
Case Report | DOI: https://doi.org/10.31579/2640-1053/118
1 Dept of Surgical Oncology, Currae Cancer & Multi speciality Hospital, Mumbai, India
2 Dept of Ophthalmology, Conwest & Jain Super speciality Eye Hospital, Mumbai, India
*Corresponding Author: Aniket Adhikari, Dept of Surgical Oncology, Currae Cancer & Multispecialty Hospital, Mumbai, India.
Citation: Aniket Adhikari, Madhusnata De. (2022). Endometrial Cancer with Cervical Extension Masquerading as Cervical Cancer. Cancer Research and Cellular Therapeutics. 6(3); Doi:10.31579/2640-1053/118
Copyright: © 2022 Aniket Adhikari, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 April 2022 | Accepted: 04 May 2022 | Published: 12 May 2022
Keywords: cervical Cancer; immunohistochemistry; hysterectomy specimen
The incidence and prevalence of endometrial cancer is less as compared to cervical cancer. Worldwide, in 2018, near about 382000 new cases of endometrial cancer were diagnosed and around 90000 women were died from the disease
The incidence and prevalence of endometrial cancer is less as compared to cervical cancer. Worldwide, in 2018 , near about 382000 new cases of endometrial cancer were diagnosed and around 90000 women were died from the disease [ 1 ]. In India, in 2020, endometrial cancer ranks at 22nd position with incidence around 1.2%, mortality around 0.75% and 5-year prevalence around 6.56 % which is very low as compared to cervical cancer which ranks at 3rd position with incidence, mortality and 5-year prevalence as 9.4%, 9.1% and 42.82 % respectively [2]. The risk factors for endometrial cancer are early age at menarche, late onset menopause, use of tamoxifen, elderly patient (> 55-60 years) and obesity [3, 4]. The diagnosis of endometrial cancer is confirmed with clinical approach, imaging studies and endometrial biopsy. In some cases, it becomes difficult to define the epicentre of the tumor whether it is arising from endometrium or cervix as the treatment approach is different for both of the carcinomas. In this scenario, the best possible tool is panel of immunohistochemistry on the hysterectomy specimen.
A 52-year-old postmenopausal lady with Eastern Co-operative Oncology Group Performance
Status 1
(ECOG PS – I) with no co-morbidity presented with per vaginal bleeding for the last 3 weeks. There was no supportive family, past, surgical and medical history. She consulted a gynaecologist and underwent biopsy from the cervix as the consulting gynaecologist found a bulky cervical mass. It was reported as differential diagnosis of squamous or adenosquamous carcinoma of cervix and immunohistochemistry was advised. As the diagnosis was in favour of carcinoma of cervix, she had underwent MRI of pelvis which was suggestive of bulky cervix with mass lesion arising from both the lips of cervix measuring 6x5.5cm with free bilateral paracervical and parametrial margins with no pelvic or paraaortic lymphadenopathy. With these reports, she visited our clinic. Systemic examination was unremarkable and local examination was suggestive of bulky cervical lesion of size 5x4cm with non-involvement of bilateral parametrium. We had advised CECT (Contrast Enhanced Computed Tomography) of thorax and upper abdomen for metastatic staging which was suggestive of no pelvic or paraaortic lymphadenopathy with no distant metastasis. As MRI pelvis, clinical examination and biopsy report was in favour of cervical cancer, our institutional multidisciplinary tumor board had advised radical hysterectomy with bilateral pelvic lymph node dissection sos paraaortic lymph node dissection. Hence, patient underwent the above-mentioned procedure. Intraoperative, paraaortic lymph nodes were not enlarged, so we didn’t go for it. Postoperative course was uneventful and she was discharged on 6th postoperative day.
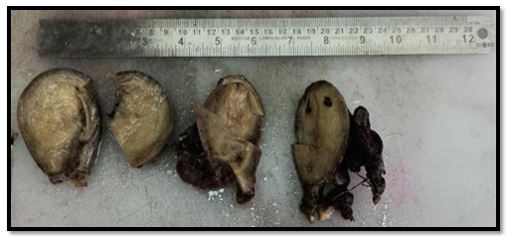
During gross examination of the specimen, it was found that the epicentre of the tumor was located in the isthmus of endometrium and not arising from cervix (Fig. 1& 2). It was an endometrial tumor projecting into the vagina mimicking like cervical carcinoma. However, half thickness of the cervical stroma was infiltrated by the tumor with full thickness myometrial involvement and serosa was free. Around 20 bilateral pelvic lymph nodes were removed which were free from metastasis. On immunohistochemistry, tumor cells were showing expression of ER, PR and Vimentin with focal expression of CEA. Hence, final impression was endometrioid adenocarcinoma and 8th edition AJCC staging was suggestive of p T1b pN0 pM0. She had been advised adjuvant radiation therapy and she completed it without any major adverse effects. After two years of completion of treatment, she is still disease free.

The optimal management of patient depends on the final histopathology, whether the lesion is arising from cervical or endometrial lining. There are number of causes which makes the task of diagnosis difficult. Thus, the distinction of origin of endometrial adenocarcinoma becomes very difficult. There are chances of overlapping of morphology by tumor on both sites i.e imaging and biopsy specimen. Sometimes, the dominant tumor component in the hysterectomy specimen may not represent the primary site. In these cases, immunohistochemical analysis is helpful in achieving the final diagnosis and standard panel of markers are helpful in distinguishing endometrial and cervical adenocarcinoma.
The differential diagnosis of a mass involving the cervix, the available options are a primary endometrial carcinoma arising in the fundus with extension into cervix, a primary endometrial carcinoma arising in the lower uterine segment with secondarily involving the cervix or a primary cervical carcinoma. There are 30% chances of association of lower uterine segment endometrial cancer with Lynch syndrome [5]. Hence, for evaluation of Lynch syndrome, it is necessary to do mismatch repair immunohistochemistry or polymerase chain reaction (PCR)-based microsatellite instability analysis.
Magnetic resonance imaging (MRI) is the best modality of imaging as compared to computed tomography (CT) or ultrasonography in defining the location and extent of endometrial cancer i.e. whether it is invading myometrium or cervix. The overall staging accuracy of MRI is between 85-93% [6]. In about 10-15% of cases, endometrial cancer invades cervical canal [7]. The reported sensitivity and specificity of MRI in the detection of cervical involvement from endometrial cancer are 72% and 93% respectively with reported positive and negative predictive values are 90% and 80%, respectively [8]. In the index case, primary investigation advised was MRI which was suggestive of cervical origin of the tumor and biopsy was in favour of carcinoma cervix.
As per 2019 National Comprehensive Cancer Network (NCCN) Guidelines [ 9 ], for patients with suspected or gross cervical involvement or If there is clear demonstration of cervical stromal involvement on imaging and if the patient has no absolute contraindication to surgery, then one may elect an option of surgery which includes a total simple hysterectomy or a radical hysterectomy and bilateral salpingo-oophorectomy, along with surgical staging with the consideration of sentinel lymph node mapping. The index case underwent radical hysterectomy as bilateral parametrial and paracervical tissues were free. In these situations, there are chances of parametrial margins will come positive. It was a post-surgery specimen which changed the complete scenario with the help of IHC markers. Hence, patient with bulky cervical mass needs proper attention from the team of treating surgeon, radiologist and pathologist.
The incidence of endometrial cancer extending into cervical stroma is very low. The final diagnosis is based on location of epicenter of tumor and standard immunohistochemistry panel markers.
Human subject: Informed consent was obtained from the patient for being included in the study.
The authors declare that they have no conflict of interests.
All authors have declared that no financial support was received from any organization for the submitted work.
All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Not applicable.
An informed consent to publish this case was obtained from the patient.
Not applicable.
Not applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
