
Review Article | DOI: https://doi.org/10.31579/2640-1053/184
1Al-Hadi University College, Baghdad, Iraq.
2Department of Biochemistry, Science Faculty, Menoufia University, Menoufia, Egypt
3MLS ministry of health, Alexandria, Egypt. - MLS ASCP, USA.
*Corresponding Author: Tamer A. Addissouky, Al-HADI University College, Baghdad. Iraq. - Department of Biochemistry, Science Faculty, Menoufia University, Egypt. - MLS ministry of health, Alexandria, Egypt. - MLS, ASCP, USA.
Citation: Tamer A. Addissouky, Ibrahim El Tantawy El Sayed, Majeed M. A. Ali, (2024), Emerging Biomarkers and Targeted Therapies Reshaping Clinical Management of Colorectal Cancer, J. Cancer Research and Cellular Therapeutics, 8(2); DOI:10.31579/2640-1053/184
Copyright: © 2024, Tamer A. Addissouky. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 January 2024 | Accepted: 01 February 2024 | Published: 28 February 2024
Keywords: colorectal cancer; immunotherapy targeted therapy; precision medicine biomarkers
Background: Colorectal cancer (CRC) is a leading cause of cancer deaths worldwide. Key risk factors include lifestyle, diet, inflammation, and family history. Understanding molecular pathways underlying CRC initiation and progression is critical to guide prevention and treatment.
Purpose: This review summarizes recent advances in CRC screening, therapy, and future directions.
Main body: New stool DNA panels and blood-based assays offer non-invasive options for early CRC detection, though require further validation. Immuno- and targeted therapies matched to tumor molecular profiles have transformed metastatic CRC treatment. Pembrolizumab elicits durable responses in mismatch repair-deficient tumors, and anti-EGFR antibodies cetuximab/panitumumab improve outcomes for left-sided RAS/RAF wild-type CRC. Larotrectinib and entrectinib are highly active in NTRK fusion-positive CRC. Research focusing on new immunotherapies, leveraging the microbiome, and combining multi-omics data to enable precision medicine holds promise. Disparities across groups remain a challenge.
Conclusions: Recent therapeutic advances have significantly improved survival for metastatic CRC patients. Advances in non-invasive diagnostics, next-generation sequencing, and computational approaches will enable more sophisticated molecular profiling and tailored therapy selection. Realizing the potential of emerging immunotherapies and integrating knowledge of the microbiome remain important frontiers.
Colorectal cancer (CRC) remains one of the most prevalent cancer diagnoses and leading causes of cancer mortality worldwide. Global disease burden has risen in tandem with adoption of certain dietary and lifestyle changes in economically transitioning countries. Understanding key risk factors and pathogenic mechanisms is imperative to guide prevention and treatment strategies [1-3]. Established environmental and lifestyle risk factors for CRC beyond screening non-adherence include smoking, heavy alcohol intake, obesity, consumption of processed or red meat, and low dietary fiber/vegetable intake. Chronic intestinal inflammation is also an important risk factor, as seen in inflammatory bowel disease. Family history of CRC confers increased risk, and several inherited cancer syndromes like Lynch syndrome dramatically predispose to early-onset CRC. Recently, the gut microbiome has emerged as a potentially important modifiable factor, though mechanisms require further characterization [4-8]. Understanding how these exposures drive CRC initiation and progression at the molecular level remains an area of active investigation. Key pathogenic pathways include chromosomal instability, microsatellite instability, and CpG island methylator phenotype pathways which dictate patterns of genetic mutations arising in tumors. Recent research has also focused on altered metabolic, inflammatory, and immune pathways within the tumor microenvironment which enable growth and metastasis [9].
Early Diagnosis and Screening
Detecting colorectal cancer (CRC) at an early stage is critical, as 5-year survival drops precipitously from 90% for localized disease to 14% for metastatic cancer. While screening has improved early diagnosis, novel modalities beyond colonoscopy and stool testing are emerging as depicted in table 1. In 2014, Cologuard, a multitarget stool DNA test, was FDA-approved for CRC screening based on superior sensitivity to standard fecal immunochemical testing. However, concerns remain regarding specificity. Plasma-based tests like Epi proColon (methylated SEPT9 DNA) and OncoBEAM (mutant KRAS/NRAS DNA) are now commercially available as screening tools, though evidence is still limited [10-11]. An area of active research is development of blood-based biomarkers for early detection. Circulating tumor cells (CTCs), cell-free tumor DNA, exosomes, miRNAs, proteins, and metabolites are all under study as non-invasive diagnostic markers. Recent advances have identified methylated gene panels, glycosylated protein markers, and metabolite signatures that can discriminate CRC from controls with high accuracy [12-24]. Machine learning and artificial intelligence tools applied to medical imaging and liquid biomarkers show enormous potential to transform early diagnosis. Deep learning algorithms can synthesize diverse data sources into predictive models. However, extensive further validation is required before clinical implementation [25-33]. While colonoscopy remains the gold standard, the advent of stool DNA panels, blood-based assays, and AI-enhanced imaging offer new options for non-invasive screening that could significantly improve early detection and save lives. But rigorous assessment of clinical utility and cost-effectiveness remains needed as these tools continue to evolve [34-35].
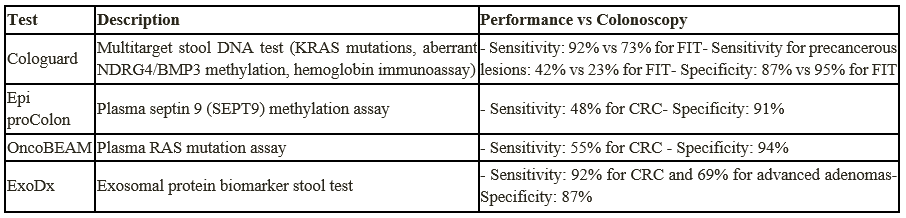
Table 1. Emerging Non-Invasive Screening Tests for Colorectal Cancer
Advances in Treatment and Innovative Therapeutics
The treatment landscape for colorectal cancer (CRC) has been transformed over the past decade by the arrival of new chemotherapeutic regimens, immunotherapies, targeted agents, and a growing emphasis on precision medicine. Significant gains have been made in systemic therapies for metastatic CRC, extending and improving quality of survival. Several new chemotherapy backbones and combinations have been established through positive randomized phase III trials and endorsed in clinical guidelines. The FOLFOXIRI regimen (folinic acid, 5-fluorouracil, oxaliplatin, and irinotecan) plus bevacizumab has become a standard first-line option for eligible metastatic CRC patients based on significant extensions in median progression-free and overall survival compared to doublet chemotherapy plus bevacizumab. For patients progressing after first-line treatment, addition of the novel vascular endothelial growth factor (VEGF) inhibitors ramucirumab or regorafenib to continuous 5-fluorouracil-based chemotherapy was shown to provide a survival advantage. The multikinase inhibitor regorafenib also showed activity as monotherapy in phase III trials [36-37].
Beyond chemotherapy, arguably the most exciting advances have come in the form of immunotherapy and targeted therapies directed against specific molecular aberrations. After demonstrating remarkable activity in microsatellite instability-high (MSI-H) solid tumors, pembrolizumab and nivolumab have emerged as mainstream options for metastatic CRC patients whose tumors exhibit mismatch repair deficiency (dMMR) or high microsatellite instability (MSI-H). The pivotal phase II CheckMate-142 trial established pembrolizumab as an effective therapy for previously-treated MSI-H/dMMR metastatic CRC, eliciting an immune-related objective response rate of 31%. Building on this, KEYNOTE-177 established pembrolizumab monotherapy as superior to standard chemotherapy in the first-line setting for this population. Ongoing studies are assessing pembrolizumab in combination with chemotherapy backbone, epidermal growth factor receptor (EGFR) inhibitors, or MEK inhibitors as initial therapy for metastatic MSI-H/dMMR CRC. Beyond MSI-H/dMMR disease, research is ongoing into other potential immunotherapy biomarkers and rational combination strategies to extend benefit to broader groups of CRC patients [38-40]. In parallel, monoclonal antibodies and small molecule inhibitors targeting key oncogenic drivers matched to specific biomarkers have moved into standard practice. Cetuximab and panitumumab, monoclonal antibodies directed against EGFR, are now firmly established components of therapy for left-sided RAS/RAF wild-type metastatic CRC. Multiple trials have proven superior outcomes with the addition of these biologics to chemotherapy backbones for this molecularly defined population. Though less common, actionable NTRK and BRAF mutations also now have clinical grade targeted therapies. Larotrectinib and entrectinib, highly selective tropomyosin receptor kinase (TRK) inhibitors, elicit rapid and often durable responses in the small subset of CRC tumors harboring NTRK fusion genes. Encorafenib (BRAF inhibitor) combined with anti-EGFR antibody cetuximab shows excellent efficacy in BRAF-mutant CRC based on the BEACON trial. While these targets affect a smaller proportion of patients, the activity of matched targeted agents is dramatic and provides proof of concept for ongoing biomarker-driven drug development [41-43].
Traditional Medicine
Some traditional herbal medicines and practices derived from ancient healing systems have shown potential anti-cancer benefits against colorectal cancer in preliminary cell line, animal, and early human studies. Most mechanisms relate to anti-inflammatory, antioxidant, and anti-proliferative properties. Curcumin, a polyphenol derived from turmeric, can inhibit growth and metastasis of colorectal cancer cells through regulating multiple signaling pathways. A small clinical trial in colorectal cancer patients found curcumin combined with chemotherapy reduced tumor cell proliferation compared to chemotherapy alone. Other polyphenols like EGCG from green tea, resveratrol from grapes, and silibinin from milk thistle also demonstrate anti-cancer effects. The traditional Chinese medicine formula PHY906, containing Scutellaria baicalensis (Huang Qin), has been shown in mouse models to normalize intestinal microbiota and reduce chemotherapy-induced toxicity. A phase I/II trial in patients with advanced colorectal cancer suggested PHY906 plus capecitabine improves progression-free survival compared to capecitabine alone. Larger randomized trials of PHY906 are underway [44-47].
Nanomedicine
Nanomedicine utilizes specially engineered nanoparticles (NPs) sized 1-100 nm for cancer imaging, drug delivery, and theranostics. Over the past decade, NP platforms have made significant progress towards clinical implementation for colorectal cancer. Dozens of NP constructs have been studied for colorectal cancer drug delivery, including liposomes, dendrimers, carbon nanotubes, and inorganic nanoparticles. Liposomal irinotecan received FDA approval in 2015 based on improved progression-free survival compared to standard irinotecan in metastatic colorectal cancer. Iron oxide, gold, and silica NPs have demonstrated potential as highly sensitive contrast agents for enhanced colorectal cancer imaging. Tumor-targeted gold NPs also enable photothermal ablation of tumors when exposed to near infrared light. An exciting development is the emergence of theranostics - NPs that integrate therapy and diagnostics into a single platform. For example, new approaches use fluorescent silica NPs to improve tumor visualization during surgery, while loaded with chemotherapeutics for sustained postoperative treatment [48-50].
Future Directions
While recent years have seen impressive advances in colorectal cancer across multiple fronts, significant opportunities and challenges remain to further progress. Exciting new innovations in treatment, diagnostics, and prevention on the horizon warrant expanded research. Novel immunotherapies offer new paradigms in activating anti-tumor immunity. Beyond immune checkpoint inhibitors like pembrolizumab, ongoing research is exploring cancer vaccines, CAR T cells, oncolytic viruses, and combination immunotherapies. These approaches aim to generate more durable responses than current options [51-53]. Leveraging the microbiome therapeutically also holds promise. Fecal microbial transplantation to restore intestinal homeostasis and probiotics/prebiotics to prevent colitis show potential to reduce colorectal cancer risk. Additional research is needed to identify mechanisms and optimal approaches [54-56]. Expanding our understanding of colorectal cancer genetics and immunology will enable more sophisticated molecular profiling, guiding personalized precision medicine. Multi-omics integration and systems biology modeling will provide a more comprehensive view of CRC carcinogenesis [57]. Detecting pre-malignant polyps and early-stage tumors remains challenging. Development and validation of blood or stool biomarkers, through proteomics, metabolomics, and epigenetics, is a key priority. AI-enhanced imaging and endoscopy could also improve screening [58-59]. Disparities persist in CRC incidence and outcomes across socioeconomic, geographic, and racial/ethnic groups. Resolving these inequities requires coordinated efforts targeting risk factor reduction, screening access, diagnosis delays, and treatment availability [60]. Multidisciplinary collaboration harnessing new technologies will accelerate progress against colorectal cancer. Advances in genomics, immunotherapy, nanomedicine, applied AI, and precision diagnostics bring hope for improved outcomes and will shape the future of CRC research.
Recent years have witnessed remarkable progress in the treatment of metastatic colorectal cancer, with median overall survival improving from around 12 months with older chemotherapy regimens to over 30 months with modern combination strategies incorporating targeted agents and immunotherapies matched to specific biomarkers. Looking forward, leveraging rapid advances across fields including genomics, immunotherapy, nanotechnology, and artificial intelligence offers immense opportunities to further advance screening, diagnosis, prevention, and therapeutic decision-making for colorectal cancer. Key priorities include developing and validating non-invasive biomarker approaches to enable earlier detection, expanding insights into colorectal cancer genetics and immunology to extend precision medicine approaches to larger groups of patients, further characterizing the role of the microbiome in colorectal carcinogenesis and response to therapy, designing innovative clinical trial methodologies to efficiently assess emerging immunotherapies and targeted agents matched to lower frequency biomarkers, and applying cutting-edge computational tools to synthesize diverse multi-omics data sources into predictive models guiding personalized therapy selection while accounting for inter- and intra-tumor heterogeneity.
Recommendations:
Several recommendations can be made to accelerate progress against colorectal cancer:
CRC - Colorectal Cancer
EGFR - Epidermal Growth Factor Receptor
CMS - Consensus Molecular Subtypes
NPs - Nanoparticles
AI - Artificial Intelligence
FIT - Fecal Immunochemical Test
dMMR - Mismatch Repair Deficient
MSI-H - Microsatellite Instability-High
PD-1 - Programmed Death-1
PFS - Progression-Free Survival
OS - Overall Survival
Ethics approval and consent to participate: Not Applicable
Consent for publication: Not Applicable
Availability of data and materials: all data are available and sharing is available as well as publication.
Competing interests: The authors hereby that they have no competing interests.
Funding: Corresponding author supplied all study materials. There was no further funding for this study.
Authors' contributions: The authors completed the study protocol and were the primary organizers of data collection and the manuscript's draft and revision process. Tamer A. Addissouky wrote the article and ensured its accuracy. All authors contributed to the discussion, assisted in designing the study and protocol and engaged in critical discussions of the draft manuscript.
The authors thank all the researchers, editors, reviewers, and the supported universities that have done great efforts on their studies. Moreover, we are grateful to the editors, reviewers, and reader of this journal.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
