
Clinical Images | DOI: https://doi.org/10.31579/2690-4861/480
1Department of Neurosurgery, The First Affiliated Hospital of Soochow University, Suzhou, China.
# Jiandong Zhu and Xin Jin contributed equally to this work.
*Corresponding Author: Jiang Wu and Zhengquan Yu, Department of Neurosurgery, The First Affiliated Hospital of Soochow University, 188 Shizi Street, Suzhou 215006, Jiangsu, China, szjiangwu@163.com and zhengquan.yu@neurosci.com.cn
Citation: Jiandong Zhu, Xin Jin, Zhengquan Yu, and Jiang Wu, (2024), Endovascular Interventional Treatment of Intracranial “Giant-Octopus”, International Journal of Clinical Case Reports and Reviews, 18(2); DOI:10.31579/2690-4861/480
Copyright: © 2024, Zhengquan Yu, and Jiang Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 May 2024 | Accepted: 13 June 2024 | Published: 25 June 2024
Keywords: apical aneurysm; dizziness; abnormalities; Giant-Octopus
A 66-year-old female patient, because the dizziness worsened in the past half month, the patient went to the local hospital for a head computed tomography angiography (CTA) examination; the head CTA showed that the basilar artery apical aneurysm. The patient was transferred to our unit from a regional hospital.
A 66-year-old female patient, because the dizziness worsened in the past half month, the patient went to the local hospital for a head computed tomography angiography (CTA) examination; the head CTA showed that the basilar artery apical aneurysm. The patient was transferred to our unit from a regional hospital.
In the past ten years, the patient with hypertension has regularly taken amlodipine besylate, but blood pressure is not monitored frequently. She had no family history of intracranial aneurysm or arteriovenous malformation. The immediate cause of her visit was the worsening of her dizziness.
After admission, the patient was clinically well with a blood pressure of 138/78 mmHg, the pulse of 85 beats per min, respiratory rate of 18 breaths per min, and oxygen saturation of 98% on room air. None of the laboratory investigations showed any significant abnormalities.
The patient underwent cerebral angiography after admission. During the operation, the apical aneurysm of the basal artery was seen, and the size was about 4.1mm×6.3mm (Figure).
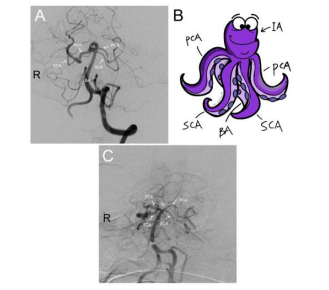
BA: basilar artery, SCA: superior cerebellar artery, PCA: posterior cerebral artery, IA: intracranial aneurysm.
Figure 1. Apical basilar artery aneurysm. (A)Cerebrovascular digital silhouette angiogram showing a basilar parietal aneurysm. (B)Schematic showing the vessel structure surrounding the aneurysm. (C)Disappearance of aneurysm after transcatheter intracranial aneurysm embolization procedure.
Based on this result, we performed transcatheter intracranial aneurysm embolization; the surgery went smoothly. Postoperative angiography showed dense embolization of the spring ring in the aneurysm, and the aneurysm-carrying artery was unobstructed.
The patient was discharged with no significant complaints of discomfort, and the dizziness disappeared. After discharge, she periodically took oral aspirin and clopidogrel tablets for anti-plate therapy. During regular outpatient follow-ups, the patient recovered well.
Apical basilar artery aneurysms are located in the deep interpeduncular pool of the posterior cranial fossa, adjacent to critical neural structures, and closely associated with several major penetrating arteries [1]. Microsurgical treatment is difficult and risky, especially for wide-necked aneurysms, and it is difficult to obtain satisfactory results by clamping, even with a modified surgical approach [2]. In recent years, with the continuous development of endovascular treatment techniques, the invention of various new stents and balloons, and the innovation of different surgical procedures, the efficacy of apical basilar aneurysms has improved significantly, even for the relatively tricky wide-necked aneurysms. Treatment of apical basilar artery aneurysms by endovascular interventional procedures has proven safe and effective [3].
Many surgeons, especially community physicians, often lack sufficient experience in treating this type of aneurysm, which is challenging to operate, and we show here a typical case of apical aneurysm of the basilar artery with the associated vascular structures labeled in a schematic form. In this form, we hope to deepen the understanding of community medical personnel about the class of diseases to enhance community intervention, strengthen the health of the community, families, and individuals, and reduce the incidence of disability and institutionalized care.
BA, basilar artery; CTA, computed tomography angiography; IA, intracranial aneurysm; PCA, posterior cerebral artery; SCA, superior cerebellar artery.
Not applicable
Not applicable
Not applicable
The authors declare that they have no competing interests.
This work was supported by the Medical and Health Science and Technology Innovation Project of the Suzhou Health Commission [grant number: SKY2022002], and the Special Funds for Science and Technology Programs of Jiangsu Provincial Department of Science and Technology [grant number: BE2023712].
JD-Zhu and X-Jin provided care for the patient. JD-Zhu and X-Jin wrote the initial draft of the manuscript. J-Wu collected the data and prepared the images. ZQ-Yu and J-Wu designed the paper, and revised the final manuscript. All authors reviewed and approved the final version of the manuscript. Written consent for publication was obtained from the patient.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
