
Research Article | DOI: https://doi.org/10.31579/2641-0419/571
1Cardiac Medical Department, FANN Hospital.
2Cardiac Surgery Department, FANN Hospital.
*Corresponding Author: Momar Dioum, Cardiac medical department, FANN hospital.
Citation: Khadim Sene, Papa A. Diagne, Moina-Hanifa II, Papa Mouhamadou D. Fall, Sidy Lamine Sy, et al, (2026), Epidemiological, Diagnostic, Therapeutic and Evolutionary Profiles of Prosthetic Heart Valve Thrombosis: Cross-Sectional Study About 20 patients The National University Hospital Center of FANN, J Clinical Cardiology and Cardiovascular Interventions, 9(7); DOI:10.31579/2641-0419/571
Copyright: © 2026, Momar Dioum. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 March 2026 | Accepted: 20 April 2026 | Published: 28 April 2026
Keywords: prosthetic heart valve thrombosis; therapeutic compliance; thrombolysis; surgery
Background/Aim
The incidence of prosthetic valve thrombosis is rare, ranging from 0.1 to 5.7% patient/year, but represents a serious complication. Clinical manifestations are variable. Management is currently well codified but remains problematic in our countries due to the unavailability of emergency surgery and the lack of patient therapeutic education. The aim of our study was to evaluate the management of patients hospitalized for prosthetic heart valve thrombosis at the CHNU of FANN.
Materials and Methods
We conducted a cross-sectional, descriptive study from January 10, 2023 to January 10, 2025. All patients hospitalized for left-sided prosthetic heart valve thrombosis confirmed by transthoracic and/or transesophageal echocardiography and who received care at the CHNU of Fann were included.
Results
We collected 20 cases of prosthetic heart valve thrombosis, representing 3.27%. The mean age of patients was 32 ± 13 years with a sex ratio of 0.42. Mitral regurgitation was the leading cardiac condition (30%). Nineteen patients had a mechanical valve and one had a biological valve. Acenocoumarol was used in 85% of cases. PT-INR monitoring was irregular in 65% of cases. Therapeutic non-compliance was noted in 85% of cases. Symptoms were varied and dominated by dyspnea stage III/IV (NYHA) in 90% of cases. The prosthetic click was absent in 19 patients (100%). INR was below 2 in 55% of patients at the time of diagnosis. Mean mitral and aortic gradients were 22.84 mmHg and 70 mmHg, respectively. Therapeutically, thrombolysis was performed in 19 patients (95%) and redo surgery in 3 patients (15%). All patients were thrombolyzed with streptokinase with a success rate of 73.70%. The outcome was favorable in 75% of cases. Five deaths (25%) were recorded.
Conclusion
Prosthetic heart valve thrombosis, especially mechanical, was found predominantly in young subjects with a female predominance. The mitral prosthesis was the most affected. Poor therapeutic compliance and irregular follow-up were the main contributing factors. Thrombolysis was the treatment of choice in our context. Mortality remained significant.
Prosthetic valve thrombosis is defined as "any thrombus located near the valve (or attached to the valve), which interferes with valve function (or obstructs flow) and is not related to infection" [1-2]. The incidence of mechanical valve thrombosis is rare, ranging from 0.1 to 5.7% patient/year, but represents a serious complication that threatens the patient's life [2]. Mechanical prosthetic valve thrombosis is more frequent during the first year following surgery.
Various data have been reported in the literature, and the incidence may be underestimated for several reasons, including the prevalence of asymptomatic cases and the difficulty in establishing the diagnosis.
Clinical manifestations can range from reduced exercise capacity to more severe forms of acute heart failure such as acute pulmonary edema or cardiogenic shock. Sudden cardiac death may be the first manifestation of mechanical prosthetic valve thrombosis [3]. Obstructive or non-obstructive prosthetic thrombus can lead to systemic or cerebral embolism.
Thrombosis is favored by inadequate vitamin K antagonist therapy [4]. Cardiac echocardiography and/or transesophageal echocardiography combined with fluoroscopy constitute the diagnostic tools for prosthetic valve thrombosis.
Although the therapeutic management of thrombosis is currently well codified (American College of Cardiology (ACC)/American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines recommendations), it remains problematic in our countries due to the unavailability of data and emergency surgery [5-3].
It is in this context that we conducted this study with the general objective of evaluating the management of prosthetic heart valve thrombosis.
We conducted a cross-sectional study over 24 months, from January 10, 2023 to January 10, 2025. All patients hospitalized for left-sided prosthetic heart valve thrombosis confirmed by transthoracic and/or transesophageal echocardiography were included.
The study variables were as follows: age, gender medical history, valve characteristics, surgical data, type of VKA, last cardiology and surgical consultation, last cardiac echocardiogram, interval between prosthesis implantation and occurrence of thrombosis (early: less than 1 year; late: more than 1 year). Clinical data included: functional signs and symptoms, auscultation findings, and complications. From a paraclinical standpoint, electrical aspects and hemostasis assessment were studied. TTE +/- TEE assessed mean transmitral gradient (normal = 5 ± 3 mmHg; abnormal Greater-Than Sign 10 mmHg), mean transaortic gradient (normal less than sign 20 mmHg; abnormal Greater-Than Sign 30 mmHg), intraprosthetic thrombus, intraprosthetic regurgitation, effective valve area, and complete or incomplete leaflet blockage on TEE [3]. Fluoroscopy of the valves assessed leaflet mobility. TheMrapeutically, the variables were thrombolysis, redo surgery, and anticoagulant therapy. With respect to clinical outcome, two variables were studied: favorable and unfavorable (complications and death).
Data were collected using a standardized survey form, then entered and organized in Microsoft Office Excel spreadsheets (version 2021). A random double-check of 10% of forms was performed to control data entry errors and ensure data consistency.
Statistical analysis was performed using R software (version 4.3.1, 2023). Student's t-test, Chi² test, logistic regression were applied according to the nature of the variables and the objectives of the study. Results were interpreted with a significance threshold set at p less than sign 0.05.
During the period from January 10, 2023 to January 10, 2025, 611 patients were hospitalized in the intensive care units of the cardiology clinic of the CHNU of Fann, of whom 20 were admitted for prosthetic heart valve thrombosis, representing 3.27%. The mean age of patients was 32 ± 13 years, ranging from 19 to 65 years. The age group between 21 and 40 years was predominant, accounting for 60% of cases. A clear female predominance was noted (14 women and 6 men) with a sex ratio of 0.42.
Nineteen patients had a mechanical valve and one had a biological valve (Table I). Among mechanical valves, 14 were in the mitral position, 4 in the mitro-aortic position, and one in the aortic position. All patients had bileaflet mechanical valves, including 16 of the Carbomedics type and 3 of the St. Jude Medical type. Among mitral mechanical prostheses, seven (7) had a size of 27, and for aortic prostheses, two had sizes of 21 and 23. Tricuspid annuloplasty was performed in 10 patients.
| Mitral Valve | Aortic Valve | Mitro-Aortic | TOTAL | |
| Mechanical | 14 | 1 | 4 | 19 |
| Biological | 1 | 0 | 0 | 1 |
| TOTAL | 15 | 1 | 4 | 20 |
Table I: Distribution of valves by type and position
Among vitamin K antagonists, acenocoumarol was used in 17 patients. Two patients were on fluindione. Fourteen patients had a surgical follow-up interval of more than 1 year, and nine patients had a cardiology follow-up interval of more than 1 year. Half (n=10) of the patients had their last cardiac echocardiogram performed more than 1 year prior. PT-INR monitoring was irregular in 13 patients, and seventeen (17) patients were non-compliant with anticoagulant therapy. The mean duration of therapeutic interruption was 74 days, with a minimum of zero days and a maximum of 2 years. The interval between valve substitute implantation and occurrence of thrombosis ranged from 2 days for a postoperative thrombosis to 16 years. Nine thromboses (45%) occurred between 1 month and 5 years after implantation. Eight patients (40%) had thrombosis more than 5 years after the primary implantation.
Symptoms included NYHA class III/IV dyspnea in 18 patients. Three patients had motor deficits. Among complications, 4 patients had acute pulmonary edema and cardiogenic shock, and 2 patients had systemic embolism. The prosthetic click was absent in all cases.
Sinus rhythm was present in 14 patients. Five cases of atrial fibrillation (25%), one case of atrial flutter, and 6 patients with conduction disorders such as complete and/or incomplete bundle branch block were noted. Biologically, the mean INR was 2.42 and 11 patients had an INR below 2 at the time of diagnosis. Transthoracic echocardiography revealed a mean transprosthetic mitral gradient of 22.84 mmHg, ranging from 11 to 35 mmHg. Nineteen (19) patients had transprosthetic mitral gradients between 10 and 20 mmHg, and 4 patients had gradients above 30 mmHg (Figure 1). At the aortic level, one patient had a mean gradient of 70 mmHg. One patient had a thrombus in the left atrium. Transesophageal echocardiography performed in 15 patients (75%) showed echogenic intraprosthetic material (Figures 2A and 2B) and immobility of one of the leaflets in 80% of patients. Valve fluoroscopy was performed in 16 patients (80%). Figure 3 shows complete blockage of one leaflet, which was found in 10 patients (62.5%). Complete blockage of both leaflets was found in one patient (6.25%). Therapeutically, thrombolysis was performed in 19 patients (95%). All patients were thrombolyzed with streptokinase with a success rate of 73.70%. Systemic embolism occurred in 2 patients: one ischemic stroke and one acute limb ischemia. Table II shows the thrombolysis results. Redo surgery was performed in 3 patients (15%). Figure 4 shows a postoperative image of a mechanical prosthesis with an adherent thrombus. Ninety-five percent (n=19) of patients were on unfractionated heparin (UFH) and 17 patients had VKA bridging. One patient was on a combination of VKA and aspirin.of the 19 thrombolyzed patients, 5 died with no reduction in gradient.
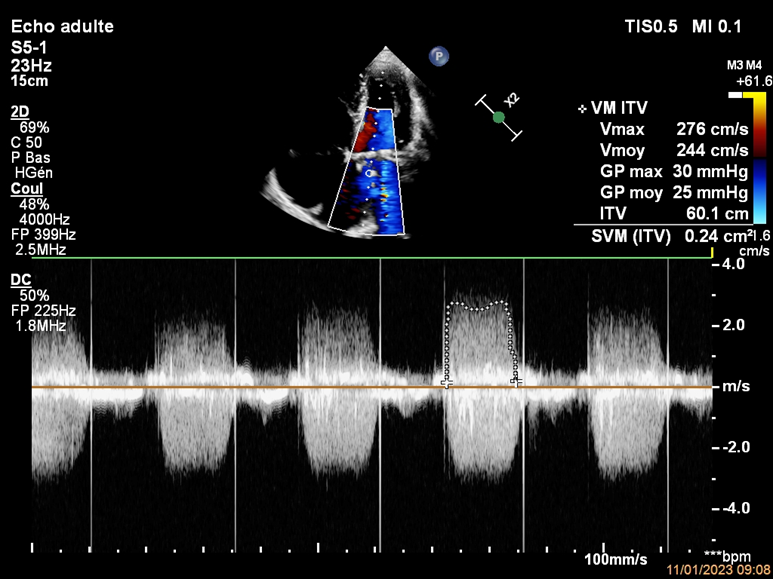
Figure 1: Echocardiographic image of mitral prosthetic thrombosis with mean gradient of 25 mmHg with continuous Doppler

Figure 2: 3D TEE image showing closure of both leaflets and presence of a thrombus (red arrow)
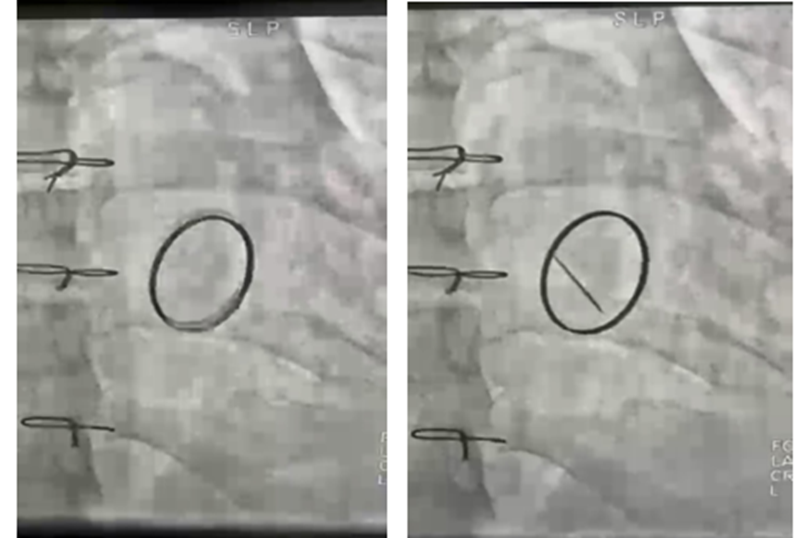
Figure 3: Fluoroscopy image of valves showing complete blockage of one leaflet
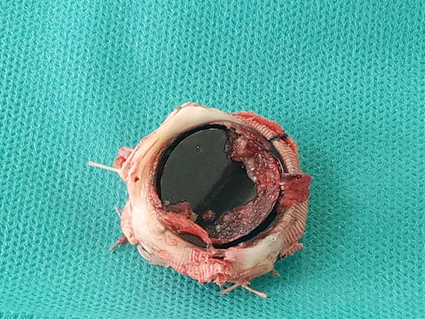
Figure 4: Postoperative image of a mechanical prosthesis in mitral position with an adherent thrombus
In our series, the prevalence was 3.89% of all patients operated on during the study period. This prevalence is close to that of Boukerroucha et al [6], who found 3.34%. The mean age of occurrence of prosthetic heart valve thrombosis in our patients was 32 ± 13 years. These results are close to those of the Kabbaj et al [7] study, which found a mean age of 38 years. Boukerroucha et al found 46.6 years [6]. The literature review confirms that this is a pathology of young subjects, especially in Africa.
A clear female predominance was noted, with a sex ratio of 0.42. The literature shows a female predominance of rheumatic heart disease [8-9], which explains the high prevalence of prosthetic valve thrombosis in female patients.
Supraventricular rhythm disorders were present in 6 patients, representing 30% of the cohort. These results were comparable to those of Durrleman et al [10], who found 41% atrial fibrillation. Atrial fibrillation is often associated with rheumatic valvulopathies and constitutes a risk factor for the occurrence of prosthetic valve thrombosis [11].
The majority of our patients were on acenocoumarol (85%). Similar data were reported by Patil et al [12], who found 69.1% on acenocoumarol alone. In our study, 85% of cases involved therapeutic non-compliance. These results were found in Kabbaj et al [7] (100%). Karthikeyan G et al [13] found 72% of patients presenting inadequate anticoagulation. This can be explained partly by the difficulty of maintaining lifelong anticoagulant therapy with rigorous clinical and biological monitoring. On the other hand, the young age of our patients carrying mechanical valves must be taken into account. A direct relationship between inadequate anticoagulation and the occurrence of valve thrombosis has already been established by several studies, as the present study suggests [14-15].
In our series, NYHA class III/IV dyspnea was found in 18 patients (90%). These results were comparable to those of Lafci et al [16], who found 88.9% of cases. Other authors found lower prevalences, such as Kabbaj et al (33%), Bouchenafa et al [17] (58%), and Patil et al (52.7%). This increase in the frequency of NYHA class III/IV dyspnea is due to diagnostic delay, as our patients tend to present at a late stage.
In our study, the INR was below 2 in 55% of patients at the time of diagnosis. These results were comparable to those of Patil et al, who found 55.5% of patients. Other authors such as Bouchenafa et al and Lafci et al found higher rates of 63% and 72.2%, respectively [17]. INR ineffectiveness is found in most studies, largely related to therapeutic interruption.
In our study, the mean transprosthetic mitral gradient was 22.84 mmHg. At the aortic level, one patient had a mean gradient of 70 mmHg. Boukerroucha et al found a mean transvalvular mitral gradient of 25.77 mmHg, and for the aortic valve, which was involved in five patients, the mean gradient was 57.1 mmHg [6].
In our study, thrombolysis was performed in 95% of cases with a success rate of 73.70%. All our patients were thrombolyzed with streptokinase. Patil et al used streptokinase in 78% of cases and urokinase in 22% of cases [12]. Consensus on the treatment of prosthetic valve thrombosis and recent systematic reviews suggest that the success rate of fibrinolytic treatment is at least 80% [18-19]. Furthermore, Sharma and Mewada [20], in a study of 48 patients, used streptokinase and reported 81% success. Singh S et al [21] also used streptokinase in 44 patients with PVT and reported 73% success.
In our series, the outcome was favorable in 75% of cases. Five deaths (25%) were recorded, including three cases of acute pulmonary edema, 1 cardiogenic shock, and 1 following infective endocarditis. Mahindru et al found a mortality of 22.95% and Kabbaj et al found 50% [7].
Prosthetic heart valve thrombosis, especially mechanical, was found predominantly in young subjects with a female predominance. The mitral prosthesis was the most affected. Poor therapeutic compliance and irregular follow-up were the main contributing factors. Thrombolysis was the treatment of choice in our context. Mortality remained significant.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
