
Research Article | DOI: https://doi.org/10.31579/2690-1919/284
Professor of Psychology at the Faculty of Psychology/ Havana University
*Corresponding Author: Humberto Garcia Penedo. Professor of Psychology at the Faculty of Psychology/ Havana University.
Citation: Humberto Garcia Penedo. (2023). Emotional comorbidities in drug addictions. Recount and thematic review, J. Journal of Clinical Research and Reports, 12(3) DOI:10.31579/2690-1919/284.
Copyright: © 2023 Humberto Garcia Penedo. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 December 2022 | Accepted: 28 December 2022 | Published: 06 January 2023
Keywords: Emotional comorbidities; complicated grief; anxiety; depression; testimonials; drug addiction; psychotherapy; psychotrauma; Bibliotherapy
It is a thematic review where the author's path in scientific research focused on enhancing the effectiveness of psychotherapeutic treatment of people with alcoholism or any other drug addiction and the results of published studies are exposed. The thematic review focuses on the neurotic level affective spectrum comorbidities in drug addictions from the progressive understanding of this author in the professional practice with Cuban and Latin American patients. The logic followed in scientific research and its outcome towards an effective professional practice in psychotherapy in this area of clinical psychology is narrated. The state of the art in the Cuban user population of these services is reported, the value of resources and psychotherapeutic strategies that give prestige to the work with the emotional area of users of the addiction service is based, since they seem to contain a greater potential for effectiveness to fulfill psychotherapeutics objectives.
Delving into the professional practice of assisting people with drug and alcohol addiction is a challenge given the complexity of these problems. After a 12-year work experience in the Rogelio Paredes Teaching Psychiatry ward of the Psychiatric Hospital of Havana as a clinical psychologist and under the direction of Ph.D. Ricardo Á. González Menéndez, starting in 1995, it was possible to assist people with varied drug addictions and of different nationalities, especially from Cuba and Latin America. At the beginning, I was instructed to carry out didactic groups that would have the objective of reinforcing the instructional part of the assistance program of the service; since its contents or methodology to implement it weren’t developed yet at that time, work was done to define which instructional contents would emerge from the needs felt and expressed by the service users themselves.
These demands were also nourished by the very logic of the care process, issues that were published [1,2,3], so that they contributed to Psychoeducation in this area. However, although this complementary assistance modality was developed by this author, its effects would be restricted to the cognitive area of the problem and, although useful, it was obvious that it would be necessary to continue looking for other procedures that would contribute to strengthening the assistance program of these people, since it is proposed that drug addictions are essentially an emotionally based problem [4,5].
Affective comorbidities in addictions are very frequent, more than 65% in a Spanish study in which patients with mood, psychotic anxiety, ADHD and personality predominated [6]. Anxiety and depression are the rule in these people [7,8], anger is also very common [9,10]. The Unpleasant Affect factor declared by several authors and which consists of a significant group of negative emotions has the greatest weight in its association with the craving for consumption [11].
Effective treatment in people with addictions becomes more complex to the extent that different types of comorbidities appear, although the most frequent are neurotic, in addition to the fact that in some cases elements of drug-induced psychosis appear. Care programs for this problem have been characterized by being multimodal [12], which means that different types of psychotherapy are used because each one provides benefits to meet certain psychotherapeutic objectives of proven efficacy.
For years the slogan has been heard that says: "What is effective is what is affective" but even when there was an intuition about the veracity of this maxim, at the beginning there wasn't a sufficient idea that would allow the implementation of interventions that would be effective in the treatment of people with drug addiction. It was noteworthy that many individuals upon admission to the psychiatric service declared that they had made that decision after having suffered an event of high social and personal significance resulting from their negligent behavior associated with drug use. A patient, for example, decided to enter after having pushed his pregnant wife and having lost the child for that reason, another patient was admitted after being sentenced to non-conviction correctional work because under the influence of alcohol while transporting his mother in the back seat of his bicycle collided with a vehicle on a slope and she died days later.
After the compilation of reference anecdotes was elaborated, it had to be tested while studying the best way to use it in assistance. Professional practice has shown that nothing is better than the confession of anecdotes of patients presents for psychotherapeutic work, while anecdotes compiled whose protagonists were patients who were no longer present and whose anonymity was reserved, would be better used as a complement in case of not obtaining immediate confessions that would serve to “emotionally warm up” a psychotherapeutic environment [16]; procedure that proved to be effective in the treatment of these people.
Once the effective potential of an approach centered on “the affective” was certain, it continued to be thought of adding other intervention procedures that would contribute to further reinforcing the care program. The integration of contributions from Neuroscience and studies on trauma would be key pieces that would be integrated into the intervention system. In 2006 two patients suffering from chronic alcoholism were treated but they had in common that they both suffered from a complicated mourning.
Patient “A”, a farmer who began his career of binge drinking after losing his father who suffered from alcoholism and committed suicide in front of him and his mother by drinking a pesticide. Patient "B" also began abusing alcohol from the moment his little brother, under eight years old, was accidentally crushed to death by the collapse of an old building where he was playing. As his mother was taking a nap, "B" blamed her for being responsible and for 21 years he mistreated and humiliated her a lot, he denied her all affection; while "A" imitated the embarrassing behavior of his father in life, both alcohol consumption and pathological gambling.
A mourning technique was applied to both patients, managing to overcome it despite the chronicity of this disorder (18 years in "A" and 21 in "B"); miraculously, the latter never drank alcohol again, he reconciled with his mother whom he kissed after 21 years without kissing her and called her "mom"; although forgiveness was a required step in this therapy; while "A", on the other hand, despite having overcome the mourning, relapsed six months later for a typical reason that explains the relapse of many patients with alcoholism, but his recovery was very fast and his relapse was free from the onslaught of the previous complicated mourning.
Grief turned out to be primary in both cases with respect to alcoholism, a typical example of a Mental Illness Substance Abuse (MISA) case; this solution was decisive in the recovery from alcoholism. How many psychiatric pathologies associated with addictions as comorbidities are influencing the chronicity of the latter? It is obvious that the comprehensive treatment of comorbidities contributes to enhancing the effectiveness of treatments, in fact the DSM in its most current version registers the category "Disorders related to traumas and stress factors" where very relevant disorders are reflected from their symptomatic composition due to the impact of traumas, but clinicians have to deal with a myriad of traumas that, due to their peculiar composition and expression of the psychopathological frame, are not classified as well in the disorders included in the reference diagnostic category, but are included within the trauma model as stated [17].
From this approach, it is known that there are dissimilar modalities of trauma experienced by people in very personal ways, attenuated clinical forms of what could be a Post-Traumatic Stress Disorder (PTSD), suitable for people who learned to live badly with these traumas and they establish interpersonal relationships that reflect social dysfunction as an expression of sequelae of events perceived by them as psychotraumatic.
From the aforementioned approach, by identifying affective comorbidities and treating them appropriately, the chances of successful treatment are high. Now the diagnosis that clarifies the entire affective spectrum is of great value to fine-tune the psychotherapeutic strategy, since by personalizing the diagnosis it also allows treatment to be individualized [6]. Although this premise is not new, it has gone through a defect that has been affecting the effectiveness and efficiency of assistance programs; even when the psychopathological categories are diagnosed from the categorical paradigm that doesn’t dictate enough about the patient. Depression, for example, is identified and ruled generically in around 50% of patients, but its character as a trait is not always judged, nor is the treatment always completely consistent with this fact, nor is it usually described emotional composition of that disorder, something that doesn’t help to personalize the treatment.
When focusing attention on depression, especially trait one, it is logical to think that the person has incorporated attitudes, beliefs, and behaviors that perpetuate the disorder into their usual way of being, and this already leads us to think about their synaptic connectivity substrate. Taylor [19] calls it "automatic or pre-programmed reactivity of the limbic system", meanwhile Maté [20] names it "brain patterns" or “programs of early painful experiences”, while Lewis [21] calls this "neural habits".
On the other hand, although depression has shared symptoms and signs, people often suffer from their anguish or discomfort personally, hence the need to identify which negative emotions are part of its composition, since some people are sad with feelings of guilt, of frustration, of a low self-esteem, while others feel hatred, resentment towards other people and expectations of harm that place them in defensive and even offensive attitudes towards others. Therefore, there is a group of negative emotions that do not in themselves constitute a psychopathological diagnosis, but that acquire a high social significance for those who suffer from an addiction. In the article by Von Hammerstein et al. [11], it can be seen that these authors name "Unpleasant affect" to a factor composed of dissimilar emotions including stress, shame, disappointment, anxiety, frustration, among others, which they declare that are associated with the craving; this means that these emotional experiences precede craving and enhance it.
These differences in emotional composition that individuals suffers are originally related to events perceived as traumatic that engendered negative predispositions in these people, which are what explain social dysfunctionality, according to Shapiro [17] and which was verified by this author in investigative practice [18]. This emotional pattern expresses the set of preconceived responses of these people to new situations that are perceived as a potential repetition of very unpleasant past experiences and that they intend to prevent from happening again. This is how a psychological trauma operates in its composition and functionality, which is found in many people with addiction in clinical practice [3]. This belief repeatedly observed by Maté was what led him to consider addiction as a secondary disorder with respect to its importance and rescue the harmful impact of traumas when he stated: “The question will never be: why addiction? Otherwise why the pain? (p.43) [20].
The addictive cycle according to Volkow [22] includes a very important component that is that of negative emotions, this reaches its maximum influence when the individual pauses in drug use and is emotionally knocked down, at the same time, that the same emotional state, being perceived as unbearable, contributes to enhancing the craving for consumption and drags the patient towards the next phase of preoccupation-anticipation before entering the binge. In this emotional component, a very valuable gateway is distinguished to enhance psychotherapeutic assistance, either when solving a complicated mourning, or when treating depression from a trait perspective in which trauma is conceived in the genesis of a large part of the psychopathological alterations of the patients.
The various negative emotions are designed to be experienced in a transitory and not permanent way. Nothing is more normal than a person feeling anger at a well-justified person and circumstance, which does not mean that the person should remain under anger all the time as happens with feelings. The same can be said of other negative emotions that must be transitory and circumstantial.
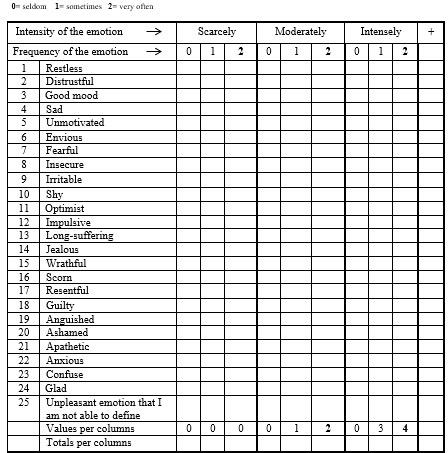
On the other hand, there are people who have incorporated negative emotions into their usual way of perceiving and reacting, which makes them vulnerable to a high number of social experiences; hence the basis for designing a psychometric instrument that allows trait emotionality to be identified based on its frequency and magnitude, both of which make up what has been called its clinical significance. Anger, being very frequent in addicted people [9], led to the design of a program for its treatment [10]; however, Alcoholics Anonym ous themselves state the following: “The greatest enemies of us alcoholics are resentment, jealousy, envy, frustration and fear.” (A.A. Blue Book p. 108). These emotions, reflecting a notable level of clinical significance, become the focus of the therapist's interest and lead to the identification of which traumatic experiences they are originally associated with. To diagnose this entire set of aforementioned emotions, an instrument was designed that has proven to be very relevant, the Modified Grau's Experiential Self-Report [23,24] (See appendix 1).
This instrument records a total of 25 emotions, of these 22 are negatives and three positives, those that obtain clinical significance will be worked on in psychotherapy with the patients. To complement this instrument, a Rotter (a sentence completion) was designed that focuses on questions that explore emotionality so that it is possible to identify which specific topics these emotions are associated with in order to clarify which past events they are originally linked to. Together with these two instruments, an interview guide is used to conclude the investigation about the psychotraumatic event or events that the patient must have gone through.
The strategy to follow for the treatment of this unhealthy emotional composition, although it is based on Shapiro's theory about its origin and shares with this author to meet the same specific objectives, is based on the Corrective Emotional Experience of Alexander and French (1949) with elements in addition to Greenberg and Watson [25]. Therapy Focused on Emotions for being very effective for these cases. The psychopathological diagnosis should not be restricted to the categorical paradigm but should include the report of dimensions that facilitate the understanding of each case; in particular, the negativity composed of negative emotions identified against the positivity composed of qualities such as optimism, good humor and happiness reported by individuals. Both dimensions are very relevant to work on the emotional area of these patients. The positivity deficit bases the need to promote emotional health that contributes to psychological well-being, while the removal of negativity will be a goal of the therapist with the conviction of suppressing the source that potentiated the anxiety. These bases demonstrated therapeutic effectiveness [24].
The follow-up of a part of the patients who were assisted with this approach showed that they have remained abstinent for a long time, some for four years after this study was carried out. This perspective shows that assistance programs are perfected in the growing integration of good practices; classic psychotherapeutic methods together with the somewhat newer ones and the gradual conviction of seeing emotional comorbidities more as an opportunity than as a stumbling block. An important implication of this approach favors combating the stigma that seeks to delegitimize addiction as a disease, the less it is shown that it is one more way of expressing affective spectrum disorders. It also shows that, although this addictive structure and dynamic is not fulfilled in all patients, in those in whom it is fulfilled they are suitable creditors to be benefited from this perspective, their resources and strategies predicting effectiveness in treatment, in addition, although addictions are they settle on a peculiar neuroconnectivity although of social origin, it is modifiable with psychotherapy.
Appendix No.1
Grau's Modified Emotional Self report
Instructions: To the left column there are a series of emotions that you could feel. To the right of each one there is a horizontal line whose left end indicates the weakest grade in that you feel these emotions, while the right end corresponds to the biggest intensity in that you may has felt them.
1.- You should check only one box per row where you think best reflects the intensity with which you have been feeling each emotion during the last few months. Please make sure to match the chosen intensity with the frequency in which it occurs.
Affective comorbidities in drug addictions represent a major challenge in treatment but at the same time, understanding how negative emotions become traits are formed and operate and the role of traumas in their origin, their treatment also represents a path that predicts the effectiveness of therapeutic assistance, since when affective comorbidities are resolved, patients reach a more favorable health condition to initiate and sustain abstinence in consumption for a longer time. Focusing on trait emotionality and trauma seems to add greater effectiveness to care; also, the more detailed psychopathological diagnosis allows to personalize the treatment, both conditions contribute to the effectiveness of the treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
