
Research Article | DOI: https://doi.org/10.31579/2692-9759/078
1 Mount Sinai Morningside and Mount Sinai West – New York.
2 Rutgers New Jersey Medical School – New Jersey.
3 Hackensack Meridian Palisades Medical Center – New Jersey.
4 New Jersey Institute of Technology – New Jersey.
5 University Hospital – New Jersey.
6 Hadassah Hebrew University Medical Center – Israel.
*Corresponding Author: Emad F. Aziz, Department of Cardiology, Rutgers New Jersey Medical School, 185 South Orange Avenue, MSB I 530 Newark, NJ 07103.
Citation: Markovic N., Hossain A., Viswanathan R., Hanna M., Emad F. Aziz, et al. (2022). Elevation Of Cardiac Troponin After Implantable Cardioverter- Defibrillator Firing as Marker of Worse Short- And Long-Term Outcome in Patients with Chronic Heart Failure. Cardiology Research and Reports. 4(6); DOI:10.31579/2692-9759/078
Copyright: © 2022 Emad F. Aziz, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 November 2022 | Accepted: 09 November 2022 | Published: 29 November 2022
Keywords: heart failure outcome; troponin leak; ICD therapy; ICD shocks
Background/Aim: The consequences of electrical discharge over the myocardium in patients with implantable cardioverter-defibrillator (ICD) are continuously debated and its implications are controversial. Cardiac troponin I (cTnI) elevations have been reported to occur after electrical discharges, however, the relation between cTnI elevation after ICD firing and patients’ mortality is still to be established. We aim to evaluate short- and long-term outcomes of chronic heart failure patients with elevated cTnI levels after ICD discharge to establish its utility as a prognostic factor.
Materials and Methods: This is a retrospective observational study comprised of 155 patients (mean (SD) age 61± 15 years, 45 women) who were admitted to our institution after receiving spontaneous ICD shocks during the preceding 24 hours. cTnI was measured between 12 and 24 hours after ICD discharge. The relationship between cTnI levels and all-cause mortality at 30-day, 6-month, one year and fiver year intervals were assessed in both univariate and multivariate analyses.
Results: During a median follow-up period of 66 months, 38 (24%) patients died. Patients with a post-discharge cTnI level of >0.12 ng/ml had worse survival than those with cTnI <0.12 ng/ml. Using adjusted Cox Hazard multivariable analysis for older age, history of diabetes, decompensated heart failure and hypertension, post-ICD firing elevation in cTnI levels remained the most significant predictor of mortality (p-value 0.001).
Conclusions: Elevation of cTnI levels after ICD discharges in patient with chronic heart failure is a significant risk factor for higher mortality that is independent of other common clinical factors that predict survival in such patients.
Implantable Cardioverter Defibrillators (ICDs) have become the standard of care for patients at increased risk of having potentially life-threatening ventricular arrhythmias leading to sudden cardiac death [1-3]. Currently around 6.7 million people suffer from heart failure in the United States [4]. About 50% of patients with heart failure die from sudden cardiac death (SCD) [5]. Since 2002, the guidelines of the American College of Cardiology (ACC) and the American Heart Association (AHA) recommend that patients with left ventricular ejection fraction of less than or equal to 30%, at least one-month post-myocardial infarction and three months post-coronary revascularization are indicated for prophylactic ICD therapy [6]. Accordingly, the number of patients implanted with ICDs has increased substantially over the past decade. However, despite the well-known benefits of ICD therapy in the appropriate settings, concerns about implications of ICD shocks in terms of morbidity, mortality and discomfort for patients remains [7]. Infrequently, patients receive multiple shocks over a short period of time, commonly termed electric storm, which, even if appropriate as an attempt to terminate a malignant ventricular arrhythmia [8], can be distressing especially in the setting of an acute coronary syndrome [9].
Various studies have investigated the impact of cardiac bio-marker elevation after ICD firing [9-10,24,25]. Earlier, a couple of studies reported no effect on mortality [7,8,10] but did report higher readmission rate8. Recent data suggests an increased mortality in acute decompensated heart failure patients (ADHF) patients who undergo repetitive ICD firing, along with decreased quality of life and psychological changes [10–13]. The electric current delivered during an ICD firing is thought to cause mechanical, electrocardiographic [14], conductive [15] and biochemical changes at the myocardial cellular level, sometimes leading to myocardial necrosis [16]. Prospective studies of troponin (cTnI) assays have demonstrated that cTnI has higher diagnostic accuracy to predict myocardial injury and worse clinical outcomes as compared to other cardiac bio-markers [17,18,26]. Thus, determination of any analogy between elevation of the cTnI post-ICD firing and an effect on mortality in chronic heart failure (CHF) patients is an area of continued interest as the implications of cTnI elevation after ICD firings in CHF patients are not well identified.
Few studies were conducted analyzing the elevation of cardiac enzymes and echocardiographic trends following spontaneous or induced ICD firing. Nevertheless, they were sternly limited either due to a small sample size or without specified targeted population [9,19,20]. Owing to the scarcity of the data regarding all-cause mortality in CHF patients receiving ICD firing, we aimed to determine the significance of elevated troponin levels and the survival probability of the patients who presented with ICD discharges. We also sought to evaluate if troponin elevations predict adverse outcomes after ICD firing in CHF patients to ascertain their clinical significance in outcomes of patients with CHF.
Patient selection
The study was approved by Internal Review Board and Ethics Committee of our hospital, a community-based university affiliated teaching hospital. This is a retrospective observational analysis comprised of 155 CHF patients who presented to the emergency department (ED) after receiving spontaneous ICD discharges between the years 2006 and 2009 and were admitted to our institution. All of the patients underwent interrogation of the devices to determine if a shock was delivered. The interrogation included event counters, number of shocks delivered, total energy delivered (in joules), and analysis of stored intracardiac electrograms to ascertain the appropriateness of shocks. All patients in whom a shock was delivered by the ICD were included in the study, regardless of being appropriate or inappropriate shock.
Data Acquisition:
This is a retrospective analysis of data extracted from a prospectively collected database. Data was collected via retrospective chart review of demographics, presenting symptoms, cardiac history, medications, laboratory work up, electrocardiographic findings (EKG), number of ICD shocks, and concomitant comorbidities and entered into a SPSS database (SPSS for Windows, version 17; SPSS; Chicago, IL) by certified ICD clinicians familiar with database design, input, and management.
Study Definitions and Parameters:
Appropriate shocks: Shocks were called appropriate when stored EGMs met the programmed criteria of Ventricular tachycardia (VT) or ventricular fibrillation (VF) detection. The EGM criteria for the diagnosis of VT included changes in the number and polarity of the QRS deflections during the tachycardia compared with that during the baseline rhythm. VF was characterized by the presence of fibrillatory R waves at a rate of more than 200 beats per minute on the EGM and termination by defibrillation. An electrophysiologist analyzed stored EKGs for all episodes of ventricular arrhythmias resulting in shock therapy were placed in the chart of each patient.
Inappropriate shocks: Inappropriate ICD shocks were segregated as sinus or atrial tachycardia, atrial flutter (AFl) or atrial fibrillation (AF) with accelerated ventricular rates, and ICD shock therapy coupled with an EGM failing to exhibit morphologic criteria for VT or VF.
Laboratory measures:
Blood samples for serum chemistry, brain natriuretic peptide (BNP), serum creatinine levels, creatinine kinase levels (CK) and cTnI were collected on admission in patients presenting with complaint of ICD firing. Blood samples were drawn from a peripheral vein into tubes and centrifuged at 2,500 rpm at 4°C. All patients had three serial measurements of serum cTnI levels at baseline, and 8 hours and 16 hours after admission. The first measurement was done within 24 hours of the first shock. Measurements were performed and interpreted by individuals blinded for clinical data. Serum cTnI was measured using the TROP method, which is a highly sensitive and specific colorimetric enzyme immunoassay that measures cTnI levels quantitatively in serum. The TROP method utilizes two monoclonal antibodies specific for two different epitopes on the cTnI molecule. The diagnostic cutoff value for positive cTnI at our institution is defined as ≥ 0.12 ng/mL.
Patients Follow-up
All patients following post-ICD firing admission were prospectively followed-up by using physician-directed scripted telephone interview. Cardiac events were confirmed by review of medical records, death certificates and/or the social security death index. Patients or relatives were interviewed at least twice during the follow-up period for up to 66 months to assess symptoms.
Endpoint of the study
The study endpoint was all-cause mortality in patients with CHF during the follow-up period. Mortality and date of death were assessed by a comprehensive search of the Social Security Death Registry, last accessed July 2010 and adjudicated entries into the database.
Statistical analysis performed using a standard statistical software package (SPSS for Windows, version 17; SPSS; Chicago, IL). Continuous variables are presented as mean with standard deviation (SD), whereas categorical variables are presented as absolute numbers and percentages. The distributions of continuous variables were tested for normality and compared using a student’s t-test. Categorical variables were compared using the χ2 or Fisher's exact test where appropriate. Cox regression analysis was performed to assess association between cTnI levels on admission and all-cause mortality, and to control for potential confounders including age, sex, and number of shocks. The relative effects are presented as hazard ratios (HR) with 95% confidence intervals (95% CI). For all-cause mortality, we performed the log-rank test and estimated event-time distributions between the patients with elevated cTnI levels on admission and those without, using the Kaplan–Meier method. All tests were two tailed, and p values less than 0.05 were considered statistically significant (figure 1).

Figure 1: Kaplan-Meier Survival Curve: Heart failure patients admitted with elevated troponin post-ICD shock carry worse outcome when compared to those who did not have significant troponin elevation
Baseline characteristics of the study participants (n = 155) of CHF patients presenting to the ED from 2006 to 2009 who randomly received ICD shocks are shown in Table 1. Patients were stratified into two groups based on the TnI levels as group with cTnI level of < 0 xss=removed> 0.12 ng/ml (n=57) with mean age of 62 ± 15 years. Baseline demographics, prior cardiac history, other laboratory markers, symptomatology and medical therapy were not statistically different among the two groups (Table 1).
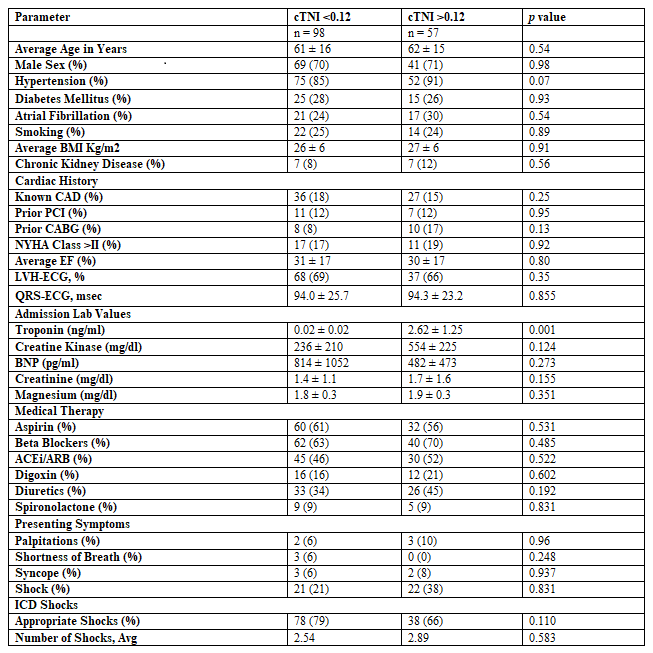
Table 1: Baseline characteristics of the patients
Inclusion criterion was patients older than 18 years with ischemic and non-ischemic cardiomyopathy who experienced an ICD discharge. cTnI was measured between 12 and 24 h after ICD discharge. Patients who did not meet any of the above criteria were excluded.
The time from first shock to admission ranged from 1 to 24 hours; the mean time from first shock was 8.9 & 9.4 hours. ICD shocks were preceded or accompanied by symptoms in 13 patients. This included palpitations in 5, dizziness in 7, syncope in 5, shortness of breath in 3, and sensation of electric shock in 43 patients. None of the patients required advanced cardiac life
support or external cardioversion. Ninety-two percent of the patients were in acute decompensated heart failure clinically, which was supported with an elevated BNP level of 648 ± 763 pg/dl.
Outcomes evaluated at 30 days, 6 months, one year and 5 years included acute myocardial infarction, stroke, all-cause mortality and total events. Sixty-eight percent of total events occurred in the group with elevated troponin as compared to 56% total events in group with cTnI level of < 0>p = 0.002) as shown in Table 2.
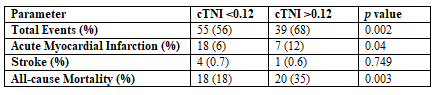
Table 2: Clinical Events at 5 Year Follow-up
All-cause mortality was significantly higher (35%) in group with cTnI level of > 0.12 ng/ml as compared to 18% in group with cTnI level of < 0>p = 0.003). Troponin elevation was found to be the second most significant predictor of the mortality in the adjusted multivariable analysis (HR = 2.6, CI: 1.24-5.24, p = 0.001) after decompensated heart failure (HR = 4.2, CI 1.84-9.80, p = 0.0007) as shown in Table 3.
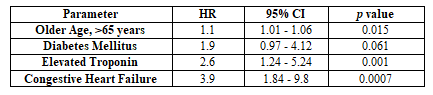
Table 3: Multivariable Logistic Regression Predictors of Mortality (p less than 0.0005)
There was a strong trend for elevated cTnI levels to correlate to the number of shocks; however, this did not quite reach statistical significance (Table 1). Most of the patients in this study received greater than 2 ICD shocks within a 24-hour period, which does not comply with the definition of “electrical storm.” Comparison of the patients who received less than and more than 3 shocks showed that the patients with more than 3 shocks were more likely to have elevated cTnI levels and inappropriate shocks than the patients who received less than 3 shocks (Table 1). Of note, the time from the first shock to when the first cTnI level was drawn was not different between the two groups. Similarly, ejection fraction and the total amount of energy used were not significant.
Our study demonstrates that cTnI elevation post-ICD discharges is associated with higher mortality in CHF patients, which suggest occult myocardial injury after these ICD shocks. In fact, 37% of the patients admitted for evaluation of multiple ICD shocks were found to have elevated cTnI levels. The MADIT –II (Multicenter Automatic Defibrillator Implantation Trial-II) study reported worse outcomes in patients receiving ICD shocks, demonstrating a three-fold increase in mortality in those receiving appropriate shock and a two-fold higher mortality in those with an inappropriate one [21,22]. Similar results were obtained from SCD-HeFT (Sudden Cardiac Death in Heart Failure Trial) data where patients receiving an appropriate shock had a five-fold increase in risk of death versus a two-fold increase in those receiving an inappropriate shock. When all these patients were combined risk of death was increased by a factor off 1111.
We found that only 23% of the patients with ICDs had underlying coronary artery disease and 18% of patients demonstrated acute coronary syndrome. In other words, elevated cTnI levels can occur following ICD shocks in the absence of coronary artery disease or acute coronary syndrome. In our patients with coronary artery disease and elevated cTnI levels, acute myocardial infarction was observed in 12% of patients’ post-ICD firing. This is consistent with results from previous studies that acute ischemia can be a triggering factor in patients with recurrent ventricular arrhythmias [7]., although the possibility that the ICD shocks precipitated acute coronary syndrome cannot be excluded. An accurate diagnosis of myocardial infarction in the context of ICD firing is essential, since it has important prognostic and treatment implications.
It has been demonstrated that patients with ventricular arrhythmias secondary to myocardial infarction in association with heart failure have a higher hospital mortality rate than patients with acute myocardial infarction without ventricular arrhythmias, but the one year mortality rate was reported to be no different [23]. Contrastingly, our study demonstrated a higher five-year mortality risk in patients with CHF and ICD firing in the setting of a myocardial infarction. In our study, mean ejection fraction of the patients was lower (30.5% ± 17%). To the best of our knowledge, this is the first study demonstrating how patients with low ejection fraction respond to ICD shocks with regards to the cTnI elevations and its eventual effect on the five-year survival of these patients.
A recent study that evaluated 26 patients with multiple spontaneous ICD shocks observed a positive correlation between troponin I and number of shocks [24]. Patients with troponin I elevation after multiple ICD shocks had higher risk of death or heart failure hospitalization compared with the group without elevation of this biomarker. The authors concluded that a majority of patients with multiple ICD shocks will have troponin I elevation as well as a higher risk of death or hospitalization due to heart failure. Our study reinforces these findings, with a far bigger patient population and longer-term follow-up.
Results from the Altitude Study showed that the patients who received ICD shocks for ventricular rhythms and atrial fibrillation showed an increased risk of death after an ICD implantation [23]. This study prompted us to investigate the causal relationships between this relationship of higher mortality in patient with ICDs and shocks. Our study demonstrated that the patients who received that ICD shocks as compared to the ones who did not receive any, have a higher mortality. Similarly, post-PCI elevation of cardiac biomarkers especially troponin elevation has been shown to be associated with worst outcomes in many recent trials [25]. Our study provides evidence that ICD shocks have an inverse relationship with survival benefit in CHF patients. While we cannot conclude whether elevated cTnI levels and higher mortality in CHF patients post-ICD firing was due to direct consequence of myocardial damage caused by shocks or secondary to the progression of heart failure itself, either of these two mechanisms may potentially play a role.
Determination of the exact cause of cTnI elevation is clinically and therapeutically important but not always straightforward. More importantly, our study demonstrated that in addition to the diagnostic role of cTnI, the extent to which cTnI levels are elevated potentially has a prognostic significance in patients with chronic heart failure, i.e., the higher the cTnI post-ICD discharge, the higher the mortality. Even though we could not differentiate between appropriate and inappropriate ICD shocks, we summarize that cTnI elevation after any spontaneous ICD shock is an independent predictor of higher long-term mortality in patients with CHF. However, as will be discussed shortly, there are limitations in the collection and interpretation of this data.
It is not possible to exclude the possibility that some of the troponin rises were due to acute ischemia (that was subclinical or did not meet the definition of acute coronary syndrome used in this study). In addition, our study endpoint was overall mortality in patients with elevated troponins after ICD shocks which limited our ability to discriminate between appropriate and inappropriate shocks, which could further help classify different populations at risk. Other clinical conditions that could cause troponin elevation like myocarditis, pericarditis, sepsis and severe GI bleeding were not excluded.
We conclude that troponin elevation in CHF patients presenting with ICD discharge is a strong predictor of higher mortality that is independent from other clinical factors. These patients need a more aggressive management during hospitalization as well as close monitoring after discharge given this higher mortality rate.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
