
Case Report | DOI: https://doi.org/10.31579/2641-0419/481
Department of Cardiac Anesthesia, Medanta-The Medicity, Gurgaon (Haryana)-122001, India.
*Corresponding Author: Ajmer Singh, Department of Cardiac Anesthesia, Medanta-The Medicity, Gurgaon (Haryana)-122001, India.
Citation: Ajmer Singh, Preeti, Ravina Mukati, (2025), Embolization of Pulmonary Artery Catheter Balloon: A Rare Complication, J Clinical Cardiology and Cardiovascular Interventions, 8(8); DOI: 10.31579/2641-0419/481
Copyright: © 2025, Ajmer Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 May 2025 | Accepted: 05 June 2025 | Published: 10 June 2025
Keywords: pulmonary artery catheter balloon; embolization; transesophageal echocardiography; cardiac surgery
Pulmonary artery catheterization is commonly used during cardiac surgery to monitor hemodynamic parameters. However, this procedure carries many risks and complications that may arise from its insertion or manipulation, its presence in the cardiovascular system, or misinterpretation of the data derived from it. Recently, we encountered a rare case of embolization of the pulmonary artery catheter balloon, which was detected using intraoperative transesophageal echocardiography. The balloon was surgically retrieved, and the patient made an uneventful recovery.
A pulmonary artery catheter (PAC) is often used during cardiac surgery to monitor hemodynamic parameters that are not reliably or continuously assessable by non-invasive or less invasive methods. Despite its benefits, the use of PAC is associated with several inherent risks and complications due to its invasive nature. Potential complications can arise from (i) central venous puncture, such as arterial puncture, hematoma, pneumothorax; (ii) insertion and manipulation of PAC potentially leading to arrhythmias, catheter knotting, catheter entanglement with cardiovascular structures; (iii) the presence of PAC in the cardiovascular system which may cause thrombosis, venous embolism, pulmonary artery (PA) rupture/perforation/infarction; (iv) infection; and (v) misinterpretation of the data derived from the PAC. [1] Rupture of the PA is particularly severe complication reported in approximately 0.03%-0.2% of patients. [2] This may occur due to overinflation of the balloon, improper balloon inflation, or improper position of the PAC.
Repeated inflation of the balloon can create cracks, leading to its rupture. Damage to the balloon can also occur from a mismatched introducer sheath or repeated re-insertion maneuvers. Although rupture and embolization of the balloon are rare, they pose significant risks. An embolized balloon can travel through the bloodstream into the PA or farther, potentially resulting in complications such as PA rupture, pseudoaneurysm formation, and pulmonary hemorrhage. This report describes a case in which the PAC balloon embolized into the PA and was successfully retrieved surgically.
A 48-year-old man presented with worsening dyspnea and palpitations and was admitted for evaluation. Transthoracic echocardiography indicated severe mitral stenosis, moderate mitral regurgitation, and mild tricuspid regurgitation. The patient underwent mitral valve replacement surgery. After the induction of general anesthesia, a transesophageal echocardiography (TEE) probe was inserted, confirming the preoperative findings (Fig.1). The right internal jugular vein was cannulated for the insertion of an introducer sheath and PAC by a skilled anesthesiologist. The integrity of all ports and the inflation and deflation of the PAC balloon (Edwards Lifesciences LLC, CA, Irvine, USA) were confirmed before insertion (Fig. 2A, 2B).
Utilizing pressure monitoring and waveform analysis, a 7.5F PAC was inserted through an 8.5F introducer sheath. After obtaining the right atrial pressure waveform at a depth of 20 cm, the balloon was inflated with a 1.5-ml syringe. However, the right ventricular pressure waveform could not be obtained until a depth of 30 cm. The balloon was deflated, and the PAC was retracted to 20 cm. During the second attempt to insert the PAC, the balloon failed to inflate, indicating a loss of resistance consistent with balloon rupture. Upon withdrawing the PAC from the sheath, it was noted that while the catheter remained intact, the balloon was notably missing (Fig. 2C). At this point, rupture of the balloon and its migration into the circulatory system were suspected. An immediate TEE evaluation showed the ruptured balloon floating in the main PA, just distal to the pulmonary valve.
Following sternotomy, the initiation of cardiopulmonary bypass, and cold cardioplegic arrest, the embolized balloon was retrieved from the main PA through a vertical incision. The planned surgical procedure continued without complication, and the postoperative course was unremarkable.
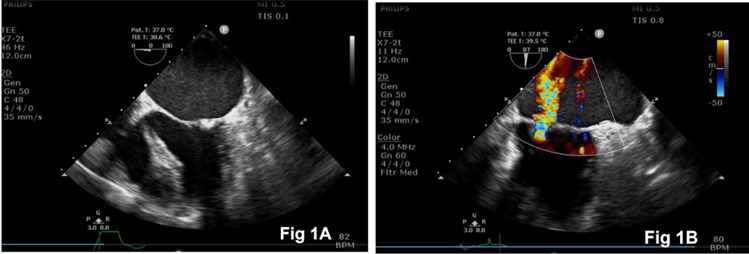
Figure 1: Intraoperative transesophageal echocardiography images showing mitral stenosis (Fig. 1A) and mitral regurgitation (Fig. 1B).
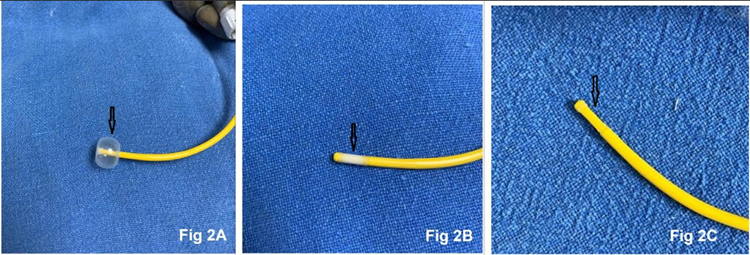
Figure 2: Photographs of the pulmonary artery catheter, arrows representing inflated balloon (Fig. 2A), deflated balloon (Fig. 2B), and missing (embolized) balloon (Fig. 2C).
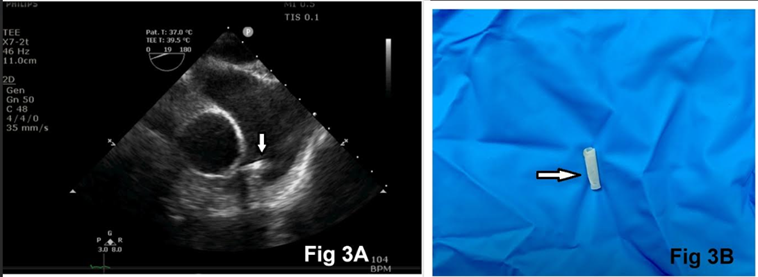
Figure 3: Transesophageal echocardiography ascending aorta short-axis view showing embolized balloon in the main pulmonary artery (arrow), just distal to the pulmonary valve (Figure. 3A). Surgically retrieved balloon of the pulmonary artery catheter (arrow, Figure. 3B).
Rupture and embolization of the PAC balloon are extremely rare but serious complications. Possible mechanisms for balloon rupture include: (i) repeated inflation leading to cracks, (ii) the use of high pressure/high volume over a prolonged duration, (iii) the use of nitrous oxide during anesthesia resulting in increased balloon diameter, (iv) repeated re-insertion maneuvers, and (v) mismatched introducer sheaths. Rupture can occur due to structural failures of the catheter or complications arising during or after catheter placement. In severe cases, balloon fragments can separate from the catheter and travel through the circulatory system, which poses significant risks that cannot be underestimated. We advocate for heightened awareness and vigilance regarding these complications in order to safeguard patient outcomes.
A similar case of a balloon separated from the PAC during an attempted removal through the introducer sheath has been reported by Helena et al. [4] However, they found the intact balloon inside the introducer sheath, and it did not embolize. Passage through a size mismatched introducer sheath, as well as repeated PAC re-insertions, can also cause balloon damage. The breaking and embolization of a catheter fragment into the pulmonary vascular system are rare and, in most cases, benign. However, Racionera et al have described severe pulmonary hypertension due to embolization of PAC fragments into the right PA. [5] The fragments disappeared with the movements of the fragment along with the flow of blood to the lung periphery. Balloon rupture followed by embolization and migration to PA can also occur during percutaneous transluminal angioplasty of the arteriovenous fistula. The preferred method for removal of a ruptured balloon during angioplasty is endovascular retrieval using additional distal access and a gooseneck snare. [6] Sometimes, surgical removal is required because attempts at removal using the endovascular technique adversely affect patient safety and result in vessel injury.
The embolized balloon or its fragments can lodge in a blood vessel, potentially causing serious complications like thrombosis, myocardial injury, arrhythmias, or perforation of a blood vessel. The embolization of the balloon into the PA can lead to rupture of the PA, pseudoaneurysm formation, and pulmonary hemorrhage. Depending upon the severity of PA rupture, the patient may experience hemoptysis, chest pain, or dyspnea. Pulmonary angiography or computed tomography of the PA (CTPA) is the gold standard for diagnosing PA rupture and pseudoaneurysm. Pulmonary angiography and CTPA can also be used to detect the position of the embolized balloon or its fragments, if they move far distally and are not visible during surgery. If a catheter fragment embolizes, it needs to be retrieved to prevent further complications, often through procedures like percutaneous extraction or surgery.
In conclusion, PA catheter balloon rupture and embolization is a serious complication that requires prompt diagnosis and treatment to prevent potentially life-threatening outcomes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
