
Research Article | DOI: https://doi.org/10.31579/2690-1919/209
* Department of Neurology and Neurosurgery Institute, Havana, Cuba.
*Corresponding Author: Orestes López Piloto, Department of Neurology and Neurosurgery Institute, Havana, Cuba.
Citation: Orestes L. Piloto, Tania C. Hernández, Pedro D. Jiménez, Norbery R. de la Paz, Duniel A. Casa, et al. (2021). Endonasal Endoscopic and Transoral Approaches to the Craniovertebral Junction and the Clival Region. J Clinical Research and Reports, 9(4); DOI:10.31579/2690-1919/209
Copyright: © 2021, Orestes López Piloto. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 October 2021 | Accepted: 22 November 2021 | Published: 04 December 2021
Keywords: transoral approach; craniospinal junction; endoscopic endonasal approach; hemoneumothorax; craniovertebral junction; clival region
Introduction: The transoral approach was first described by Kanavel in 1917 to treat injuries of the craniospinal junction. In 2002, Frempong-Boaudu reported 7 adults who underwent endoscopically assisted transoral surgery, this was the first report that endoscope was used in an assisted manner for transoral surgery. In 2005, Kassam published the first report of an EEA being used to perform an odontoidectomy.
Method: A descriptive, retrospective and linear study was carried out in 16 patients who underwent surgery using the microsurgical and endoscopic transoral and Extended Endoscopic Endonasal approach in the period from January 2004 to May 2021.
Results: The average age of the patients was 45 years and there was a predominance of the male sex (10) with the female one (6). The tumoral pathology (9), 6 cases with histological diagnosis of clivus cordroma and 1 patient with chondrosarcoma, two cases with Meningioma and cholesterol granuloma of clival localization, achieving gross total resection in 2 of them and in the rest subtotal resection, all improved neurological symptoms. Complications, partial dehiscence of the velopalatine surgical wound 1 case, 1 lesion of the left vertebral artery and 1 case decompensated Diabetes Mellitus and hemoneumothorax during stay in the ICU, which death 7 days after surgery and 1 CSF fistula.
Conclusions: Both, the transoral and endonasal endoscopic approaches have their precise indications in each particular case, having their indications well defined. To achieve this, we must have neuroimaging studies and be able to correctly define the selection of the surgical approach.
The transoral approach was first described by Kanavel in 1917 to treat injuries of the craniospinal junction, later in 1957 Southwick and Robinson describe the case of a giant osteoma removed through a transoral route. Fang and Ong in 1962 established the transoral route as a surgical technique by publishing its use in 6 cases with injuries to the upper cervical vertebrae; in their casuistry, three of the cases were traumatic, due to dislocation or fracture dislocation in the Atlanto-axial joint, in two cases it was due to recurrent dislocations of unknown causes and one case of tuberculous infection in the two upper vertebrae, of these one died of Sepsis and the others evolved satisfactorily [1]. Following these events, criticism of transoral surgery continued because of limited exposure, poor lighting, and inadequate instrumentation.
With the advent of the surgical microscope, microsurgical instruments, and especially the creation of the transoral retractor system, it favored the reuse of the transoral approach [2-8]. The use of endoscopy has taken a leap forward in dealing with lesions in the lower region of the clivus and the odontoid process, all with the aim of increasing exposure and better visualization of the structures [9-11].
Each approach has its advantages and disadvantages, it also has limitations in its exposure, surgeons must be familiar with various antero-medial approaches and their modifications, to select the best approach in each case [11-16].
The location and extent of the injury are determining factors in selecting an appropriate skull base approach. The transoral approach offers direct access to medial injuries of the craniovertebral junction with extradural location, such as chordomas, chondrosarcoma, giant cell tumor, rheumatoid or degenerative pannus [14,16-18]. The report of 14 transoral cases by Crockard and colleagues in 1985 and 53 transoral cases by Hadley, Sonntag, and Spetzler in 1989 helped solidify the approach. The standard transoral approach as popularized by the pioneers mentioned above include the transoral-transpharyngeal approach and the transoral transpalatopharyngeal approach [19].
In 2002, Frempong-Boaudu et al reported on 7 adults who underwent endoscopically assisted transoral surgery, this was the first report in which the endoscope was used in an assisted manner for transoral surgery. In 2005, Kassam et al [9], published the first report of an EEA being used to perform an odontoidectomy [19].
In our study, we highlight the evolution from the standard transoral approach, going through the endoscopic transoral approach until reaching the extended endoscopic endonasal approach, to address lesions located in the ventral region of the great hole and the cranio-spinal junction, as treatment alternatives for approaches to the base of the skull. Currently, there is a great development of endoscopic approaches and the learning of which must be linked to every neurosurgeon as one more tool within their therapeutic arsenal, but the necessary means to carry them out are not always available and we can resort to classic techniques that today are in disuse.
A descriptive, retrospective and linear study was carried out in 16 patients who underwent surgery using the microsurgical and endoscopic transoral and Extended Endoscopic Endonasal approach in the Clinical-Surgical Hospitals "Lucía Iñiguez Landín" in Holguín. ¨Lenin Fonseca¨ School Hospital in Nicaragua and Institute of Neurology and Neurosurgery in Havana, in the period from January 2004 to May 2021. All patients who underwent surgery gave their informed consent in writing according to the rules of Good Medical Practice (BPM).
Diagnosis
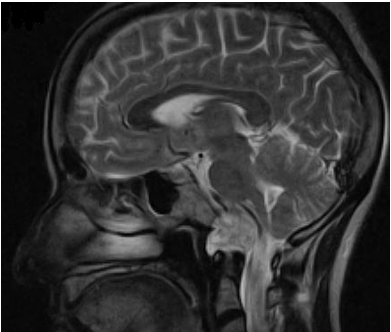
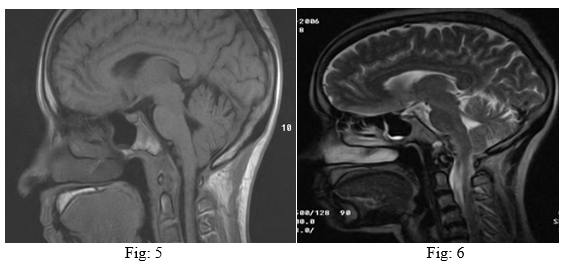
The patients attended during this period presented degenerative or tumor lesions of the craniospinal region, all patients underwent a transoral approach, both standard and endoscopic, as well as endoscopic endonasal approach extended to the clivus or odontoid process. Prior to surgery, a neuroimaging study, a simple radiograph of the cranial spinal junction in dynamic views, computed tomography (CT), and magnetic resonance imaging (MRI) were performed (Phillip 0.23T and 3T equipment). The medication for patients with Rheumatoid Arthritis (RA), was not interrupted unless they were complying with the Metrotexate regimen, in these cases it was suspended 15 days before surgery and started again 15 days after the procedure.
Standard Transoral Approach
Anesthesia and position
Intubation of the patient by the orotracheal route, after topical anesthesia in the oropharynx and nasopharynx, laryngeopharyngeal packing with aseptic material. Prior to this procedure, continuous lumbar spinal drainage is performed in the patient, which makes it easier for us to work in the area with the least risk of cerebrospinal fluid fistula by reducing the dura mater tension. Supine position, semi-seated on an acrylic-based surgical table to facilitate the entry of Rx, the head is held in the Mayfield head, the latter allows us to perform the necessary deflections of the spine at the high cervical level if necessary.
Approach
Antisepsis of the area with 10% povidone iodine, then with Hydrogen peroxide and ending with 0.9% saline irrigation, placement of Dickman autoretractor, antisepsis of the area is completed, the endotracheal tube is protected with the lateral autoretractor, the oral retractor allows depression of the tongue and lateral retraction increases the field of work, 0.5% lidocaine is infiltrated with an epinephrine solution 1: 200,000, sometimes this step is not necessary, in many In cases, the pharyngeal wall is opened with monopolar cautery. A midline is located palpating the C1 tubercle, this anatomical point may be absent or distorted in those patients who present a tumor in this location, a midline incision is made of the pharyngeal mucosa that extends from the hard palate to the base of the uvula, deviating laterally, retraction of the edges of the mucosa, fixing to the autoretractor, a surgical microscope is placed, then a midline incision of the posterior pharyngeal raphe is made, extending from the clivus to interspace C2-C3, the wall The posterior pharynx is retracted laterally by means of a Dickman fixation suture, dissection of the prevertebral fascia and of the long neck muscles, which are released from the bony ligaments, thus exposing the caudal end of the clivus, the arch. anterior of the atlas and anterior surface of the axis, before exposing these bony structures the anterior common longitudinal ligament and the occipital ligament are di Dried, with this exposure a width of 3 to 3.5 cm is achieved, it is not advisable to try to seek a more lateral exposure, in this effort there is a risk of destruction of the Eustachian tube orifices, injury to the vertebral artery and hypoglossal nerve. Subsequently, the 3 cm of the anterior arch of the atlas is removed with a high-speed drill, resection of the caudal portion of the clivus depending on the pathology treated, the soft tissue located anterior to the odontoid is released with a gouge, resection of the process odontoid in the face-flow direction with a high-speed drill and a diamond tip, using microsurgical dissection, the ligaments of the neighborhood are separated, if it presents chronic instability, do not forget to carefully resect the pannus, with cauterization, incomplete resections should be avoided of the odontoid because it can injure the dura and cause a cerebrospinal fluid (CSF) fistula, for its complete resection the angled Lee-Smith Kerrison (1 mm) and angled curette should be used to facilitate removal, resect the pannus behind the odontoid should be done carefully and with angled curette rings.
Subsequently, incision of the tectorial membrane that allows dural decompression, an Angled Hook Dissector is placed between the tectorial membrane and the dura to prevent dural tear. When performing this surgical step, care must be taken in handling, which is gentle so as not to provoke changes in the latency of the brain stem or compression of the same that may cause any previously non-existent sequel.
If there is a need to explore intradurally, a cruciform opening is made, immediately behind the clivus, in the infero rostral direction, after cauterization of the circular sinus at the level of the hole, work in this area is facilitated by spinal drainage, due to the lower turgor dural, the dural opening allows us to expose: lower portion of the bridge, medulla and cervicomedullary junction. At the end of the operation, dural coping with Dacron or 4-0 polyester is performed and later it is reinforced with muscular fascia and the area is protected with Gelfoam.
Before the closure of the mucosa, a sample is taken for culture, an antibiotic is instilled in the area, approximation of the long neck muscles, posterior pharyngeal musculature and the posterior pharyngeal mucosa with absorbable suture 3-0, the closure of the soft palate is performed together with the nasal mucosa to loose points using Vicryl 3-0.
In patients with clivus lesions or a diagnosis of platybasia, it is necessary to expose the hard palate by performing a resection.
Endoscopic Endonasal approach
During de procedure we using a two-surgeon, four-handed technique. General anesthesia with orotracheal intubation. The patients were positioned supine on operating table with the head in slight flexion, tilted slightly toward the surgeon, with using a fixation system (Mayfiell-Kees head holder). For all procedures, 0° and 30° wide-angle endoscopes were used (Karl Storz, Tuttlingen, Germany) with a neuronavigation system (Brain Lab) for confirming anatomical areas during all stages of the procedure and neurophysiological monitoring of motor and somatosensory evoked potentials. A portion of the upper leg was prepared for possible fat or fascia lata graft. The nasoseptal flap was elevated, and following the bilateral out fracture of the inferior turbinates, endonasal access to the nasopharynx was ensured via both nares. The inferior nasal meatus was used as a guide to directly access the nasopharynx overlying CVJ. The eustachian tubes lie approximately at the level of the occiput–C1 junction, acting as an important landmark for the lateral limit of exposure. We palpated the anterior tubercle of C1 and confirmed this with neuronavigation. A midline vertical linear incision was made using monopolar cautery. We dissected myomucosal layer subperiosteally and exposed the C1 anterior arch, dens, and lower clivus. A high-speed drill was used to remove C1 and odontoid, leaving the posterior cortical shell and ligamentous attachments in place. A Kerrison rongeur or micro dissector was then used to remove the cortical shell and ligaments. The dura was visualized to confirm sufficient decompression [20].


The average age of the patients was 45 years and there was a predominance of the male sex (10) with the female one (6).
The tumoral pathology (9) of clival localization was the most frequently found, 6 cases with histological diagnosis of clivus cordroma and 1 patient with diagnosis of chondrosarcoma, the remaining two with diagnosis of Meningioma and cholesterol granuloma of clival localization, all were performed a Standard Transoral Approach (transpalatopharyngeal or transpharyngeal), transodontoid, endoscopic transoral or Extended Endoscopic Endonasal Approach to the Clivus or odontoid, achieving gross total resection in 2 of them and in the rest subtotal resection, all improved neurological symptoms. Radiotherapy was indicated in cases with subtotal resection after surgery.
| No | Age/ Sex | Histological | Approach | Resecction Grade | Follow up (moths) | Recurrent | Treatment post-recurrent | Complications
| Inestability Signs
| Results |
| 1 | 57/m | Clival Chordoma tip | TPPh | Subtotal | 35 | 1 | RT | no | Improved, died 6 years after surgery | |
| 2 | 61/m | Clival Chordoma Midle 1/3 | TPh | Subotal | 62 | - | - | no | Improved, Died 62 months after surgery | |
| 3 | 52/f | Clival Meningioma
| TPPh | Subtotal | 47 | 1 | RT | Left vertebral injury. | no | Improved |
| 4 | 47/f | Clival Chondrosarcoma
| TPPh | Subtotal | 10 | fallecido | RT | no | Improved, Deceased at 10 months | |
| 5 | 32/m | Cholesterol Granuloma
| TPPh | Total | 5years | - | - | no | Cured | |
| 6 | 54/f | Rheumatoid Pannus
| TPh TOd | Total | 5years | - | - | no | Cured | |
| 7 | 66/m | Rheumatoid Pannus
| TPh TOd | Total | 5years | - | - | CSF fistula | no | Cured |
| 8 | 70/m | odontoid Os (postrauma) | TOd | Total | 12 | - | - | Partial dehiscence of velopalatine wound | yes | Cured |
| 9 | 61/m | Rheumatoid Pannus
| TPh TOd | Total | 12 | - | - | no | Improved. | |
| 10 | 29/m | odontoid Os | TPh TOd | Total | 4 years | Cured | ||||
| 11 | 45/f | Basilar Impresion
| TPh TOd | Total | 36 | Improved. | ||||
| 12 | 59/m | Clival Chordoma
| EEE | Subtotal | 9 | Decompensated Diabetes, Left Unilateral Pneumothorax. | no | Died 7 days after surgery | ||
| 13 | 63/f | Clival Chordoma Inf 1/3 | EEE | Subtotal | 10 | yes | Improved, Died a 1 year after surgery. | |||
| 14 | 29/m | Cervical Chordoma
| TOE | Total | 36 | no | Cured | |||
| 15 | 12/f | Clival Chordroma tip
| EEE | Subtotal | 24 | no | Improved. | |||
| 16 | 14/m | Basilar Impresion
| EEE | Subtotal | 36 | no | Cured |
TPPh: Transoral-Transpalatopharyngeal, TPh: Transoral-transpharyngeal, TOd: Transodontoid, TOE: Transoral Endoscopy, EEE: Endosopic Endonasal Extend, RT: Radiotherapy
Table 1: Behavior of operated patients by transoral and endonasal approach
The remaining 3 cases presented rheumatoid arthritis, with manifestations of compression of the brain stem, due to the presence of Pannus, it was decided to perform a standard transoral approach and resection of the same, presenting immediate improvement of the symptoms, 2 patients had chronic dislocation of the axis tooth (Os Odontoideo), due to an old type II fracture of Anderson and Alonso, which was initially treated with conservative treatment (Halo-vest for 3 months), 23 years after the fracture, one begins with gait disorders and myelopathic signs, confirming in neuroimaging studies, neural compression due to displacement of the axis tooth and the other, a fracture that went unnoticed, up to 5 years after a trauma that began with myelopathic signs, and in neuroimaging studies, bone abnormality was found.
In all the cases operated on by norm in the postoperative period, the Cervical Collar was placed, which was maintained for three months, only two presented signs of instability in one patient, without showing signs of neurological compression, and decided to perform fixation 6 months after surgery. occipito-cervical and the other case, despite remaining simple with the external orthosis, presented manifestations of medullary compression and due to general condition, it was not possible to perform the intervention and died.
The report found a patient with partial dehiscence of the upper end of the velopalatine suture, healing in two months, without the need for a new surgical intervention.
In the operated cases, there was no need to perform a preoperative tracheostomy, although 4 of our patients had low cranial nerve intakes (Cholesteatoma, Chondrosarcoma, Basilar impression and 1/3 inferior chordoma), we related this advantage to the modified Dickman separator, it provides an excellent surgical field and the flexible and ringed endotracheal tube, which prevents narrowing of the lumen. In the postoperative period, we maintained intubation for 24 hours, feeding was performed with a liquid diet for 7 days by Levine catheter and then for 3 weeks a soft diet, as well as treatment with a broad-spectrum prophylactic antibiotic in the immediate postoperative period, in these 16 operated patients did not present septic complications, only 1 case with partial dehiscence of the velopalatine surgical wound, 1 partial lesion of the left vertebral artery that was solved in the postoperative period, and one case with decompensated Diabetes Mellitus and hemoneumothorax during stay in the ICU, which led to death at 7 days after surgery and 1 CSF fistula for which continuous spinal drainage treatment was applied for 7 days, resolving that symptoms.



The Transoral Approach, is a procedure with which you can directly decompress damaged neurovascular structures, causing less instability, although sometimes you have to perform an internal fixation in a second surgical time [25,26]. There are cases where the extension of the tumor tends to destabilize the Atlanto-occipital or atlantoaxial joint, requiring stabilization, sometimes instability is not present at the time of diagnosis, however, after tumor resection, stabilization may be required to avoid postoperative iatrogenic instability [22-27].
Clivus chordomas are lesions that derive from remnants of the notochord, within the most frequent locations of this type of neoplasm, the clival is between 30 and 40% in relation to the other locations, these lesions are preferably observed in this region and in the sacrococigee, being more frequent in men than in women between 20 and 40 years [28].
Platybasia and Basilar Impression are different entities, but they are almost always presented together, just like brain stem kinking. However, Platybasia can present in isolation, on the other hand, Basilar Impression can be observed without Platybasia, the latter isolated is not accompanied by symptoms and when observed, there is always Basilar Impression or other associated malformations, Basilar Impression was described by First time by Ackermann in 1790, it is the most frequent cervicoccipital malformation, the one most often associated with neurological insufficiencies of the cervicobulbar region [29].
Os odontoideo is a rare entity, its prevalence and incidence is not well elucidated. In 1863 it was described for the first time postmortem in the separation of the odontoid process from the axis body. In 1886 Giacomini confers the term Os odontoid when the tooth is separated from the body of the axis [2].
In 1974 Fielding was the first to hypothesize the traumatic origin of the Os odontoid due to poor consolidation of a fracture or due to vascular compromise at the time of the fracture. Other authors propose its congenital origin due to its association with various etiologies such as Down's syndromes, Klippel-Feil, epiphyseal dysplasia, Morquio syndrome, which by postmortem studies reveal bone or ligament changes compatible with congenital malformations [2].
The odontoid process develops between the anterior ring of the atlas ventrally, the dorsal ligament of the atlas and its lateral mass. Any sudden movement predisposes to a rupture of the odontoid or the transverse ligament of the atlas and to the instability of the atlas on the axis with the potential neurological damage or death. Identification of the Os odontoid is usually accidentally performed in the emergency department, after routine performance of a cervical x-Ray. It usually manifests as local neck or occipital pain, torticollis or with clinical symptoms of a brainstem or cervical injury, and may be accompanied by seizures, dizziness or visual symptoms [30].
Once diagnosed, it must be taken into account if it is asymptomatic or not. Speirings et al [30]. In 1975 analyzed 37 asymptomatic cases of which 20 were treated without surgery and 17 surgically, with no differences in the two groups in the medium and long term [30,31].
Rheumatoid Arthritis is an inflammatory disease mainly of the diarthrodial joints, cellular and tissue involvement is identified by the formation of the pannus, the destruction of the articular cartilage, ligaments, tendons and bone structures. The most destructive element is Pannus, granulation tissue composed of proliferating fibroblasts, blood vessels, and various types of inflammatory cells. Collagen and proteoglycans appear to be altered in the region immediately adjacent to mononuclear cells at the cartilage-pannus junction [31].
The deformities that can be found in patients with compromised cervical spine are: atlanto-axial instability (65%), atlanto-axial impaction (20%), subaxial subluxation (15%) [31].
The posterior atlanto-dental distance (PADI) is the distance measured between the posterior surface of the odontoid and the anterior aspect of the posterior arch of C1, being one of the most important predictors of risk of neurological deficit. Boden et al., Established that a PADI less than 14mm is correlated with the development of paralysis8. It should be remembered that the PADI does not represent the free space for the spinal cord, since the pannus is not visible on radiography, so that patients with values greater than 14mm may present medullary compression, the preoperative PADI can also be used to predict the recoverability of the patients to be operated, the patients with a PADI less than 10mm presented little neurological recovery, those in which the PADI was greater than 10mm presented some degree of recovery. The Ranawat index measures the distance between the center of the C2 pedicle and the transverse axis of the atlas, through the axial axis of the odontoid. Values less than 15 mm in men and 13 mm in women are considered altered [31-33].
However, if the lesion extends below the palatine line, an endonasal route is not necessarily contraindicated. Several authors have proposed various methods of predicting the inferior limit of the endonasal approach by drawing anatomical lines on sagittal CT scans. The nasopalatine line (Kassam line) was previously proposed to predict this inferior limit by drawing a line from the rhinion toward the posterior edge of the hard palate that continues toward the craniovertebral junction. However, the nasopalatine line seems to overestimate the inferior limit of the approach by approximately 6–12 mm. The trajectory and angle of this line are often too steep and are not reproducible in clinical settings, because the line does not take into account the soft tissue limitations of the nare. To provide an alternative, Aldana et al. described the nasoaxial line, which is drawn from the midpoint between the rhinion and the anterior nasal spine that extends toward the posterior edge of the hard palate and continues toward the craniovertebral junction. In the cadaveric study, the nasoaxial line was more accurate in predicting the inferior limit of the endonasal endoscopic approach than the nasopalatine line. In our practice, we generally use the palatine line and the nasoaxial line to determine the optimal surgical approach (figure 7). If the lesion extends beyond the reach of the nasoaxial line, a transoral approach (which can be performed endoscopically as an endoscopic transoral approach) can be used alone or in combination with the endoscopic endonasal approach, if needed. In addition, preoperative dynamic plain radiographs in flexion and extension views should be obtained to assess for preexisting instability at the craniovertebral junction. Even if there is no instability present, most patients will require posterior occipitocervical stabilization and fusion because of iatrogenic instability after resection of the odontoid and involved ligaments [17].
For these specific cases, we use the surgical approach with the best reach for the surgeon, as well as the best solution for the patient. One of the drawbacks with this surgical technique is discomfort for the surgeon, the small microsurgical workspace that occurs during proceeding. But it is an approach to consider when you do not have all the necessary tools and you must take appropriate surgical behavior.
Both the transoral and endonasal endoscopic approaches have their precise indications in each particular case, having their indications well defined. To achieve this, we must have neuroimaging studies and be able to correctly define the selection of the surgical approach. This is not the case with the standard microsurgical transoral approach, which is becoming increasingly obsolete, due to the delay in proceeding and the limited scope of the surgical field, while the endoscopic approach is faster, with better visualization and is accompanied by fewer complications.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
