
Case Report | DOI: https://doi.org/10.31579/2639-4162/055
1 Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh.
*Corresponding Author: Richmond Ronald Gomes (2022). Enteric Encephalopathy: An Old Archenemy. J. General medicine and Clinical Practice. 5(1); DOI:10.31579/2639-4162/055
Citation: Richmond Ronald Gomes (2022). Enteric Encephalopathy: An Old Archenemy. J. General medicine and Clinical Practice. 5(1); DOI:10.31579/2639-4162/055
Copyright: © 2022 Richmond Ronald Gomes, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 October 2021 | Accepted: 27 December 2021 | Published: 03 January 2022
Keywords: typhoid; salmonella; encephalopathy; pulse steroid
Typhoid fever is the name given to the illness caused by the bacterium Salmonella Typhi, a member of the Salmonella family. Typhoid fever is spread through food and water contaminated by animal and human feces. Typhoid fever is very rare in the United States and other developed nations, and it is more common in underdeveloped nations, particularly Latin America, Asia, and Africa. Typhoid fever has a wide variety of presentations that range from an overwhelming multisystemic illness to relatively minor cases of diarrhea with low-grade fever. The classic presentation is fever, malaise, diffuse abdominal pain, and constipation. Untreated typhoid fever may progress to delirium, obtundation, intestinal hemorrhage, bowel perforation, and death within 1 month of onset. Survivors may be left with long-term or permanent neuropsychiatric complications. Here, we present a 30 years old nurse who presented with fever, constipation and diagnosed as typhoid fever. While on treatment, she developed abnormal behavior. CSF was sterile. Neuro imaging was normal. Considering typhoid encephalopathy she was treated with high dose pulse steroid. She showed significant improvement. Thus, all clinicians should keep in mind the possibility of typhoid encephalopathy as a rare complication of typhoid fever.
Typhoid fever, also known as enteric fever, is a potentially fatal multisystemic illness caused primarily by Salmonella enteric serotype typhi and, to a lesser extent, S enterica serotypes paratyphi A, B, and C. The terms typhoid and enteric fever are commonly used to describe both major serotypes. S typhi has been a major human pathogen for thousands of years, thriving in conditions of poor sanitation, crowding, and social chaos. It may have been responsible for the Great Plague of Athens at the end of the Pelopennesian War. [1] The name S typhi is derived from the ancient Greek typhos, an ethereal smoke or cloud that was believed to cause disease and madness. In the advanced stages of typhoid fever, the patient's level of consciousness is truly clouded. Although antibiotics have markedly reduced the frequency of typhoid fever in the developed world, it remains endemic in developing countries. [2] Typhoid fever can feasibly be eradicated completely if advances in its diagnosis, prevention and treatment are financially supported by governments and philanthropists and if the healthcare infrastructure in regions with endemic Typhoid fever are improved [3].
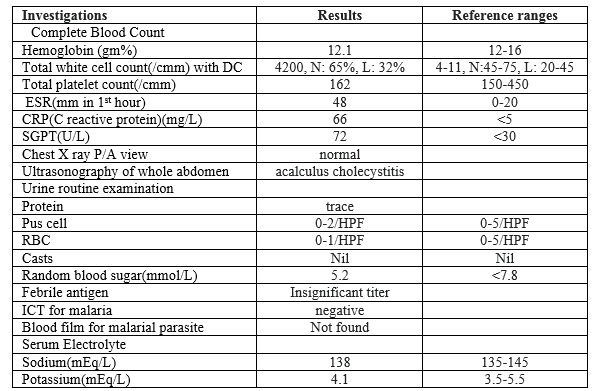
A 30 years old nurse, not known to have diabetes, hypertension, bronchial asthma presented with the complaints of high presented to us with the history of initial low grade then high grade, continued fever (maximum recorded temperature 104oF) associated with chills but not with rigor, headache, bodyache and dry cough for 4 days, vomiting for several times and severe prostration for 1 day. She denied any altered consciousness, convulsion, chest pain, palpitation, shortness of breath, abdominal pain or distension, burning micturition, joint pain or skin rash or bleeding from any site. She had no recent history of travel to malarial endemic zone. She also denied any previous history of tuberculosis or contact with any patient with active tuberculosis. On examination, she was toxic, conscious, oriented, febrile (temperature 102oF), with pulse 92 beats/min, with normal rhythm and volume, Blood pressure was 110/70 mm of Hg. There was diffuse blanching erythema. There was no signs of meningeal irritation. Fundoscopy was normal. Other systematic examination including general examination, cardiovascular system, respiratory system, alimentary system and nervous system examination revealed no abnormalities. Initial laboratory investigations is plotted in table 1.
As she denied hospitalization, she was started tablet ceftibuten 400 mg once daily along with anti-pyretic and anti-emetic pending blood C/S report. Three days after starting antibiotics, her roommate complained of episodic irrelevant behavior with muttered speech. In the meantime, her blood C/S showed growth of salmonella typhi sensitive to ceftriaxone. She was urgently hospitalized. Injection ceftriaxone was started at the dose of 2 gram twice daily. Repeat serum electrolyte and random blood sugar result was non-significant. So CT brain and CSF analysis was done which were also noncontributory (table 2). Thus, the diagnosis of typhoid encephalopathy was considered and she was given pulse methylprednisolone 1 gram daily for 3 days along with ceftriaxone. With treatment she showed significant recovery with subsidence of fever and she became conscious oriented with normal speech. Ceftriaxone was continued for 10 days. During discharge she was hemodynamically and neurologically stable.

The cause of typhoid fever is the bacterium Salmonella enterica subsp. enterica serovar Typhi growing in the intestines, peyers patches, mesenteric lymph nodes, spleen, liver, gallbladder, bone marrow and blood.4,5 Typhoid is spread by eating or drinking food or water contaminated with the feces from an infected person.6 Risk factors include limited access to clean drinking water, and poor sanitation.7 Those who have not yet been exposed to the pathogen and ingest contaminated drinking water or food are most at risk for developing symptoms.5 As far as we currently know, only humans can be infected; there are no known animal reservoirs. [6]
All pathogenic Salmonella species, when present in the gut are engulfed by phagocytic cells, which then pass them through the mucosa and present them to the macrophages in the lamina propria. Nontyphoidal salmonellae are phagocytized throughout the distal ileum and colon. With toll-like receptor (TLR)–5 and TLR-4/MD2/CD-14 complex, macrophages recognize pathogen-associated molecular patterns (PAMPs) such as flagella and lipopolysaccharides. Macrophages and intestinal epithelial cells then attract T cells and neutrophils with interleukin 8 (IL-8), causing inflammation and suppressing the infection. [8,9]
In contrast to the nontyphoidal salmonellae, S typhi and paratyphi enter the host's system primarily through the distal ileum. They have specialized fimbriae that adhere to the epithelium over clusters of lymphoid tissue in the ileum (Peyer patches), the main relay point for macrophages traveling from the gut into the lymphatic system. The bacteria then induce their host macrophages to attract more macrophages. [8] S typhi has a Vi capsular antigen that masks PAMPs, avoiding neutrophil-based inflammation, while the most common paratyphi serovar, paratyphi A, does not. This may explain the greater infectivity of typhi compared with most of its cousins. [10]
Typhoidal salmonella co-opt the macrophages' cellular machinery for their own reproduction 11 as they are carried through the mesenteric lymph nodes to the thoracic duct and the lymphatics and then through to the reticuloendothelial tissues of the liver, spleen, bone marrow, and lymph nodes. Once there, they pause and continue to multiply until some critical density is reached. Afterward, the bacteria induce macrophage apoptosis, breaking out into the bloodstream to invade the rest of the body. [9]
The bacteria then infect the gallbladder via either bacteremia or direct extension of infected bile. The result is that the organism re-enters the gastrointestinal tract in the bile and reinfects Peyer patches. Bacteria that do not reinfect the host are typically shed in the stool and are then available to infect other hosts. [2,8]
Chronic carriers are responsible for much of the transmission of the organism. While asymptomatic, they may continue to shed bacteria in their stool for decades. The organisms sequester themselves either as a biofilm on gallstones or gallbladder epithelium or, perhaps, intracellularly, within the epithelium itself. [12] The bacteria excreted by a single carrier may have multiple genotypes, making it difficult to trace an outbreak to its origin. [13]
Typhoid fever occurs worldwide, primarily in developing nations whose sanitary conditions are poor. Typhoid fever is endemic in Asia, Africa, Latin America, the Caribbean, and Oceania, but 80% of cases come from Bangladesh, China, India, Indonesia, Laos, Nepal, Pakistan, or Vietnam.14 Within those countries, typhoid fever is most common in underdeveloped areas. Typhoid fever infects roughly 21.6 million people (incidence of 3.6 per 1,000 population) and kills an estimated 200,000 people every year. [15]
The most common symptom is prolonged fever which occurs in about 75% of patients and can last up to four weeks if left untreated. Although abdominal pain and constipation/ diarrhoea are considered classical symptoms, they occur in only about 35% of the population.1 This patient had fever for ten days before admission to TH Jaffna and did not have any gastrointestinal symptoms. Other symptoms such as headache, chills, sweating, anorexia, arthralgia may also occur in patients with enteric fever. Around 10
Typhoid delirium is a known neurological complication of typhoid fever which has not been previously reported in Sri Lanka. This patient presented on day nine of fever with typical muttering delirium and picking at bedclothes and imaginary objects. The diagnosis could have easily been missed if not for the high degree of clinical suspicion. Early initiation of specific antibiotics ensured complete recovery without residual complications.
None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
