
Review Article | DOI: https://doi.org/10.31579/2693-7247/041
1 Assistant, Department of infectious Diseases and Tropical Medicine, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
2 Assistant Professor, Infectious Department, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
3 Assistant Professor, Clinical Research Development Unit, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
4 Assistant Professor, Department of infectious Diseases and Tropical Medicine, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
5 Infection Control Supervisor, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran
*Corresponding Author: Amin Bojdy, Assistant Professor, Infectious Department, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
Citation: Yeganeh Ahrari, Amin Bojdy, Mona Najafi, Mahnaz Arian, Nasrin khosravi Zeenyani (2022) Epidemiology and Outcome of Candidemia in ICU, Mashhad, a 6-Year Multi-Center Study. J. Pharmaceutics and Pharmacology Research, 5(2); DOI:10.31579/2693-7247/041
Copyright: © 2022 Amin Bojdy, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 November 2021 | Accepted: 10 December 2021 | Published: 05 January 2022
Keywords: drug discovery; therapeutic drug; COVID-19
Background and aim: candidemia is a state that usually happens in immunocompromised patients. Thus it is more prevalent in ICU patients. This status brings mortality and morbidity; however, the outcome is various in different ICU care settings. The aim of this study is to assess epidemiology of outcome of candidemia in ICU in Mashhad during a 6-year period.
Method: in a cross-sectional study between 2012 and 2018 in different ICU centers affiliating with Mashhad University of Medical Sciences, data of candidemia patients were extracted from hospital information system. These data were demographic, past medical history, result of the culture, and antifungal treatment.
Result: totally, 55 patients (22 men and 33 women) were included in the study. The mean age of the patients was 45.9±1.9 years. Furthermore, the mean duration of hospitalization and the mean duration of ICU care were 43 and 37 days, respectively. Five patients had a history of immunosuppressive treatment and four patients were prescribed antifungal treatment in their past medical history (all with fluconazole and none with Itraconazole). Eighteen patients received caspofungin, eleven Amphotericin B treatment, and two fluconazole with no significant difference in outcome of the patients regarding antifungal type. In case of coincident antibiotic treatment, Carbapenems were prescribed in 43 patients, Glycopeptides in 48 patients, 25 patients had Cephalosporin treatment, and 13 patients had Fluoroquinolone treatment with no significant difference regarding the antibiotic type.
Conclusion: The mortality percent of candidemia in ICU was 69.1 within mean time of 37 days. Furthermore, there was no significant difference in outcome of the patients regarding using Caspofungin or Amphotericin. Timely initiation of antifungal regarding to the culture result may bring better outcomes.
Candida family is a vast group of molds presenting in many surfaces especially as a saprophyte yeast [1]. This fungus is present in many parts of the human body, especially mucosal surfaces and as a commensal microbiota can adapt environmental changes [2]. These predisposing factors may be immunocompromising conditions such as human immunodeficiency virus (HIV) infection, using immunosuppressive treatments, and chemotherapy, or presence of some chronic diseases such as diabetes, hematologic malignancies, end stage renal disease, liver disease, and etc [3, 4].
However, candidiasis mainly is caused by C. albicans, C. parapsilosis, C. glabrata, C. tropicalis, and C. krusei [5]. Among several candida species C. albicans is the major pathologic specie that is responsible for 46.3% of cases. In the second step C. glabrata stands with 24.4% of the found species in cultures [6]. The morbidity and mortality of the candidiasis mostly depends on the immunity response of the host, virulence of the candida specie and strain, and anatomical site of infection [7, 8].
The invasive infestation of candida as blood borne disease is called candidemia. This condition brings 20% to 40% mortality rate [9]. The estimated financial cost at an episode of hospitalization due to candidemia is around $25,000–$55,000 in US [10]. In Iran, it is reported that 70.4% of invasive fungal infections are due to the infestation of candida [11]; however, lack of sufficient epidemiologic data is sensed through literature review [12]. The aim of our study is to assess epidemiology and outcome of candidemia in an intensive care unit in Ghaem and Imam Reza Hospital, Mashhad, Iran, between 2012 and 2018.
We conducted a cross-sectional study in Emam Reza and Ghaem Hospitals, which are educational hospitals of Mashhad University of Medical sciences, between 2012 and 2018. Presuming that a vast number of candidemia cases are found in intensive care units (ICUs), this study was conducted on ICU patients. First of all, Candidemic patients, those who had positive blood culture for candida, were extracted from hospital information system (HIS) using the medical records of the ICU patients in this data base. Total steps of the study was in line with the Helsinki ethics declaration and ethics committee of Mashhad University of Medical Sciences approved all the ethical points in our study.
Totally, 55 patients were included in the study consisting of 22 men (40%) and 33 women (60%). The mean age of the patients was 45.9±1.9 years. The mean duration of hospitalization in total was 43 days and the mean duration of ICU admission was 37 days. Fourteen patients had diabetes, 6 suffered from end stage-renal disease, 27 had cardiovascular disease, 4 had a history of surgery, and one patient had underwent organ transplantation. None of the patients had a history of liver disease, hematologic malignancy, and chemotherapy. Five patients had a history of immunosuppressive treatment. Four patients had a history of antifungal treatment and all of them had a history of previous fluconazole therapy, and none of them have taken Itraconazole.
24 patients (43.6%) received no antifungal treatment. 11 patients had no antifungal treatment and 13 were expired before receiving antifungal treatment. In case of antifungal treatment in ICU admission, 18 patients (32.7%) were prescribed caspofungin, 11 (20.0%) had Amphotericin B treatment, and 2 (3.6%) had fluconazole treatment. Data regarding coincident antibiotic treatment showed that Carbapenems were prescribed in 43 patients (78.2%), Glycopeptides in 48 patients (87.3%), 25 patients (45.5%) had Cephalosporin treatment, and 13 patients (23.6%) had Fluoroquinolone treatment. Antifungal treatment was initiated in 15 cases (27.3%) before a period of two weeks, in 8 cases (14.5%) within two weeks, and in seven cases (12.7%) in a timing of more than two weeks. Seventeen cases expired in a period of less than one week and 19 (34.5%) patients expired in a timing of more than one week from the positive blood culture for candida. Other body fluid culture was negative in 63.6% of the patients. Nineteen patients (34.5%) had a urinary culture of candida and only one case (1.8%) had a peritoneal fluid positive for candida. Five patients (9.1%) also had received prednisolone (Table 1). All of the patients had urinary catheter with a mean duration of 33.7 days. Also, 46 patients had CV line with a median duration of 22 days.
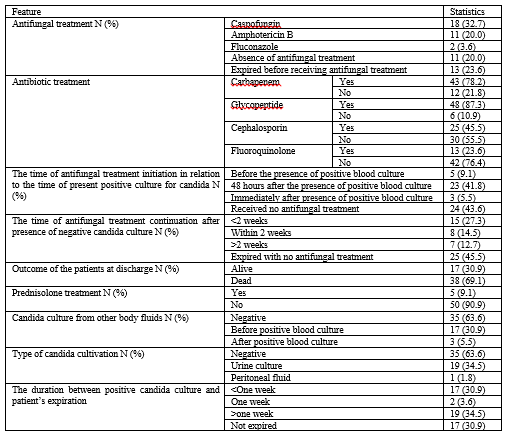
Most of the patients (23 cases or 41.8%) received treatment during the first 48 hours after the presence of positive blood culture. The outcome of the patients showed that 17 patients (30.9%) were alive at the end of study and 38 patients (69.1%) were dead (table 2). There were no significant difference in outcome of the patients regarding using Carbapenem (p=0.227), Glycopeptide (0.999), Cephalosporin (p=0.562), or Fluoroquinolone (p=0.500). 29.4% of the patients who received Caspofungin, were alive, 63.6% of those who received Amphotericin, and 33.3% of the patients who received Fluconazole were alive. There was no significant difference regarding the outcome of Caspofungin and Amphotericin (p=0.074). Table 2 shows the details of the above mentioned. 51 patients (92.7%) received wide spectrum antibiotic therapy.
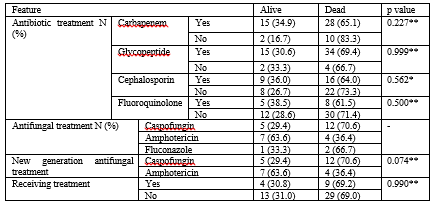
*Fisher’s exact test; **chi-square test
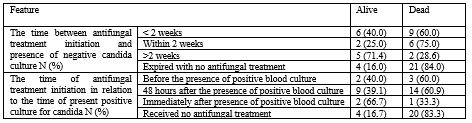
Table 3 also shows the distribution of the patients’ outcome regarding the timing of the initiation of anti-fungal therapy. 40 percent of the patients who had a negative blood culture for candida in less than two weeks were alive, however, this was 71.4 percent in patients with a period more than two weeks. It has also been shown that 66.7% of the patients who received antifungal treatment immediately after presence of positive blood culture were alive. Only 2 cases (16.7%) of the patients who received no treatment were alive.
Yapar et al. [13] conducted a similar study on the incidence risk factors and outcome of the candidemia in patients in ICU and compared it with those ICU patients without candidemia. They reported an incidence of 12.3 per 1000 admissions in ICU. In our study also, 83.6 percent of the patients had central venous catheter. It seems that catheterization may be a risk factor for candidemia. Our study showed no difference in the outcome of the patients recieving Carbapenems, Glycopeptide, Cephalosporins, or Fluoroquinolones antibiotic classes. They reported a crude mortality rate of 43.9 percent at 30 days ICU residency. In our study with a mean ICU stay of 37 days, 69.1 percent of patients were expired. Literature review of the studies supported that about one third of candidemic cases happen in medical or surgical intensive care units and a mortality rate around 50 to 60 percent is expected for these patients [14-16]. These statistics are similar to our findings; however, mortality was slightly higher in our study.
The other point of our study was that we found no significant difference regarding using caspofungin or amphotericin as the treatment with better outcome in patients’ survival. A recent systematic review and meta-analysis out of eight relevant articles revealed no difference between echinocandins, voriconazole, or amphotericin B formulations as the first choice treatment and the regarding outcome of the critically ill patients [17]. Other studies on ICU patients reported no difference regarding the choice of antifungal treatment and the outcome of the patients. Garnacho-Montero et al. [18] in a Spanish retrospective study reported that the mortality rate was 37.4% in ICU patients who were treated with fluconazole and 31.9% in ICU patients under echinocandin treatment and this difference was not significant. Nagy et al. [19] in another study in ICU patients reported that treatment with fluconazole is not inferior than caspofungin, micafungin or amphotericin B in the outcome of candidemia patients. Mora-Durate et al. [20] also reported that caspofungin is at least as effective as amphotericin B for the treatment of invasive candidiasis and, more specifically, candidemia. It seems that the main predisposing factor for candidemia is the virulence of candida specie [21].
However, the main limit of the studies in the case of candidemia, especially those in intensive care units, is that the number of candidemia cases are few. Our study also had a total number of 55 candidemia cases and we tried to reach this sample size by adding two tertiary health centers to our study sample. It seems that the studies in case of candidemia should be done multi-centric. The larger sample size can overcome the limits in analyses. Putting this shortcoming away, our study was among the few studies in candidemia in ICU and especially in Iran. This can further help researchers to complete the gap in the data regarding candidemia in ICU.
Our study showed that 69.1 percent of the cases expired within a mean ICU stay of 37 days. Furthermore, there was no significant difference in outcome of the patients regarding using Caspofungin or Amphotericin. Our results also showed that timely initiation of antifungal regarding to the culture result may bring better outcomes as 66.7% of the patients who received antifungal immediately after a positive blood culture of candida survived.
The authors wish to express their appreciation for the financial support of Mashhad University of Medical Sciences and We would like to thank the clinical research development unit, Imam Reza Hospital, Mashhad University of Medical Sciences, for their assistance in this manuscript.
Authors have declared that no competing interests exist.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
