
Review | DOI: https://doi.org/10.31579/2640-1053/109
1 Department of Health, Faculty of Vocational Studies, Universitas Airlangga, Surabaya, Indonesia.
2 Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia.
3 Department of Dental Nursing, Poltekkes Kemenkes, Surabaya, Indonesia.
4 Faculty Of Medicine, Universitas Airlangga, Surabaya, Indonesia.
*Corresponding Author: Nanda Rachmad Putra Gofur, Department of Health, Faculty of Vocational Studies, Universitas Airlangga, Surabaya, Indonesia.
Citation: N R P Gofur, A R P Gofur, Soesilaningtyas, R N R P Gofur, M Kahdina, Hernalia M Putri. (2022). Ethiology and Pathophysiology of Whart Hpv Infection: A Review Article. Cancer Research and Cellular Therapeutics. 6(1); Doi:10.31579/2640-1053/109
Copyright: © 2022 Nanda Rachmad Putra Gofur, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 December 2021 | Accepted: 22 December 2021 | Published: 01 January 2022
Keywords: hpv; wharts; pathophysiology; ethiology
Genital Human Papillomavirus (HPV) infection is a self-limiting and often asymptomatic disease. Genital HPV infection is divided into high-risk HPV (HPV 16 and 18) and low-risk HPV (HPV 6 and 11). Low-risk or non-oncogenic HPV produces a clinical picture of anogenital warts, which may be condylomatous, papules, or keratotic. The subclinical form of genital HPV infection can present with an "aceto-white" lesion found on the cervix that will appear when examined using an acetic acid solution evaluated by colposcopy. Based on the association with cervical cancer and precursor lesions, HPV can also be classified as high-risk (HR-HPV) and low-risk (LR-HPV) oncogenic types. LR-HPV types, such as HPV 6 and 11, can cause generalized genital warts or benign hyperproliferative lesions with a very limited predisposition to malignant progression, while infection with HR-HPV types, HPV 16 and 18, is associated with the development of pre-malignant and cervical lesions.
Discussion: Human Papillomavirus is a small DNA virus (50-55nm) belonging to the family Papillomaviridae and genus Papillomavirus. Human papillomavirus (HPV) is a relatively small non-enveloped virus containing a double-stranded circular DNA genome associated with histone-like proteins and protected by a capsid formed by two final proteins, L1 and L2. Each capsid consists of 72 capsomeres, The pathogenesis of HPV begins with infection of stem cells in the basal layer of the epithelium. Once inside the cell, the virus requires expression of the E1 and E2 genes to maintain a low genome copy number. These proteins bind to the origin of replication and the virus secretes cellular DNA polymerases and other proteins required for DNA replication. In the suprabasal layer, the expression of genes E1, E2, E5, E6 and E7 contributes to the maintenance of the viral genome and induces cell proliferation, increasing the number of HPV-infected cells in the epithelium, resulting in a higher number of cells that will eventually produce infectious virions.
Conclusion: In benign HPV lesions, cell proliferation increases leading to increased nutrition, resulting in competition for nutrients and oxygen. Both HR-HPV and LR-HPV E7 proteins increase the level of the transcription factor Hypoxia-inducible factor-1 (HIF-1), and induce increased expression of HIF-1 target genes under hypoxic conditions. Increased HIF-1 activity results in increased transcription of a subset of genes that support angiogenesis, and the induction of this angiogenesis is critical for the persistence and growth of HPV lesions such as genital warts.
Genital Human Papillomavirus (HPV) infection is a self-limiting and often asymptomatic disease. Genital HPV infection is divided into high-risk HPV (HPV 16 and 18) and low-risk HPV (HPV 6 and 11). Low-risk or non-oncogenic HPV produces a clinical picture of anogenital warts, which may be condylomatous, papules, or keratotic. The subclinical form of genital HPV infection can present with an "aceto-white" lesion found on the cervix that will appear when examined using an acetic acid solution evaluated by colposcopy, and can give another form, namely squamous intraepithelial lesions (SIL) using microscopic examination with cytology and histopathology1.
Based on the association with cervical cancer and precursor lesions, HPV can also be classified as high-risk (HR-HPV) and low-risk (LR-HPV) oncogenic types. LR-HPV types, such as HPV 6 and 11, can cause generalized genital warts or benign hyperproliferative lesions with a very limited predisposition to malignant progression, while infection with HR-HPV types, HPV 16 and 18, is associated with the development of pre-malignant and cervical lesions. malignant. HR-HPV types are also associated with many carcinomas of the penis, vulva, anal, and head and neck, and contribute to more than 40% of oral cancers [1,2].
A population-based study in Rochester, MN, reported an incidence of HPV infection of 1.06 per 1000 population in the late 1970s. In Sweden, the incidence of genital HPV infection was estimated to be 2.4 per 1000 population in 1990. In all studies, reported incidence of genital HPV infection was higher more in young women than in men. A study of female college students showed that genital warts would develop clinically after one year of infection with HPV 6 or 11, and develop within 3 years. The second peak was lower in older women, but oncogenic HPV types were found to be more common than non-oncogenic HPV types [3].
Human Papillomavirus is a small DNA virus (50-55nm) belonging to the family Papillomaviridae and genus Papillomavirus. This virus does not have a capsule, each genome consists of about 8000 base pairs of double-stranded nucleotides, circularly shaped DNA [4].
Human papillomavirus (HPV) is a relatively small non-enveloped virus containing a double-stranded circular DNA genome associated with histone-like proteins and protected by a capsid formed by two final proteins, L1 and L2. Each capsid consists of 72 capsomeres, each of which consists of five monomeric units of 55kDa which combine to form a pentamer corresponding to the main protein capsid, L1. The L1 pentamers are distributed to form a network of intra and interterpentameric disulfide interactions that serve to stabilize the capsid. In addition to L1, a minor capsid protein with 75kD in the virion and is called an L2 protein. To form the viral capsid, the pentamers fuse with the L2 copy that closes the center of each pentavalent capsomere [1,5].

The HPV viral genome consists of a single double-stranded molecule and DNA, contains about 8000 base pairs and stores an average of 8 open frames (ORFs). From a functional point of view, the HPV genome is divided into three parts. The first part is upstream noncoding regulation (URR) or length control region (LCR) which has transcriptional regulatory functions of E6 and E7 viral genes. The second is the initial section (E), which consists of six ORFs: E1, E2, E4, E5, E6, and E7, which code for the absence of structural proteins involved in replication and viral oncogenesis. The third is the final part (L) which encodes the structural proteins L1 and L2. The LCR portion of anogenital HPV ranges from 800–900 bp, represents approximately 10% of the genome, and varies substantially in nucleotide composition between individuals [6].
Only one strand of double-stranded DNA serves as a template for viral gene expression and coding for a number of polycistronic mRNA transcripts. The regulation of viral gene expression is complex and is controlled by the cellular and viral components of transcription factors [7].
Most parts of the LCR, contain a cis-active element transcriptional regulator. Virus early promoter, differentiation promoter, and two coordinated polyadenylation signals are regulated during differentiation in body cells. Genes E6 and E7 maintain competency replication. E1 E2, E4, E5, and E8 are involved in viral DNA replication, control transcription, among other functions. L1 and L2, are responsible for the assembly of viral particles. When the cells have entered the body, the tissue will undergo host stratification/differentiation. Once activated, the promoter further promotes transcription from a heterogeneous set of start sites and serves to generate transcripts that facilitate the translation of L1 and L2 proteins. Furthermore, gene expression will occur, encoding structural proteins L1 and L2, which combine to form a capsid and form a virion [8].
Pathogenesis
HPV is epitheliotropic and replication occurs in the differentiated squamous epithelium. Viral DNA can be detected in the lowest layer of the epithelium. While the protein coat can be found in the superficial layer. HPV infection can give a picture of stratum spinosum cell hyperplasia (acanthosis) with the stratum corneum having one or two layers of parakeratotic cells. The dermal papillae are elongated and there are well-defined boundaries in the dermis. The presence of koilocytes cells, which are squamous cells that have large and mature sizes, have a clear perinuclear zone, which has expanded beyond the cell layer. The nucleus of the koilocyte cell is enlarged and hyperchromatic and sometimes doubles in appearance. These cells show a cytopathic effect caused by HPV. These cells are not sensitive to predict the presence of HPV infection in the cervix [9].
The pathogenesis of HPV begins with infection of stem cells in the basal layer of the epithelium. Once inside the cell, the virus requires expression of the E1 and E2 genes to maintain a low genome copy number. These proteins bind to the origin of replication and the virus secretes cellular DNA polymerases and other proteins required for DNA replication. In the suprabasal layer, the expression of genes E1, E2, E5, E6 and E7 contributes to the maintenance of the viral genome and induces cell proliferation, increasing the number of HPV-infected cells in the epithelium, resulting in a higher number of cells that will eventually produce infectious virions. In more differentiated cells of the same epithelial layer, promoter activation is dependent on differentiation and maintenance of E1, E2, E6 and E7 gene expression. Furthermore, there will be an activation of the expression of the E4 gene, which will promote the amplification of viral genome replication, greatly increasing the number of virus copies per cell, at the same time the expression of L1 and L2 genes occurs [10].
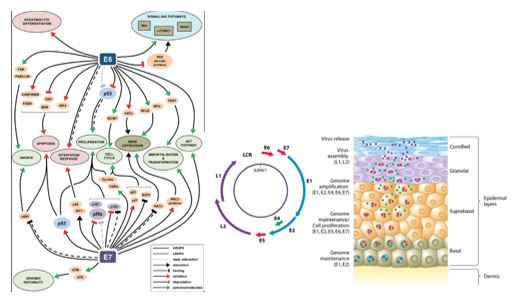
In the granular layer, the gene end products, major and minor proteins of the viral capsid, L1 and L2 respectively, from the viral capsid and virion formation, which reach the cornified layer of the epithelium and are released. HPV replication begins when host cell factors interact with the LCR region of the HPV genome and begin transcription of early viral genes, at E6 and E7. Viral gene products E6 and E7 deregulate the cell cycle, impairing cell growth regulatory pathways and modifying the cellular environment to facilitate the virus. Replication in cells occurs terminally. Infection with HR-HPV usually lasts from 12 -18 months and can be cured depending on the immune system. However, about 10% of women fail to develop a cure for HPV infection, resulting in persistent infection [11].
Many studies classify HPV infection as persistent if HPV is detected in two consecutive follow-up visits, 4–6 months apart. The persistent nature of HPV infection and the integration of viral DNA into the cell genome contribute to an increased risk of high-grade and malignant lesions due to the resulting genomic instability. E6 and E7 can induce centrosomal abnormalities resulting in abnormal centrosome reduplication, leading to an abnormal number of centrosomes [9].
In benign HPV lesions, cell proliferation increases leading to increased nutrition, resulting in competition for nutrients and oxygen. Both HR-HPV and LR-HPV E7 proteins increase the level of the transcription factor Hypoxia-inducible factor-1 (HIF-1), and induce increased expression of HIF-1 target genes under hypoxic conditions. Increased HIF-1 activity results in increased transcription of a subset of genes that support angiogenesis, and the induction of this angiogenesis is critical for the persistence and growth of HPV lesions such as genital warts.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
