
Research Article | DOI: https://doi.org/10.31579/2834-5142/017
1 Departament of Urology. Hospital “Evita Pueblo”, Berazategui, Buenos Aires, Argentina.
2 Chair of Cytology, Histology and Embryology, Faculty of Medical Sciences, UNLP, Buenos Aires, Argentina.
*Corresponding Author: Pablo Francisco Colaci, Departament of Urology. Hospital “Evita Pueblo”, Berazategui, Buenos Aires, Argentina.
Citation: Pablo Colaci, Flavio Santinelli, Gustavo López, Fernando Mías, Marcela García, Claudio Baldarena (2022). Epidemiology and Prognostic Factors for Survival of Clear Cell Renal Carcinomas. International Journnal of Clinical Nephrology. 4(1); DOI:10.31579/2834-5142/017
Copyright: © 2022 Pablo Francisco Colaci. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 December 2021 | Accepted: 12 January 2022 | Published: 18 January 2022
Keywords: renal cell carcinoma; clear cell; survival; prognostic factors
Tumor size, histologic grade, and TNM classification characterize kidney tumors and provide a useful prognosis for predicting survival in research and medicine. Our objective was to determine the postoperative survival of operated patients with a diagnosis of clear cell renal carcinomas (CCRC) and to evaluate its relationship with other prognostic factors. Age, sex, clinical presentation, size, Fuhrman nuclear grade, tumor-nodule-metastasis (TNM) stage, and the presence of local invasion were retrospectively analyzed in 66 patients operated on for clear cell renal carcinomas. Clinical follow-up was performed for 5 years to determine postoperative survival.
During the follow-up period, 17 deaths occurred, with the cancer-specific survival rate being 77%. The presenting symptoms of the tumor that led to the diagnosis were not related to postoperative survival. The estimated survival for stages T2 was 100%, for T1 it was 93%, and for T3 it was 55%. No patients were found in stage T4. The lower Fuhrman grades (I and II) had an 85% survival rate, while the higher grades (III and IV) had a 53% survival rate. Survival rates also varied depending on the type of adjacent tissue that was affected. Specifically, survival decreased to 80% when infiltrating the renal capsule, 70% when infiltrating the perirenal tissues, and 28% when invading the renal vein. We can conclude that tumor size in CRCC is not a prognostic factor that allows determining postoperative survival independently, and for this reason, it should be considered as a variable that acquires importance when evaluated together with the presence of vascular invasion or adjacent tissues. We can confirm that the Fuhrman Histological Grade is useful as an independent parameter of survival when grouped into low and high grades.
Renal cell carcinoma represents the third most common genitourinary tumor, with prostate and bladder cancer being more prevalent. The clear cell renal carcinoma (CRCC) subclass represents between 84.5 and 90% of renal cell carcinomas, according to works published in North America and Mexico. In Argentina, however, the Institute of Oncology Ángel H. Roffo reported that clear cell tumors are responsible for 70 to 80% of total renal carcinomas [1-3]. Its incidence is higher in men than in women (1.5 / 1) and it affects black men more frequently. It presents an increased incidence in ages 54 through 70, with an average age of onset of 63 years, while these ages vary depending on the region studied [4]. In Latin America, the country with the highest incidence is Brazil [5]. In Argentina, renal cell carcinoma is the 9th leading cause of cancer death
in men and the 13th in women, with an incidence, according to the World Health Organization, of 6.1 cases per 100,000 inhabitants and a mortality rate per year of 3.4 cases per 100,000 inhabitants [1]. Various studies have shown that between 40 and 60% of CCRC are detected incidentally through imaging studies performed for other pathologies [3,6,7]. Only 6 to 10% of cancers present with one or more symptoms of the classic triad: hematuria, palpable flank mass, and low back pain or paraneoplastic syndromes [8]. Several prognostic factors for postoperative survival have shown their value in daily practice, such as tumor size, Fuhrman histological grade, and tumor-nodule-metastasis (TNM) staging. These prognostic factors are important pillars for both researchers and clinicians [9-11]. Our objectives are to evaluate the distribution of CCRC according to age, sex, and clinical presentation, and to determine overall postoperative and cancer-specific survival within our population.
With the approval of the teaching and research committee of the Hospital "Evita Pueblo", 66 patients with a diagnosis of CCRC during the period between January 2005 and December 2009 who had been operated in the aforementioned hospital were studied. Patients operated by all nephrectomy techniques (radical or partial, with open or laparoscopic technique) were included in the study. Fourteen cases were excluded for not having the necessary data for follow-up and 2 cases for presenting mixed tumors. The clinical characteristics studied were gender, age, and clinical presentation through the analysis of medical records, while the histopathological characteristics studied were tumor size, Fuhrman histological grade, and TNM staging. Preoperative files prepared before the patient's admission to the operating room, CT results, and ultrasound results were used to determine the age, gender of the patient, form of presentation, tumor size, and presence of metastases. The Fuhrman histological grades were re-evaluated by micrometric measurements, in the Chair of Histology "A" of the UNLP. The patients were followed up to assess survival, every six months for the first two years and then annually for up to 5 years. The SPSS Statistics 17.0 software was used to obtain descriptive data and the Kaplan Meier test to evaluate postoperative survival.
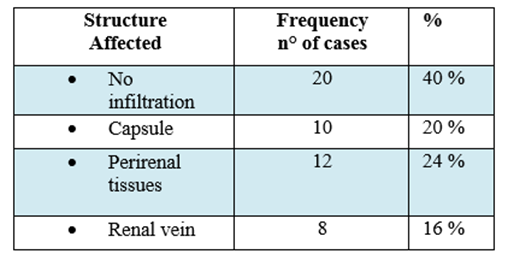
Of the total sample (n = 50), 12 were female and 38 were male, corresponding to 24% and 76% of the sample size, respectively. The mean age of detection of clear cell carcinoma was 60 years (range, 37-79 years). The mean tumor diameter was 6.38 cm (range, 2-15 cm). The right kidney was predominantly affected over the left, 58% and 42% respectively, and more frequently in the upper and mesorenal pole. In 58% of the cases, the tumors were diagnosed as an asymptomatic finding by ultrasound, computed tomography, or magnetic resonance imaging performed for other pathologies, while in 42% it was diagnosed by other signs and symptoms such as hematuria, flank pain, and urinary tract infection. The Fuhrman grades were distributed according to the following percentages: Fuhrman 1: 6%, Fuhrman 2: 68%, Fuhrman 3: 24% and Fuhrman 4: 2%. Regarding the infiltration of peripheral tissues, 40% of the tumors were not infiltrating, 20% infiltrated the renal capsule, 24% invaded perirenal tissues, and 16 affected the renal vein. No case infiltrated Gerota's fascia (Table I).
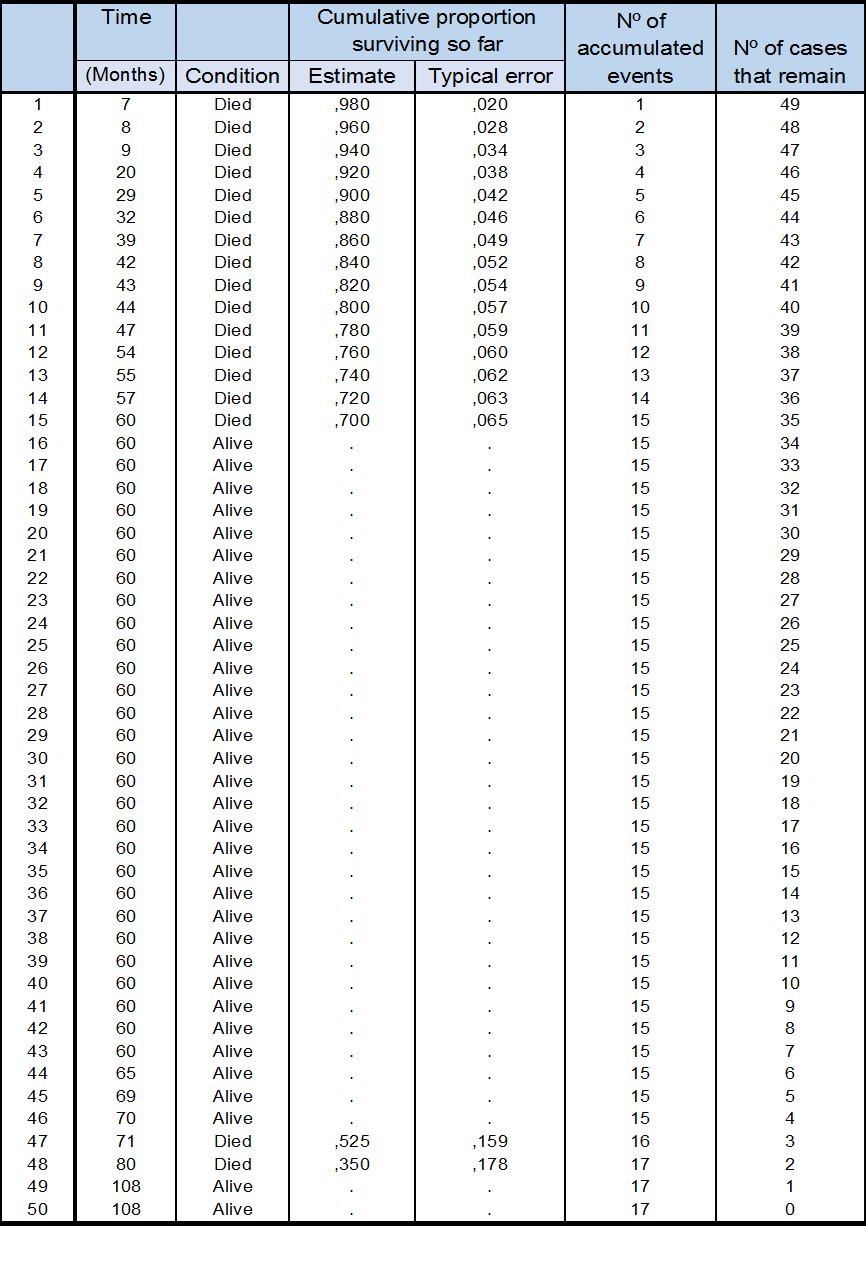
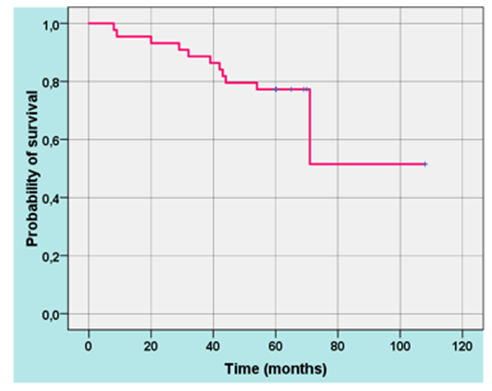
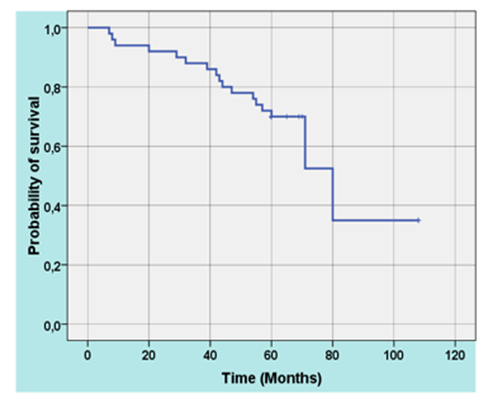
Stage T1 tumors were the most frequent (54%), followed in frequency by T3 (42%), and only 2 cases in stage T2 (4%). In our sample, we did not find tumors in T4 stage. There were 17 deaths during the 5-year follow-up, 12 of these due to metastases in the lung, bone, brain, or contralateral kidney; 1 due to postoperative hemorrhagic complication, and 4 due to other causes not related to the tumor. The overall survival rate was 70%, while the specific cancer survival rate was 77% (Table II. Figure 1 y 2).
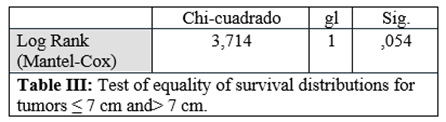
Tumors smaller than or equal to 7 cm had a 3-year survival rate of 96%, and those greater than 7 cm, 67% (p <0>
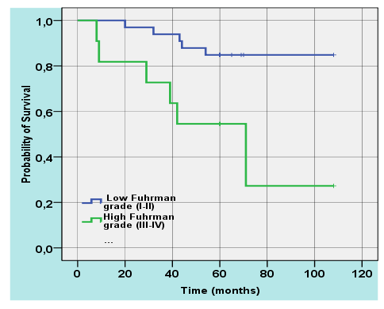
The lower Fuhrman grades had a survival rate of 85%, while the higher grades had a survival rate of 53% (P.0.014) (Figure 3. Table V). Regarding survival depending on the type of peripheral tissues invaded by the tumor, when there was no infiltration, it was 100%, and successively lower when infiltrating the renal capsule (80%), perirenal tissues (70%) and renal vein (28%) (p 0.000) (Table VI).
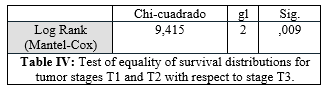
The mean age of presentation (60 years) and the increased incidence of CRCC in males coincide with the main works published in several countries [4,6,7], although our incidence in men is even higher, possibly in relation to environmental factors, such as industrial pollution in the Buenos Aires suburbs and occupational exposure. The incidental finding is the most frequent form of diagnosis in the last decade, with predominant involvement of the right kidney [2,6,12-14]. The mean tumor size was similar to that found by other authors, while the predominant histological grade was Fuhrman grade II [6,12,14]. Regarding tumor stages, like another study in Madrid, we found a low percentage of T2, due to the fact that a large part of tumors larger than 7 cm present invasion of the perirenal tissues or involvement of the renal vein [15]. For this reason, there are insufficient cases in stage T2 to validate the statistics when calculating survival. Grouping stages T1 and T2 show significant differences in cancer-specific survival with respect to stage T3. Our cancer-specific survival rates are among those published in other countries such as Spain and China [16,17]. Unlike other authors, we have found statistically significant differences in postoperative survival in relation to tumor size [8,18,19]. In other words, in our study, patients with tumors smaller than or equal to 7 cm did not have a greater postoperative survival than those larger than that size; instead, invasion of the perirenal tissues and the presence of tumor venous infiltration were factors directly related to the risk of mortality from kidney cancer as in several published studies [20-27].
Based on the data obtained in our research, we can determine that tumor size in CRCC is not a prognostic factor that allows determining postoperative survival independently, and for this reason, it should be considered as a variable that acquires importance as it is evaluated together with the presence of vascular invasion or of the adjacent tissues. Likewise, we can confirm that the Fuhrman Histological Grade is useful as an independent parameter of survival when grouped into low (I and II) and high grades (III, IV). We believe that the high incidence in the male sample in our population could be attributed to work activity, since the hospital is located in a manufacturing area with high levels of environmental pollution, but more studies should be carried out that can corroborate our hypothesis.
The authors are especially grateful to María Laura Colaci, Camila Sarcone y Dora Pilz for their grammatical and technical assistance.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
