to the differences in geographical distribution of diseases and health care facilities.
In terms of outcome , mortality rate in patients with AKI was significantly higher as compared to patients without AKI and 56.8%(n=67) of the patients who had AKI died during their ICU stay as compared to 30.4%(n=59) in patients without AKI. This finding is also supported by the results of various previous studies including the recent study from the DRC in which ICU mortality in patients with AKI was 58% as compared to ICU mortality of 28% in patients without AKI [1]. Similarly results from a study conducted in Sri Lanka showed that ICU mortality in patients with AKI was 52.3% as compared to 23.2% in ICU patients without AKI [5].
In this study, higher stages of AKI were associated with longer ICU stay duration and it showed that AKI is associated with increased hospital stay and health care expenditure .This result is consistent with the previous studies which showed mean increase in ICU stay duration in patients with AKI as compared to those without AKI [5].
Although this study provided valuable information regarding etiology and prognosis of AKI in ICU settings, it has various limitations as well. First of all long term follow up was not done in the patients. Also base line creatinine before admission was not available in some cases and we had to use base line creatinine at admission in those cases. In our study group, many patients had comorbidities like diabetes, hypertension, Chronic obstructive air way disease, ischemic heart disease and cerebrovascular diseases and mortality in patients was also contributed by the primary disease itself and individual relationship between the primary disease and mortality was not investigated in this study. So future studies should also be aimed at finding the relationship of mortality and other comorbidities along with the AKI.
Our study concludes that the frequency of etiology including infectious causes was 39%, cardiac pathology 10%, GI causes 32%, drugs was 19% and mortality was 56.8% in patients with acute kidney injury.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
