
Research Article | DOI: https://doi.org/10.31579/2690-1919/266
1 ème Cardiology service of national hospital of Niamey/Niger
2 èmé Cardiology service of hospital Amirou Boubacar Diallo Niamey/Niger
3 eme Internal medicine department of general hospital of Niamey/Niger
*Corresponding Author: Hama Idrissa. ème Cardiology service of national hospital of Niamey/Niger
Citation: Hama Idrissa, AM Maliki, A Andia, Tinni Abdou R, H Harouna.et al (2022). Epidemiological Aspects of The Management of Heart Failure Patients Seen in Cardiological Consultations in The National Hospital of Niamey, J. Clinical Research and Reports, 11(4) DOI:10.31579/2690-1919/266
Copyright: © 2022 Hama Idrissa. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 August 2022 | Accepted: 20 August 2022 | Published: 04 September 2022
Keywords: epidemiological aspects; management; heart failure; HNN; niger
Background/Aim: Heart failure is defined as a structural or functional abnormality of the heart resulting in an inability to supply the tissues with oxygen at a rate commensurate with their needs.
Objective: To contribute to a better knowledge of the epidemiological aspects of the treatment of in charge of patient’s heart failure patients.
Materials and Methods: This is a prospective, cross-sectional study conducted over a period of 6 months (February 2020 to October 2020 without April et May due to Covid)
Result: Thus, our sample consisted of 300 cases. The average age was 56.9 +13.7 years with extremes ranging from 19 to 98 years. Housewives were the most represented at 43.7%. High blood pressure and sedentary lifestyle were the most common DRFs in 95% of the patients, followed by obesity in 22.3%. In 61.3% of the cases, patients knew they had heart disease but did not know the type. Unusual shortness of breath on exertion was the main sign that prompted patients to consult a doctor (67.7%). Only 2% weighed themselves regularly. All of our patients (99%) were aware of the recommendation for sodium restriction and more than half (58.3%) had adapted to a low-salt diet. Only 23.2% of our patients drank less than 1.5L per day. 29.7% of our patients were not physically active. Regarding treatment, diuretics were the most used as specific treatment in 64.3% of cases and antiplatelet agents in 12.3% of cases.
Conclusion: Our study has highlighted educational gaps in the heart failure population. Further studies may help to initiate a therapeutic education approach for patients in order to improve their quality of life and Morbi-mortality.
Known to physicians since ancient times, heart failure (HF) is defined as a structural or functional abnormality of the heart resulting in an inability to supply the tissues with oxygen at a rate commensurate with their needs. The European Society of Cardiology (ESC) treatment guidelines distinguish between three types of heart failure: heart failure with reduced ejection fraction (due to contractile failure), with moderately reduced ejection fraction and with preserved ejection fraction (due to insufficient myocardial relaxation) [1].
Heart failure is considered a major public health problem in industrialised countries. Its prevalence is estimated to be between 3 and 20 per 1000 and increases considerably with age. [2]
According to the World Health Organisation (WHO), the number of people suffering from heart failure in the world is estimated at twenty million and the five-year mortality rate of these people is between 50% and 60% [2] In Niger, studies on heart failure in 2001 and 2013 showed a respective frequency of 10% and 35.15% of patients hospitalised, i.e. an increase in the frequency of the disease.
[3] The benefits of therapeutic education (improved quality of life, reduced morbidity and mortality) have made it essential for the management of heart failure, as with other chronic diseases such as diabetes, chronic renal failure, asthma and chronic obstructive pulmonary disease (COPD). [1 ,4] Evaluate the level of prior knowledge of patients and get them to adhere to the care proposals offered to them by medical community.
Background/Aim:
To contribute to a better knowledge of the epidemiological aspects of the management of heart failure patients at the HNN
Our study is prospective and cross- sectional conducted over a period of 6 months, from February 2020 to October 2020. We suspended 2 months because of the corona virus (Covid 19).
Our study included: Patients, regardless of sex, who were seen in cardiology consultations. Any patient who had presented at least once in their history symptoms or signs of heart failure (exertional dyspnoea, orthopnoea, peripheral oedema, jugular turgidity...) [Protocol].
A functional cardiac abnormality was known or strongly suspected (old or poorly controlled hypertension) [1].
Patients who did not give consent and were not considered to have heart failure were excluded from the survey.
The data from our questionnaire were collected on a 5-page survey form with the following parameters: patient identity, cardiovascular risk factors, assessment of knowledge of diagnosis, assessment of monitoring of warning signs, assessment of knowledge of and compliance with treatment.
The advent of COVID 19 and the non-consent of some patients. Data collection was manual through a survey form
The data were entered and analysed using Epi info version 7.2.2.3 and Microsoft Word and Microsoft Excel 2013
We collected 300 respondents, 66.5% of whom were women. The average age of the patients was 56.9 years with a standard deviation of 13.7 years and extremes of 19 and 98 years. The 46 to 75 age group was the most represented with 74.7% of patients. The patients came from Niamey in 68.3% of cases. The patients were housewives in 43.7% of cases.
Figure 1: Distribution of patients by gender
The Zarma ethnic group was the most represented 53.7% of the cases. The average body mass index was 25.9 + 4.9 kg/m2. 22.3% of our patients were obese. 95.95, ..
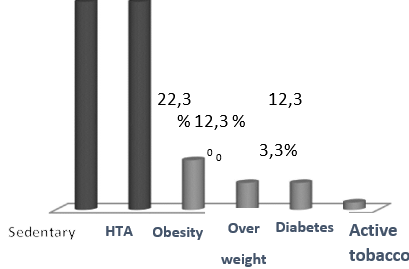
Figure 2: Distribution of patients according to risk factors
The patients were sedentary and hypertensive in 95% of cases. In 61.3% of the cases, the patients admitted to having a heart disease but did not know the type. Patients measured their weight less than once a week in 98% of cases. Unusual shortness of breath on exertion and fatigue were signs that prompted a visit to the doctor in 67.7% and 51.7% of cases respectively. According to 99.7% of the respondents, there was no link between shortness of breath and water retention. The patients were on diuretic therapy in 64.3% of cases.
Face 3: Distribution of patients according to knowledge of their pathology.
The patients stated that they had never failed to take their medication in 88.7% of cases. Heart failure patients should limit their salt intake in 99% of cases. The patients could not estimate their daily water consumption in 77% of the cases. For those patients who could estimate their daily water consumption, 23.2% estimated it to be less than 1.5 litres. Aromatic spices and commercial soup were high in salt according to the patients in 98.7% and 96% of the cases respectively. Cases.
Patients stated that physical activity is recommended for heart failure patients in 93% of cases. Patients were physically active for more than one hour and thirty minutes in 48.6% of cases. 2/3 of our patients practised one physical activity per week. Walking was the physical activity practiced by all patients. More than half of the patients consumed about 5g of salt per day. None of our patients had any knowledge of the exact amount of salt consumed per day by a heart failure patient. Heart failure requires life-long treatment according to 61.7% of the patients. The measurement of blood pressure was necessary for the follow-up of heart failure patients according to 99.3% of the patients.

Table 1: Distribution of patients by follow-up for heart failure
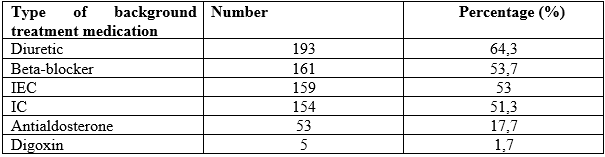
Table 2: Distribution of patients according to the type of drug used in specific treatment
As background treatment, diuretics were most commonly used in 64.3% of patients followed by beta-blockers in 53.7% and ACE inhibitors in 53%. The most frequently used non- specific treatment was antiplatelet agents in 12.3% of cases followed by statins.
Our study showed a predominance of women seen in cardiology consultations for heart failure: 66.5% of cases against 33.5% of men with a sex ratio of 0.5. This frequency is higher than that of Mahamane B. [3] in 2001 in Niger and Garba F. [5] in 2020 in Niger who found respectively 58.9% and 58.3%.
Our results are contrary to those of Moctar M. [4] in 2013 in Niger who found a male predominance of 53.6%. This female predominance may be linked to the fact that certain etiologies heart failure is not found in men, such as postpartum cardiomyopathy.
In our series, the age range between 46 and 75 years is the majority with 74.7%. Our results are in line with those of Ghita K. [5] in 2017 in Morocco who found 80% for the 50 to 79 age group. On the other hand, Hawa J. [7] n 2018 in Mali found lower results at 44.1%. This could be explained by the fact that heart failure is a disease of the elderly.
The patients came from Niamey in 68.3% and from Tillabery in 13%. Our results are similar to those of Salifou S. [8] in 2014 in Niger who found 65.9% for Niamey and 19.5% for Tillabery. On the other hand, Mahamane D. [3] found a preponderance of patients coming from the region of Tillabery 47.59% and Niamey in 24.10%.
In our series 43.7% of the patients were housewives. Our results are similar to those of Salifou S. [8] and Hawa J. [7] who found respectively 62.1% and 39%. This could be explained by the predominance of women in our study and especially the low rate of schooling of women/girls in our country. Zarma are the most represented with 53.7%. Our results are comparable to those of Hamza B. [9] in 2018 in Niger, which recovered 60% of zarma.
In our study, hypertension was found in 93% of patients. Our results are superior to those of Hawa J. [7] and Salifou S. [8] with respectively 42.2% and 63.4%. Other DRFCs such as smoking, diabetes and obesity were less common in our patients.
The first question asking the patient if they have heart disease, 61.3% or 184 cases answered that they have heart disease but without knowing the type. Our results are inferior to those of Guillaume L. [1] in 2017 in France who found that 71.37% of the patients responded that they had a heart disease.
In our study only 2% of patients reported weighing themselves once or twice a week compared to 98% who weighed themselves less than once a week. Our results are lower than those of Guillaume L. [1] and Bruni V. 62 et a1 [11] who found 48.2% and 61% respectively. This could be explained by the fact that the majority of our patients have no education.
In our series, 66.8% of patients consulted for unusual breathlessness on exertion compared to other symptoms. Our results agree with those of Maire-Edlinger A. [10] in 2011 in France and Guillaume L. [1] who found respectively 90% and 90.6%. In our study, 64.3% of our patients were treated with a diuretic. This is comparable to the results of Guillaume L. [1] who found 53.1%.
In our sample 93% of the patients recognized that physical activity is recommended in heart failure patients. Our results are similar to those of Guillaume L. [1] who found 93.8%. Patients who were physically active represented 70.3% of our sample. Our results are in line with those found by Bruni V. et al [11] in 2012 in France which found 72%. The most common type of activity iswalking, accounting for 69.4%.
In our study, 97.1% of patients said that a heart failure patient should limit salt intake. Guillaume L. [1] found lower results, 81.3%. In our series 58.3% of our patients had adapted a low-salt diet. Our results are lower than those found by Maire-Edlinger A. [10] and Bruni
V. et at. [11] with 76% and 83% respectively For 26.6% of patients, heart failure patients have to limit their cholesterol intake, 16.4% for sugar intake and only 2.3% for water intake. This could be explained by the fact that in society, heart diseases such as hypertension and heart failure are considered as salt-related diseases. Of the patients who were able to estimate their daily water only 23.2% were able to estimate it as less than 1.5 liters. The results are lower than those of Guillaume L. [1] who found 78.1%. In our series, 60.9% of the patients replied that they were aware that their CI required life-long treatment. Guillaume L. [1] found higher results at 87.5%. In our study 99.8% of patients considered that knowing more about their disease would help them to live better. Our results are comparable to those of Guillaume L. [1] who found 93.8%.
The most frequently associated non- specific treatment for CI was antiplatelet agents (12.3%) followed by statins (7%) and anticoagulants in 4% of cases. Contrary to Guillaume L. [1] who found a predominance of anticoagulants in 50% followed by statins in 43.8% and antiplatelet agents in 34.4%.
For the specific treatment of IC, diuretics were the most used (64.3%) followed by beta-blockers (53.7%) then ACE inhibitors (53%). Our results are contrary to those found by Théo P. et al [12] in France in 2020 who found a predominance of beta- blockers (81.6%) then diuretics (75.5%) then ACE inhibitors (71%).
Heart failure is a chronic disease with a very high morbidity. Its diagnosis remains difficult, its treatment rarely optimised. The many efforts made have not made therapeutic education accessible to all patients.
At the end of the study, it was found that the population was mostly elderly people in their sixties who lived mainly in urban areas. More than half of our patients were aware of their heart disease but did not know the type, and all of our patients knew that a person with heart failure should limit their salt intake.
Thus, half of the patients had a lack of understanding of the disease, its mechanisms, and the usefulness and importance of treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
