
case report | DOI: https://doi.org/10.31579/2641-0427/022
*Corresponding Author: Khadiga Ahmed Ismail, Faculty of Applied Medical Sciences, Taif University Taif Saudi Arabia. Parasitology Department Faculty of Medicine, Ain-Shams University Cairo Egypt.
Citation: Marzouq K. Mahmoud., Ismail A. Khadiga., Khalifa M Ahmed., Khalifa M. Osama., (2020) Erythema Dyschromicum Perstans.J. Orthopaedics and Surgical Sports Medicine, 3(1): Doi:10.31579/2641-0427/022
Copyright: © 2020 Khadiga Ahmed Ismail. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 January 2020 | Accepted: 15 January 2020 | Published: 29 January 2020
Keywords: erythema dyschromicum perstans; melanocytes; basal cell keratinocytes; antigens; vacuolar liquefactive
Erythema dyschromicum perstans is an asymptomatic eruption of oval, polycyclic, or irregularly shaped, gray-blue hyperpigmented macules on the trunk, the arms, the face, and the neck. It begins as ash-colored macules, sometimes with an erythematous or elevated border. The patient is not usually suffer from any systemic symptoms. Erythema dyschromicum perstans may resolve in 2-3 years in prepubertal children, but it is more likely to persist in adults. [1]
Erythema dyschromicum perstans (EDP) most often affects darker skinned patients, most frequently Latin Americans and Indians. It has also been reported in people of lighter skin colour and various ethnicities. It may occur in women more often than men. It is repoted in young adults than adults.
The exact etiology of EDP is unknown. Damage to melanocytes and basal cell keratinocytes that is observed with EDP is due to an abnormal immune response to antigens with a predominance of CD8 + T lymphocytes in the dermis and HLA-DR +, intercellular adhesion molecule 1 + keratinocytes in the epidermis.
EDP is characterized in histological examination by a vacuolar liquefactive degeneration of the basal cell layer with dermal melanosis and a perivascular infiltrate.
65 years old Saudi male patient, presented with slow onset of asymptomatic pigmentation in the trunk and less prominent pigmentation in the extremities since few months as shown in plates [1, 2 , 3 , 4] . He was under treatment with phenytoin 100 P/O T.I.D. There was no oral pigmentation. There was also no other associated symptoms.




Laboratory Investigations:
As regard his complete blood count:
The clinically significant results are as follows:
White blood cell count (WBC) of 7.70 k/µL (N) (n 4 – 10 k/µL), with a eosinophilia of 15.3% (n 1-6%) , Red blood cell count (RBC) of 4.61 M/µL (L) (n 4.5-5.5 M/µL) with a hemoglobin of 12.30 gm/dl (L), hematocrit of 39.70% (L) (n 40-50%), Platelet count of 237 K/µL (N) (n 150-410 K/µL).
As regard his chemistry:
His random glucose of 98.20 mg/dL (n 70-140 mg/dL), blood urea of 13.40 mq/dL (low) (n 20-48 mq/dL), creatinine of 0.61 mq/dL (n 0.6-1.2 mq/dL), normal SGOT (AST) (26µ/L) (n 0-42 µ/L), normal SGPT (ALT) (17 µ/L) (n 0-33 µ/L), normal bilirubin (total) (0.243 mg/dL) (n 0-1.1 mg/dL), total protein (7.93g/dL) (n 6.6-8.7 g/dL), chloride (101 mmol/L) (n 98-107 mmol/L), sodium (135 mmol/L) (n 135-151 mmol/L), potassium (4.6 mmol/L) (n 3.4-5.1 mmol/L), normal prolactin (275 µU/mL) (n 86-324 µU/mL), testosterone (total) (3.75 ng/mL) (n 2.8-8 ng/mL), low cortisol AM. (97 nmol/L) (n 171-536 nmol/L), insulin (23.4 µU/mL) (n 2.6-24.9 µU/mL),and low vitamine D total (25 ng/mL) (n 30-70 ng/mL).
Histological Findings
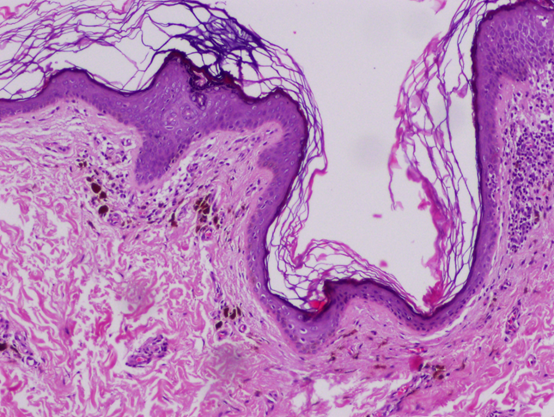
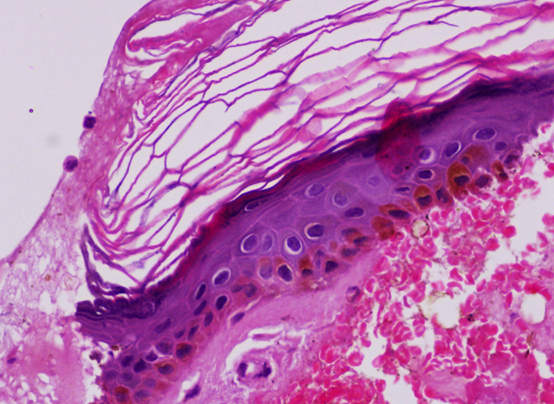
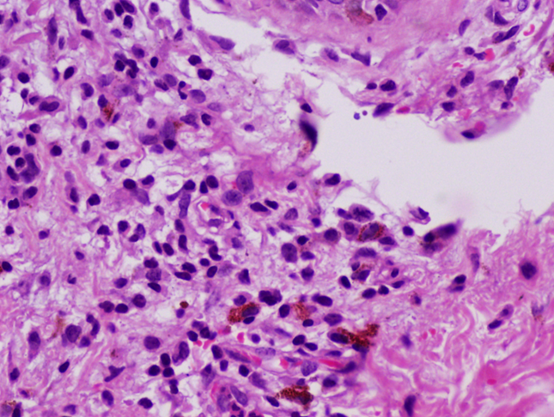
Sections examined from skin biopsy showed basket-weave cornified layer, slight epidermal hyperpigmentation, focal vacuolar alteration, subepidermal melanophages, mild perivasular lymphocytes infiltration in the dermis as shown in plate [5, 6, 7].
Differential diagnosis:
1- Erythema dyschromicum perstans
2- Dermatologic Aspects of Addison Disease
3- Allergic Contact Dermatitis
4- Dermatologic Manifestations of Hemochromatosis
5- Lichen Planus
Erythema dyschromicum perstans
Erythema dyschromicum perstans (EDP) is a pigmentary disorder characterized by multiple pigmented macules on the trunk and proximal extremities. The hallmark of this disease is erythema occurring on the border of the pigmented macules. On the other hand, ashy dermatosis (AD) or dermatosis cenicienta is a pigmented condition characterized by persistent ashy hypermelanosis. Although these diseases are often considered to be identical, some clinical features differ. For example, erythema with scaling around the pigmented patch is a characteristic feature of EDP. [11] The etiology of erythema dyschromicum perstans is unknown, but many consider erythema dyschromicum perstans to be a variant of lichen planus actinicus. A variety of predisposing factors have been cited. These include ingestion of ammonium nitrite, an intestinal parasitosis caused by nematodes (whipworm infection, control of which produced erythema dyschromicum perstans remission), orally administered radiographic contrast media, and, possibly, an occupationally associated cobalt allergy in a plumber. [12]Histological Findings are usually show mild basal cell layer vacuolar degeneration overlying an upper dermis with a mild perivascular mononuclear cell infiltrate and increased melanophages. [13]
Dermatologic Aspects of Addison Disease
One of the major finding of Addison disease hyperpigmentation of the skin [2] and mucous membranes, also decreased pubic and axillary hair in women, vitiligo, dehydration, and hypotension. Oral mucous membrane hyperpigmentation is pathognomonic for the disease. [3, 4]
Hyperpigmentation of the skin is considered a prominent feature of Addison disease and is present in 95% of patients with chronic primary adrenal insufficiency. However, hyperpigmentation is not a universal sign of adrenal insufficiency. Although the presence of normal-appearing skin does not exclude the diagnosis.The skin may appear normal, or vitiligo may be present. Increased pigmentation is prominent in areas of the skin that are subject to increased pressure, such as over the knuckles or the skin creases. Hyperpigmentation is also prominent on the nipples, axillae, perineum, and buccal mucosa. [3, 4]
In our case, there is no abnormailty in the electrolyts as in Addison disease as shown in labortatory results.
Pigmented contact dermatitis
May appear as characteristic erythema, papules, and pruritus associated with epidermal melanosis, with little preexistent actual dermatitis, followed by hyperpigmentation from chemicals in washing materials. [23]
Dermatologic Manifestations of Hemochromatosis
Around 90% of patients with idiopathic hemochromatosis had cutaneous hyperpigmentation, although it may be mild. [4] Hyperpigmentation is one of the earliest signs of the disease, and it tends to be most pronounced on sun-exposed skin, particularly on the face, with a coloration of brownish bronze or, at times,
slategrey
Structures of skin are injured by iron deposits and increased synthesis of melanin in melanocytes. The rapid tanning with minimal sun exposure reflects the synergistic effects of iron accumulation and sun exposure, but is the result of melanin, rather than the iron itself. Hyperpigmentation often accentuates during exacerbations and regresses with therapy. Treatment with phlebotomy does not immediatelyresolvethehyperpigmentation.[13]
Ichthyosiform alterations, skin atrophy, koilonychia, and hair loss may also be evident. In the series of 100 patients, ichthyosis-like changes were evident in 46% of patients. [4] Ichthyosiform changes may be mild or marked. Skin affected with ichthyosiform changes is very dry. [13] Cutaneous atrophy was observed in 42% of 100 patients, usually on the anterior surface of the leg.
Hyperpigmentation of the oral mucosa was found in 15-20% of patients. Dental pigmentation with enamel loss may be noted. [14] Sanchez-Pablo and coworkers found hyposialia in hemochromatosis-affected patients. [15]
The cutaneous hyperpigmentation in patients with hereditary hemochromatosis should be differentiated from drug-induced hyperpigmentation and actinic reticuloid.
Lichen Planus
Distinguishing ashy dermatosis from lichen planus pigmentosus (LPP) is not always easy. A Mexican study of 20 patients with erythema dyschromicum perstans and 11 with LPP provided clear clinical delineation between the 2 often histologically indistinguishable disorders. [31] LPP has pruritic brownish black macules or patches, with no active border, on the face and the flexor folds. Erythema dyschromicum perstans does not involve mucosal surfaces, where LPP does. In favor of erythema dyschromicum perstans being either a subset of idiopathic lichen planus or a lichenoid drug eruption are reports of lichen planus and erythema dyschromicum perstans occurring in the same patient, the clinical resemblance of erythema dyschromicum perstans to atrophic lichen planus, and similar histologic patterns with immunofluorescence in both erythema dyschromicum perstans and LPP.
The border of an active erythema dyschromicum perstans lesion and the border of an LPP lesion often both show hyperkeratosis, a thinned epidermis, hydropic degeneration of the basal layer, pigment incontinence, and a perivascular lymphohistiocytic infiltrate. Colloid bodies are occasionally seen in both.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
