
case report | DOI: https://doi.org/10.31579/2690-1897/208
1Department of Neurosurgery, Debre Behan University, Debre Berhan, Ethiopia
2Department of Neurosurgery, Fujita Health University, Bantane Hospital, Nagoya, Japan
*Corresponding Author: Mikael Aseged, Assistant professor of Neurosurgery, cerebrovascular fellow at Fujita Health University Present address- Debre Berhan University, Ethiopia.
Citation: Mikael Aseged, Fuminari Komatsu, Yoko Kato, (2024), Endoscopic Evacuation of Post Burr Hole Subdural Empyema Caused by Propionibacterium Acne, Case Report. J, Surgical Case Reports and Images 7(7); DOI: 10.31579/2690-1897/208
Copyright: © 2024, Mikael Aseged. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 August 2024 | Accepted: 12 August 2024 | Published: 19 August 2024
Keywords: subdural empyema; endoscopic assisted; p.acnes; post burr hole; chronic subdural hematoma
Introduction: Post burr hole subdural empyema caused by Propionibacterium acnes is very uncommon and drainage with endoscopy is effective and efficient. Less complication than craniotomy/craniectomy and better evacuation the burr hole alone.
case presentation: we presented a 71-year-old male patient who presented to our hospital after he had undergone 2 times burr hole in same site for CSDH in another hospital,with headache. MRI showed restriction on diffuse weighted image and CRP of 19mg/dl. We evacuated the empyema with endoscopy with culture result of P.acnes. He was put on IV antibiotics and had significant improvement.
Conclusion: Endoscopy assisted burr hole evacuation of subdural empyema is a great option to manage this devastating subdural space collection.
CRP- C-reactive protein
CSDH - Chronic subdural hematoma
CT – computerized tomography
DWI-ADC- Diffusion weighted image-apparent diffusion coefficient
MRI- Magnetic resonant imaging
SDE- Subdural Empyema
Subdural empyema (SDE), a purulent loculated collection under the dura mater, is a rare condition with the estimated incidence of 0.1 per 100,000 persons. [1]. Because the subdural space lacks any anatomical barrier that could prevent the pus from spreading across the brain hemisphere, it has a rapid course and usually a poor prognosis if not diagnosed and managed early. [2]. It is usually treated with burr hole drainage or craniotomy. With the wide acceptance of neuroendoscopic surgery, it can be used to drain subdural empyema which will help to see the blind spot that cannot be addressed with burr hole and minimize morbidities associated with Craniotomy. Here we present a case of SDE post burr hole for Chronic subdural hematoma (CSDH) caused by Propionibacterium acne (P.acnes) which is an anaerobic, lipophilic, gram-positive bacteria managed with endoscopic subdural empyema drainage and irrigation then he received intravenous antibiotics based on culture and drug susceptibility. He had improvement.
A 71-year-old man presented with a headache and a CT scan examination revealed a right side hemispheric chronic subdural hematoma. He underwent burr-hole surgery, hematoma was evacuated and was discharged with improvement. However, a month later, he experienced retro-orbital pain and headaches, followed by weakness in the left upper and lower extremities. The patient was taken to Operation theatre and through previous burr-hole irrigation was done and had improvement. But 1 months after the second surgery the patient complain headache and investigated with MRI and CT as shown below in Fig 1. An MRI examination revealed extra axial fluid collection at previous burr hole side with heterogeneous intensity on T1 and hyper-intensity on T2, with central foci of hypo-intensity and restricted diffusion on DWI-ADC mapping as shown in Fig 1. The CRP was determined and found out to be 19mg/dl. Using previous burr hole defects endoscopy was advanced to the subdural space since it would be difficult to evacuate the empyema with burr hole alone. The intraoperative findings were a thick abscess in the subdural space with septation and thin abscess filling the bone defect, with endoscopic-assisted abscess drainage and irrigation it was possible to remove the thick abscess from deep pockets, as shown in fig 2 which was sent for microbiological culture study, identifying Propionibacterium acnes as the causative organism. Subdural drain was left, and he was put on IV antibiotics subsequently discharged with significant improvement.
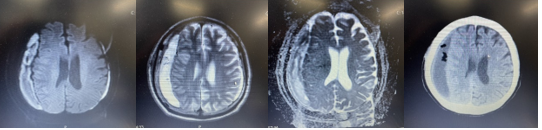
Figure 1: a shows T2 hyper intensity with foci of hypo intensity 1.b and 1.c shows DWI-ADC mapping with restriction and 1.d shows CT of Subdural empyema with central hypo density

Figure 2: shows epidural collection at previous burr hole site, and shows endoscopic view of thick abscess with septation
Discussion
Subdural empyema (SDE) following chronic subdural hematoma (CSDH) surgery is an uncommon but serious complication. Even though it is a rare pyogenic infection it is fatal complication of surgical procedures.[3] Post operative subdural empyema following burr hole drainage is not commonly reported case. Usually, the implicated organisms are normal skin floral like Streptococci sp., S.aureus, S.epidermidis but the ubiquitous member of skin flora P.acnes is a rare cause of intracranial infections.[4] SDE has nonspecific clinical features, including headache and vomiting which makes it difficult for early diagnosis. Additionally, it is also difficult to differentiate between recurrent CSDH and SDE without special imaging evaluation such as magnetic resonance imaging (MRI) which might suggest more about the content of the subdural collection.[2] P.acnes is an unusual, rare cause of intracranial infection. Although recently some publication reports the increased incidence of P.acnes in intracranial pyogenic collections. The incriminated risk factor is brain surgical implant with mild clinical course.[5] Cultures positive for P. acnes may sometimes represent a false-positive result due to contamination which makes the diagnosis of a true infection often challenging. Moreover, these organisms may be difficult to identify initially because of their slow growth. When cultured, they often need more than three days to grow.[6]In our case apart from the MRI result of restricted diffusion the C-reactive Protein (CRP) value was 19mg/dl which suggest inflammatory and infectious process. Surgical management is necessary for subdural empyema but there are still controversies and depends on surgeons' preference, patient condition and imaging parameters to decide on the mode of management either to use burr hole or craniotomy. Each of them has their own Prons and cons.[7] Burr hole drainage requires local anaesthesia, but it poses some difficulties to access and drain septated and thick empyema while craniotomy/craniectomy needs general anaesthesia it gives best view to address thick and septated abscess with the drawback and complication of general anaesthesia and bone flap infection. Endoscopic surgery combines the benefits of both burr hole and Craniotomy with the mare complication of local anaesthesia and requirement of expertise. It gives best view of septated and loculated abscess drainage with burr hole. Jonathan Yun et al also describe superiority of Endoscopic assisted burr hole evacuation of empyema to burr hole drainage alone with regard to recurrence rate.[8] In our case the use of endoscopy was not only to visualise, but also surgical removal of abscess pockets and cavity was done with endoscopy which has shifted the mode of approach from craniotomy to burr hole since with thick abscess it would have been difficult to see and manipulate with burr hole alone.
Endoscopic assisted burr hole drainage of SDE is effective and can be used to drain even loculated abscesses with local anaesthesia. It will prevent the complications associated with craniotomy/craniectomy like general anaesthesia, bone flap infection and second surgery to replace bone as well as with burr hole alone which is mainly recurrence due to inadequate drainage.
Ethical Declaration- N/A
Patient consent- patient consent was obtained
Author Contribution
MA conceptualization, writing, editing
Y.K- editing
F.K- editing
No funding was available
Nothing to declare
I would like to thank all the neurosurgical stuff and patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
