
Research Article | DOI: https://doi.org/10.31579/2578-8868/272
1 Additional Professor, Department of Physiology, AIIMS Raipur, Chhattisgarh, India, 492099.
2 Professor, Department of Physiology,Pt. J N M Medical College, Raipur, Chhattisgarh, India, 492001.
3 Professor, Department of Physiology, AIIMS Raipur,Chhattisgarh, India, 492099.
4 Additional Professor, Department of Medicine, AIIMS Raipur, Chhattisgarh, India, 492099.
5 Professor, Department of Biochemistry, AIIMS Raipur, Chhattisgarh, India, 492099.
*Corresponding Author: E Khandelwal, Additional Professor Room No 3116, 3rd Floor, Medical college building, Department of Physiology, AIIMS Raipur, 492099 Chhattisgarh, India.
Citation: E Khandelwal, S Tripathi, A Ingle, P Wasnik, R Nanda (2023), Endothelial Dysfunction in Adult Patients of Sickle Cell Disease, J. Neuroscience and Neurological Surgery. 13(3); DOI:10.31579/2578-8868/272
Copyright: © 2023, E Khandelwal. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 19 June 2023 | Accepted: 17 July 2023 | Published: 28 July 2023
Keywords: sickle cell disease ; red blood cells
Sickle cell disease is one of the most common hemoglobinopathy worldwide. It is an autosomal recessive genetic disorder caused by replacement of adenine to thymine nucleotide in the beta chain of hemoglobin results in replacement of valine for glutamic acid at 6th position. This substitution results in formation of sickle hemoglobin (HbS) which in turn leads to a reduced lifespan of red blood cells (RBC). In hypoxic conditions, HbS has a tendency to aggregate and form fibrillar structure called tactoid within the red cells
Sickle cell disease is one of the most common hemoglobinopathy worldwide. It is an autosomal recessive genetic disorder caused by replacement of adenine to thymine nucleotide in the beta chain of hemoglobin results in replacement of valine for glutamic acid at 6th position. This substitution results in formation of sickle hemoglobin (HbS) which in turn leads to a reduced lifespan of red blood cells (RBC). In hypoxic conditions, HbS has a tendency to aggregate and form fibrillar structure called tactoid within the red cells [1]. RBC’s gets distorted and attains crescent moon shape, leading to increase in hemolysis and vaso-occlusive crises (VOC). VOC is characterized by episodes of acute painful crisis and multi-organ dysfunctions [2,3,4] in SCD. There are many factors triggering VOC like: increase viscosity of blood, dehydration of sickled red cells, anchoring of sickled red cells to vascular endothelium and other vascular inflammatory changes [5]. Though the pathophysiology6,7of VOC is centered on deoxy sickle hemoglobin, however the role of endothelial dysfunction (ED) is also very crucial but is often neglected in evaluation of SCD severity. Endothelial dysfunction leads to impaired synthesis of nitric oxide (NO) effecting the vascular vasodilatation which impairs the local blood flow [8] and reduce local tissue perfusion. It also affects the circulation time of sickled red cells in the body and increases the risk of VOC [9]. ED is one the major cause of morbidity & mortality in SCD patients Estimation of endothelial functions and its correlation with vascular biomarkers [10] can be helpful in early risk detection of vaso-occlusive crises in these patients and can potentially streamline the management the VOC and improve their quality of life[11,12]. SCD is an important public health problem which affects millions of people globally causing high treatment burden on health care system. It is very common in the Indian subcontinent[13,14]. Chattisgarh State which lies in the sickling belt of, India has a high prevalence of the disease [15]. Very few studies have been undertaken to understand the correlation of endothelial dysfunction and vaso-occlusive crises in the affected population. The purpose of the present study was to evaluate the ED using reactive hyperemia by photoplethysmography (PPG) to detect impending risk of VOC in SCD and to reduce the complications associated with it.
Aim and Objective: Aim of the present study was to estimate endothelial dysfunction by reactive hyperemia in SCD patients with risk of impending VOC. To study correlation of blood biochemical markers like Nitric Oxide (NO), Endothelin 1 (Et) and Vascular endothelial growth factor (VEGF) with the PTT recovery parameters of reactive hyperemia in SCD patients and controls.
Methodology: This was a cross sectional study with total sample size (n) 60. After obtaining Institutional ethical clearance (no:AIIMSRPR/IEC/2018/128) and informed written consent participants divided into two groups. Group 1 comprising of 30 Young Adult SCD diagnosed patients of age group 18 to 40 year recruited from sickle cell OPD of AIIMS Raipur, India. Group 2 as control group comprising of 30 of healthy age-matched subjects recruited from general population. Patients having history of VOC in past six months, smoking, alcohol intake, diabetes mellitus, essential hypertension, vascular disorder, psychiatric problems and seizures were excluded.
Each patient and control were explained in detail about the procedure of assessing endothelial function by PPG during reactive hyperemia. They were asked to abstain from any stimulant like cigarette, alcohol, tea, caffeine intake for 12 hours before test. After patient recruitment recordings were conducted at Autonomic & Vascular testing clinic at AIIMS Raipur. The room temperature was maintained between 25° - 27°C in noise free condition. All the test recordings of patients and controls were performed around 10:00 am.
Each patient and controls electrocardiogram (ECG) was monitored using a lead II for 5 minutes to estimate Heart rate variability (HRV). After 5 mins of supine rest PPG [16] signals were recorded utilizing either right middle or index finger as a baseline measurement. This was followed by induction of reactive hyperemia (RH). It is a standard procedure used for assessment endothelial function. The blood pressure cuff was tied on right forearm 6 cm above the cubital fossa. After baseline recording of PPG and ECG for 5 mins, pressure in the BP cuff was raised to supra systolic (220mm Hg) to induce ischemia and the pressure was maintained for 5 minutes (or till patients tolerate). Recovery recording of PPG parameters and ECG was done for further 5 minutes after pressure was released and completing reactive hyperemia protocol [17] shown in Figure 1. Parameters acquired are Amplitude of wave-form, Peak to Peak interval (PPI), Pulse Transit Time (PTT), Crest time (CT), Slope of wave-form. HRV and PPG were recorded on 8-channel digital physiograph (LabChart, AD Instruments, Bella Vista, Australia).
Bio chemical markers: 6 ml of blood sample was collected from patients and controls for assessment of Nitric Oxide, Vascular endothelial growth factor and Endothelin-1 by Sandwich ELISA technique at department of biochemistry, AIIMS Raipur. Other routine blood investigation was carried for all patients and controls.
Data Analysis: Baseline ECG and PPG were recorded for 5 minutes to obtain control data. PPG pulse parameters viz: amplitude; height of the systolic peak point from the foot; slope, maximum of the first derivative of upstroke; systolic peak to peak interval, the time difference between the successive systolic peak were obtained by beat-to-beat changes PPG and ECG. Additionally, the beat-to-beat changes of Pulse Transit Time was computed as the time delay between R wave peak of ECG and onset of corresponding PPG pulse [18].
Data obtained were initially checked for distribution. Parametric test was applied for Gaussian distribution and appropriate non parametric test was applied for non-Gaussian distribution.
The following tests were used as appropriate for the data: Paired ‘t’ test, Mann Whitney test, Friedman and Wilcoxon signed ranks test, Spearman's correlation. Level of significant was set to p<0>
Total 42 SCD patients were recruited from sickle cell OPD out of which 30 patients (mean age 24.53 ± 4.96 years) fulfilled the inclusion and exclusion criteria and 30 healthy controls (mean age 30 ± 3.8 years) were recruited from general population. Demographic profile and baseline physiological parameters are presented in Table 1. SCD patients had significantly lower height and body weight than controls. Patients had significantly higher resting heart rate but comparable blood pressure. HRV, the basal cardiac autonomic tone parameters were compared between SCD patients and Controls and shown in Table 2. HRV parameters for parasympathetic and sympathetic responses showed that SCD patients had significant lower cardiac autonomic tone as compared to controls. Time domain parameters of HRV were significantly lower in the SCD patients as compared to control subjects. Total power is also significantly reduced in patient group. Table 3 lists the baseline PPG parameters of the SCD patients and Controls, All the PPG parameters were significantly higher in controls than patients except slope. Table 4 compares the recovery response of reactive hyperemia for the PPG parameters in SCD Patients and controls. PTT recovery parameters were significantly different in patients than controls after reactive hyperaemia. Table 5 showed baseline biochemical markers of Endothelial Functions. All the markers NO, Et1 and VEGF were significantly higher in patients than controls. Correlation of biomarkers and PTT was analyzed in SCD patients and controls. We found that all the biomarkers of endothelium functions are negatively correlated with Pulse Transit Time in SCD patients. NO is significantly negatively correlated with PTT in Patients (r=-.378*, p=.039*). Correlation analysis of biomarkers and PTT in controls showed that all the biomarkers of endothelium functions are positively correlated with PTT. VEGF (r=.462, p=.04) & NO (r=.485, p= .03) is significantly positively correlated with PTT in Controls.

Values shown are mean ±S.D., p value* ≤ 0.05 (significant).
Table 1: Demographic Profile and Baseline physiological parameters

Values are shown in Median (1 quartile – 3 quartile), p value* ≤ 0.05 (significant).
SDNN- standard deviation of the R-R intervals; RMSSD- root mean square of successive RR Intervals; NN50- number of RR intervals equal to or greater than 50 milliseconds; pNN50- percentage of NN50; SDSD-Standard deviation of differences between adjacent RR intervals. ab- absolute unit for total power of entire frequency spectrum of heart rate variability.
Table 2: Comparison of HRV parameters in patients and controls

The values are presented as Median (1st quartile- 3rd quartile), p value* ≤ 0.05 (significant).
Table 3: Baseline Photoplethysmography (PPG) parameters in patients and controls
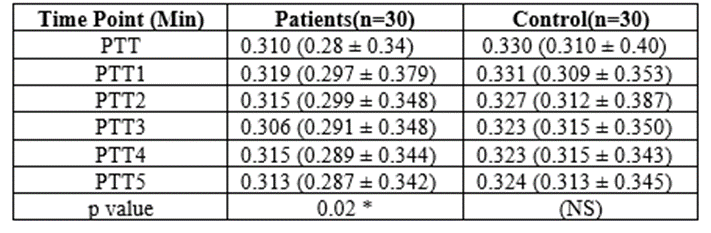
Values shown are mean ±S.D., a = p values are significant (p<0>
Table 4: comparison of recovery response of reactive hyperemia for the Pulse Transit Time (PTT) in SCD Patients and controls.

The values are presented as Median (1st quartile- 3rd quartile), p value* ≤ 0.05 (significant).
Table 5: Baseline Biochemical Markers of Endothelial Functions
The baseline heart rate was significant higher in-patient group as compared to controls suggestive of increased sympathetic neural drive to heart. Blood pressure is comparable in both the groups. Other demographic parameters like height and weight were significantly decreased in patients as compared to the control suggestive of compromised growth in sickle cell patients [19].
HRV findings in table 2 showed that the parasympathetic time domain parameters were significantly lower (RMSSD, NN50, pnn50, SDSD) in the patient group. Lower resting parasympathetic tone has been postulated to be an important feature in the pathophysiology of cardiac autonomic dysfunction and also it has been suggested that the decrease in absolute power of the LF component is associated with sympathetic activation which may explain the increased resting heart rate in patients [20]. Baseline PPG parameters are significantly decreased in SCD patients than controls suggestive of compromised neurovascular tone. To compare the
endothelial functions in both the groups the change of PPG recovery response of vasodilation during RH has been attempted in the present study. PTT was significantly lower patients as compared to controls indicates some kind of increased tone/ Stiffer blood vessels.
During reactive hyperemia, vasodilation and decrease in vascular resistance happens due to accumulation of local metabolites and Endothelial NO. This was depicted by the significant increase in the amplitude in the control group, then in the patient group. PTT is inversely proportional vasomotor tone, longer PTT in controls as compared to patients immediately after the release of occlusion strongly suggest intact endothelial function in controls due to release of Endothelial NO. Our study findings are similar to Maltz and Budinger [21], Itzhaki et al [22] suggested that peripheral arterial tone assessed by PTT can be used as a noninvasive method of assessing endothelial function in health and disease. In patients ET 1 is raised due to vascular dysfunction by sickle cells. This increased level leads to vasoconstriction everywhere in circulation and also has effect on sympathetic nervous system. Correlation analysis showed that patients are negatively correlated with biomarkers specifically NO. This raised ET1 may lead to increase in NO as compensatory mechanism of vasoconstriction [9]. VEGF is one of the biomarkers depicting vascular injury and hypoxia was significantly raised in patient group. VEGF express vascular adhesion molecules and hence facilitates adhesion of sickled red cells. It also helps in vascular remodeling and growth of collateral vessels [9]. Interesting result of our study was the reduced vascular response to RH in patients of SCD has been objectively assed by PPG responses. This preliminary study suggests that together parameters of PPG and HRV can be used to quantify endothelial function objectively to detect the deficits of vascular response in SCD. This study helps us to gain useful research insight in field of pathophysiology of SCD for medical field and its applications which is lacking in our current scenario and can be extended in future in larger scale.
Acknowledgements: Department of Sickle Cell Clinic, AIIMS for referring patients.
Sources of funding: AIIMS Raipur
Conflicts of interest: The authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
