
Research Article | DOI: https://doi.org/10.31579/2768-0487/038
*Corresponding Author: Mesbah Uddin Ahmed, MS in Microbiology, Bangladesh University of Health Sciences.
Citation: S Begum, S Ferdousi, Iqbal H Chowdhury, Mesbah U Ahmed, A.N. N Ahmed. (2021) Eosinopenia as a Marker of Sepsis in Intensive Care Unit Patients. Journal of Clinical and Laboratory Research. 3(2); DOI:10.31579/2768-0487/038
Copyright: © 2021 Mesbah Uddin Ahmed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 July 2021 | Accepted: 06 August 2021 | Published: 16 August 2021
Keywords: absolute eosinophil count (AEC); sepsis; intensive care unit (ICU); receiver operating characteristic curve (ROC)
Sepsis is one of the most common cases of mortality and morbidity in the intensive care unit (ICU). This study was done to evaluate eonsinopenia as a marker of sepsis in intensive care unit patients. This cross sectional study was carried out in the Department of Clinical Pathology, Bangabandhu Sheikh Mujib Medical University, Dhaka from March 2012 to February 2013. Absolute Eosinophil Count (AEC) was done by automated cell counter and rechecked manually microscopically. In this study 74 suspected case of sepsis were enrolled from intensive care unit, BSMMU, Dhaka. Out of these patients 34 were included in the infection group and 40 in the non-infection group depending on blood culture report. The area under ROCcurve was 0.765 in current study. At the cutoff valve of AEC< 40 cell/cumm, the sensitivity and specificity of AEC for diagnosis of sepsis was 72.5% and 61.8% respectively. This present data revealed that decreased absolute eosinophil count was significantly associated with sepsis. So eosinopenia may be a reliable marker for early diagnosis of sepsis.
Sepsis is one ofmost common causes of mortality and morbidity in the intensive care unit (Abidi et al., 2008). Despite continuing advances in diagnosis and treatment, sepsis remains one of the important causes of higher mortality and morbidity. As the diseases progress more rapidly, the mortality rate is higher in sepsis. Early diagnosis of sepsis plays an integral role in the morbidity and mortality of patients admitted tothe intensive care unit (Rey etal., 2007). Sepsis is a systemic inflammatory response to infection, manifested by two or more of the following condition as a result of infection: Temperature >380c or < 360c>90 beats/min, Respiratory rate > 20 breaths/min and white cell count>12,000/cumm,<4000>10% immature (band) forms (Abidi et al., 2008, Bone et al.,1992). Sepsis was documented more than 35% of patients during their ICU stay (vincent et al., 2006). The hospital mortality ranged from 16.9% for non-infected patients to 53.6% for patients who had infection at ICU. An estimated 7,50,000 cases of sepsis occur annually in the United States and the mortality rate is about 30%. The incidence will increase by 1.5 per year (Curtiset al, 2002). Normal eosinophil count is 40-400 cells/cu mm of blood (Firkin, 2006). Eosinopenia refers to a reduction in the normal number of circulating eosinophils (Bain, 2003). The level of eosinophils is normally tightly regulated (Abidi et al., 2008). Eosinophil production is regulated by IL-3, IL-5 and granulocyte macrophage colony stimulating factor (GM-CSF). Without these cytokines eosinophil cannot survive. These cytokines are not significantly activated in patients with sepsis. It is belived to be main mechanism of eosinopenia is sepsis (Wibrow et al., 2011). Eosinopenia during infection is also enhanced by chemotactic substance such as C5a (Shaaban et al., 2010). This substance causes migration of eosinophils into the inflammatory site (Jagadesh et al., 2012). So eosinopenia caused by migration of these cells from the vascular space, inhibition of bone marrow release and eventual decrease in marrow production (Harris et al., 1987). Sepsis and non-infectious systemic inflammatory response syndrome (SIRS) produce every similar clinical feature (Rey et al., 2007). Therapy and outcome differ greatly between patient with and those without sepsis. The widespread use of antibiotics for all such patients is likely to increase antibiotic resistance and toxicity (Gibot et al., 2004). The definitive diagnosis of sepsis is made by a positive culture, which requires a minimum of 48-72 hours (Reimer et al., 1997). Asthe culture procedure is costly and longer time required, other tests in the diagnosis of sepsis are required (Vincent et al., 2010). Several markers like C-reactive protein, procalcitonin, lactate, Interleukin-1 (IL-1), Inter leukin-6 (IL-6), Tumor necroting factor (TNF) etc have been reported to predict sepsis (Shaban et al., 2010). Most of these markers are expensive and not easily accessible to clinicians. They are not ideal for early diagnosis of sepsis. Among them blood eosinophil count is simple, easy, quick, less expensive and reliable marker of sepsis (Shaabanet al., 2010, Rinaldo et al., 1999). It is part of complete blood countwhich is done as routine laboratory test. It can establish the presence or absence of infection and may assist clinicians regarding early administration of antibiotics. It reduces widespread use of antibiotic, mortality and sepsis related complications, the cost of treatment and shorten the hospital stay. So this study was carried outto evaluate the diagnostic sensitivity of eosinopenia for detection of sepsis in ICU patients.
This cross-sectional study was conducted at the Department of Clinical Pathology incollaboration with Department of Anesthesia, Analgesia and Intensive care Medicine and Department of Microbiology and Immunology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka from March 2012 to February 2013. 74 suspected sepsis patients who were admitted in the Intensive Care Unit, BSMMU, Dhaka were enrolled for the study. Study population was divided into infection and non-infection group depending on blood culture reports.34 patients were positive for culture who were included in infectiongroup and 40 patients were negative for culture who were included inthe non-infection group. Prior to the commencement of this study, the research protocol was approved by the Institutional Review Board (IRB) of BSMMU, Dhaka. After taking written consent from patient’s attendant blood sample were collected by venipuncture from each patient with all aseptic precaution. 2ml blood was collected from completed blood count including absolute eosinophil count. Within 2 hours CBC count including eosinophil count was done by automated cell counter and rechecked manually microscopically. Blood sample from patients who were receiving antibiotics inoculated in faster antibiotic neutralization bottles for automated blood culture and patients who were not receiving antibiotics were inoculated in conventional blood culture bottles for conventional blood culture. Single set of culture was done for each patients. All theblood culture bottles were then transported immediately to the Department of microbiology and Immunology, Bangabandhu Sheikh Mujib Medical University for further processing. Blood culture reports were collected and recorded in data sheet from report. All data were recorded systematically in a preform data collection sheet and expressed as mean±standard deviation (SD). Receiver operating characteristic curve and the respective are undercurves was calculated for eosinophils. In a receiver operating characteristic (ROC) curve the true positive rate (Sensitivity) is plotted against the false positive rate for different cut-off points of a parameter. Each point on the ROC curve represents a sensitivity/specificity pair corresponding to a particular decision threshold. Sensitivity, specificity were calculated at the best cut off value. Statistical analysis was done by using statistical package for social science SPSS 17.0. p value <0>
In this study, 74 patients were divided into two group according to blood culture findings. Out of these patients 34 were included in the infection group and 40 in the non-infection group. The mean ± SD of AEC was found 18.3±11.4 cells/cu mm in infection group and 145.0±57.7 cells/cu mm in non-infection group. In infection group AEC was lower than non-infection group. The result was statistically highly significant (p<0>
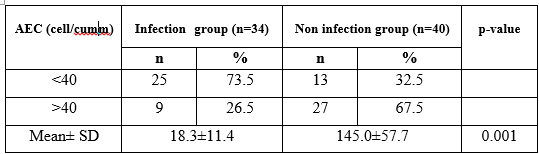
pvaluereachedfromunpaired t-test
Table 1 shows the AEC of the study patients. AEC <40>40 cells/Cumm was found 9(26.5%) in infection group and 27(67.5%) in non-infection group. The mean AEC was found 18.3±11.4 cells/cumm in infection group and 145.0±57.7 cells/cumm innon infection group. The difference was statistically significant between two groups.

Receiver-operating characteristic (ROC) curve of AbsoluteEosinophil Count (AEC) forprediction ofinfection
The area under the receiver-operating characteristic (ROC) curvesfor the infection predictors is depicted in the following table. Based on the ROC curves AEC had the best area under curve. ROC were constructed using AEC of the patients with infection, which gave a AEC cutoff value of (<40>)

This cross sectional study carried out to evaluated absolute eosinophil count for early diagnosis of sepsis compared with gold standard blood culture. Inthis study mean value of absolute eosinophil count were 18±11.4 cells/cu mm in infection group and 145±57.4 cells/ cu mm in no infection group. Similar findings were observed in the study done by Abidi et al (2008), Shaban et al (2010), Kadir et al (2012), Gil et al (2003). From the study of Kadir et (2012) mean absolute eosinophil count were 23±46 cells/cu mm in sepsis and 143±101 cells/ cumm in patients without sepsis. This finding was similar to our study. In previous study the sensitivity of eosinopenia in sepsis patient had a resonable range of variation. Our study showed sensitivity 75.5% which was consistent with thestudy of Abdi et al (2008). From the study of Abidi et al (2008), Bayram el al (2012), Lopez et al (2010), Gil et al (2003), sensitivity was 71%, 61.4%, 64.8%, 64% respectively. These result were nearly consistent with our study. The present study has also defined the specificity of eosinopenia in sepsis patients. Our study showed specificity of eosinopenia for diagnosis of sepsis was 61.8% which was consistent with the study of Shaban et al (2010). According to their observation specificity was 65%. From the study of Lopez et al(2010), Moura etal (2011) specificity was 70.9%, 71% respectively. These results were nearly consistent with our study. The area under ROC curve for the sepsis was depicted in our study. The area under receiver operating characteristic curve was 0.765 in current study. This is similar to the observation of the study done by Shaban et al (2010). According to their observation the area under receiver operating characteristic curvywas 0.72 which is consistent with our study. Considering the sensitivity specificity, thisstudy impliesthat eosinopeniaisreliableas adiagnostic tool for sepsis. The level of eosinophils in the body is normally tightly regulated (Abidi et al., 2008). Eosinophil production is requlated by IL-3, IL-5 and granulocyte macrophage colony stimulating factor. Without these cytokines, eosinophil cannot survive. These cytokines are not significantly activated in patients with sepsis. It is believed to be main mechanism of eosinopenia in sepsis (Wibrow et al.). Eosinopenia during infecton is also enhanced by chemotactic substance such as c5a (Abidi et al., 2008, Shaabon et al., 2010). Eosinopenia may be the result of migration of eosinophils into theinflammatory site itself due to release of the chemotactic factor of acute inflammation in to the circulation (Jagadesh et al., 2012). So eosinopenia caused by migration of these cells from the vascular space, inhibition of bone marrow release and eventual decrease in marrow production (Harris et al., 1987).
Form this study, it can be concluded that AEC is significantly lower in patients with sepsis. Eocinopenia may be a useful marker to distinguish the infected from non-infected patients. An early diagnosis of sepsis is made by absolute eosinophil count thatcan be obtained from routine laboratory test (Complete bood Count) which is simple, quick, cost effective and readily available. In our study eosinopenia provide an effective guideline to make decision regarding judicious use of antibiotic therapy which will be lifesaving and minimize the risk of emergence of resistant organism due to misuse of antibiotics.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
