
Research Article | DOI: https://doi.org/10.31579/2641-0419/083
1Central Cardiology Medical Center, Bakersfield, CA.
2Touro University California, Vallejo, CA.
3Central Cardiology Medical Center, Cedars-Sinai, College of Osteopathic Medicine, Touro University California, Vallejo, CA.
*Corresponding Author: Singh Sarabjeet, Central Cardiology Medical Center, 2901 Sillect Avenue Suite 100, Bakersfield, CA 93308, USA
Citation: Sahoo Alor, Strong Laura, Jensen Alexander, Flaherty Daniel, Anand Mukul, Alromheen Hassan, Singh, Sarabjeet (2020) Elevated Lipoprotein (a) in Cardiac Outcomes: A Review. J. Clinical Cardiology and Cardiovascular Interventions, 3(9); Doi:10.31579/2641-0419/083
Copyright: © 2020 Singh Sarabjeet, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 September 2020 | Accepted: 25 September 2020 | Published: 01 October 2020
Keywords: lipoprotein(a); cardiac outcomes; cholesterol; coronary artery disease; cardiac risk
Context
Elevated lipoprotein (a) [Lp(a)] levels is an often-ignored risk factor for major adverse cardiac events (MACEs) in humans. Even after accounting for established risk factors (discussed in the text), some residual risk can still be independently attributed to elevated Lp(a) levels.
Current guidelines dictating normal and elevated Lp(a) levels and subsequent treatment have proven haphazard due to unstandardized studies. Many studies offer cutoff values in units mg/dL, which do not account for the heterogeneity of Lp(a). Interpretation of elevated Lp(a) necessitates consideration of ethnicity necessary for proper predictions. Numerous studies detail the effects of elevated Lp(a) in relation to myocardial infarction, aortic valve stenosis, and atherosclerosis, among other conditions. This article aims to clarify the numerous cutoffs and guidelines presented.
Methods
Searches were primarily conducted through Google, PubMed.gov, and cochrane.org.
Results
Elevated Lp(a) seems to correlate with the incidence of MACEs and should be considered when assessing risk. Specific cutoff values remain quite unclear.
Conclusions
We urge for further detailed investigation on the effects of elevated Lp(a) on cardiac outcomes with the use of isoform independent assays. Particular attention should be given to ethnicity when assigning risk cutoffs for cardiac conditions. Proprotein convertase subtilisin/kexin type 9 (PCSK-9) inhibitors can lower Lp(a) levels significantly and should be investigated.
According to the Center for Disease Control (CDC), within the United States (US), 18.2 million adults aged 20 or older have a form of coronary artery disease (CAD), which is a risk factor for other cardiac conditions.[1] Effective treatment can reduce the frequency of major adverse cardiac events (MACEs) in these high-risk individuals if identified early on. [2,3]
Elevated low-density lipoprotein cholesterol (LDL-C) levels, systemic hypertension, smoking, diabetes, and old age are the major, well-established risk factors of MACE in general. Nonetheless, a MACE can still occur even if some or all of these factors are controlled. [4] But the effects of lipoprotein (a) [Lp(a)] should not be neglected.
First described in 1963, Lp(a) is an LDL-like particle consisting of an apolipoprotein B100 (apoB100) covalently bonded to an apolipoprotein a [apo(a)] molecule, which exists in multiple “kringles” and contributes to the different Lp(a) isoforms. [5]
Some studies suggest that lipoprotein(a) [Lp(a)] plasma levels are independently correlated with MACE, which may explain this residual risk. [6] For example, one study found that the risk of acute myocardial infarction (MI) was higher in Chinese patients with normal LDL-C levels, but high Lp(a) levels. [7]
In some cases, Lp(a) does not appear to increase the risk of certain cardiac conditions but rather aggravate pre-existing conditions. For example, patients with existing aortic valve stenosis (AS) and elevated Lp(a) levels have a higher risk of mortality. [8]
It seems that apo(a) preferentially carries oxidized phospholipids (OPLs), which are highly atherogenic and hasten the disease progression of AS in these individuals.8 In addition to this, apo(a) appears to have anti-fibrinolytic and prothrombotic properties. [9]
Notably, serum levels of Lp(a) are relatively resistant to changes in diet, environment, and lipid-lowering agents. [10,11]
Methodology and Objective
This review aims to analyze current studies that look at the association between Lp(a) levels and MACEs independent of the previously mentioned established risk factors. Searches were conducted through the search engines Google, PubMed.gov, and cochrane.org. Websites of various journals, such as the New England Journal of Medicine, Journal of the American Heart Association, Arteriosclerosis, Thrombosis, and Vascular Biology, and Journal of the American College Cardiology, were also pursued.
While many studies have demonstrated a positive correlation between Lp(a) levels and MACE incidence, there has been controversial data in other studies.
For example, while a study in the Journal of the American College of Cardiology (JACC) found a positive correlation between elevated Lp(a) and MACE for people who already had CAD, the heterogeneity of the studies analyzed did not allow the authors to conclude that Lp(a) was a useful marker for risk assessment, especially in those with well-controlled LDL-C. [12]
Units of Measurement and Lack of Standardization
Though measurement of Lp(a) levels are usually given in mg/dL, this is not ideal. For example, a study in the Journal of the American Heart Association (JAHA) determined that an Lp(a) level of ≥30 mg/dL was considered “high,” while other studies determine an elevated Lp(a) level to be anywhere from ≥25 mg/dL to ≥65.2 mg/dL, making recommendations for people with these intermediate Lp(a) levels unclear. [13,14] In one systematic review in Lipids in Health and Disease, the authors noted that around half of the secondary prevention studies analyzed treated Lp(a) levels as categorical variables (such as low, medium, high,) further complicating risk assignment. [13]
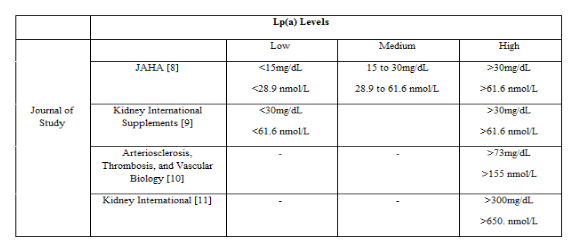
These types of cutoffs ignore the heterogeneity of apo(a) particles and are a bit arbitrary, as all apo(a) and Lp(a) particles do not weigh the same. [13,15] There is also no way to accurately convert the units of mg/dL into nmol/L, which measures the number of particles per volume and provides a better representation of Lp(a) concentration. [16] Unfortunately, some studies have continued to attempt to relate the two measurements, potentially obscuring results. A study in Arteriosclerosis, Thrombosis, and Vascular Biology (ATVAB) used the equation [Lp(a),nmol/L] = 2.18[Lp(a),mg/dL] − 3.83, where [Lp(a),nmol/L] was the serum Lp(a) level in units of nmol/L and [Lp(a),mg/L] was the serum Lp(a) level in units of mg/dL; such conversions can propagate misleading recommendations. [17] These converted values are included in Table 1 in red.
Studies in the past have been harmed by this lack of standardization. Initial results from a Physician Health Study showed that high levels of Lp(a) correlated with a higher risk of angina pectoris were later revised. [15] The initial study used enzyme-linked immunosorbent assays (ELISAs), which were sensitive to apo(a) size (i.e. isoform dependent), and the latter used nephelometry. [15] These types of measurements are unfortunately quite common: of the thirty-nine primary prevention studies studied in the systematic review in Lipids in Health and Disease, only twelve studies used isoform independent assays. [13] These assays can also overestimate Lp(a) levels in hypertriglyceridemic individuals. [15]
Other Issues in Handling Samples
In the systematic review previously mentioned, 34 of the 39 studies didn’t use fresh plasma samples when obtaining measurement; however, using frozen plasma is ill-advised for the most accurate measurements. [13] For example, a study in ATVAB found that Lp(a) plasma levels in samples frozen for between 3 to 28 months were around 4.83% lower than levels found in fresh samples. [18] This decrease is primarily caused by low-molecular-weight (LMW) apo(a) isoforms. Since people with atherothrombotic disease more frequently have these LMW apo(a) isoforms, studies using frozen plasma may find an unusually weak correlation between MACEs/ASCVD and Lp(a) levels. [19] This of course complicates the interpretation of studies involving Lp(a) that utilize frozen plasma.
Even when the proper types of measurements are taken, the prevalence of LMW isoforms may impact studies. The Choices for Healthy Outcomes in Caring for End Stage Renal Disease (CHOICE) study, which used an isoform independent Lp(a) assay, found that the association between having LMW isoforms and ASCVD was more robust than the association between Lp(a) levels of ≥52.5 nmol/L and ASCVD in patients on dialysis. [13,18]
All else held constant, the specific time of day at which the sample is taken does not seem to affect Lp(a) measurements significantly. A study in the journal Atherosclerosis found that the median fasting levels of Lp(a) were 17.3 mg/dL, while median levels at 3-4 hours after the last meal were 19.4 mg/dL. [20]
As detailed later, it is prudently advised that further studies be performed following the guidelines provided, as the heterogeneity in the MACE outcomes, populations, and statistical analysis methods means a proper meta-analysis has not been able to be conducted at this point. [13]
Results and Discussion
Challenges in Lowering Lp(a)
It is generally agreed that high Lp(a) levels are correlated with MACEs, though it is unclear whether this is a causal relationship. Some studies contradicted this and determined that Lp(a) had little impact on MACEs. An example of such a study is the Italian Longitudinal Study on Aging (ILSA), which initially found that there was no correlation between high Lp(a) levels and fatal–nonfatal coronary artery disease (CAD) events. [13,21] However, high Lp(a) levels were found to be an “independent and significant predictor” after six years in adults between the ages of 65 and 84 years. [13,21]
This increase in risk would not be as problematic if Lp(a) levels could be consistently lowered with no risk. However, this is not the case.
As stated previously, serum Lp(a) levels and “regular moderate exercise” show no correlation. [10,11] Some studies suggest that people who participate in “intense load-bearing exercise” even have increased Lp(a) levels, though these studies neglected to account for ethnic factors. [11]
Conventional treatments include numerous side effects. Niacin in the amounts needed to treat these dyslipidemia causes “transient, asymptomatic elevations in serum aminotransferase levels” in around ⅕ of people. [22] High doses of sustained-release (SR) niacin tend to cause jaundice and hepatic necrosis, which may be reversible. Some patients may also have underlying liver problems that contraindicate the use of this treatment. [22]
In addition to this, there may be other risks associated with low Lp(a) levels. A study in the Clinical Chemistry found an inverse relationship between Lp(a) and type 2 diabetes, independent of other risk factors. [23] It is not conclusively known whether or not this relationship is a causal one. [23]
Other treatments, such as proprotein convertase subtilisin/kexin type 9 (PCSK-9) inhibitors, have shown promise in reducing Lp(a) levels. [24] One such drug, inclisiran, has been especially useful in lowering Lp(a) by 17.2% from baseline in patients with heterozygous familial hypercholesterolemia who had already been treated with typical statins, according to a study in the New England Journal of Medicine. [25] Small interfering RNA drugs like inclisiran seem roughly as effective as monoclonal antibodies that target PCSK-9; however, inclisiran requires less frequent administrations, increasing the likelihood of patients to adhere to a treatment regimen. [24,25] Since roughly 1 in 250 persons have heterozygous familial hypercholesterolemia, further research into dosing and long-term viability should be considered. [25] This product is still investigational.
The Effect of Lp(a) on Other Cardiac Risk Standards
Coronary artery calcium (CAC) scores are consistently used to assess CAD risk, especially in asymptomatic individuals.26 A study in the Journal of the American Medical Association Cardiology (JAMA Cardiology) found that adults between the ages of 31 to 46 years who had non-zero calcium scores less than 19 had a 2.6-fold risk of having a MACE in the future than participants who had a score of zero. [27] Another study in the journal Nutrition, Metabolism & Cardiovascular Diseases found a positive association between Lp(a) levels >38.64 mg/dL CAC scores >0.28
Whether elevated Lp(a) contributes to increased risk of CAD independent of elevated CAC score is not decisively known. A study in the Journal of Clinical Lipidology found that for= individuals with a family history of ASCVD, elevated Lp(a) levels (defined as >50mg/dL) were associated with CAC scores >100.29 However, a study in JACC suggested that high Lp(a) and CAC>100 were independently associated with ASCVD risk.30 While no interaction between these variables was observed in this study, the existence of a joint association between elevated Lp(a) and CAC score with ASCVD is unclear and requires further research. [30]
One difference between these studies appears to be the resulting racial distribution from which subjects are chosen, as ethnicity seems to be an influential factor on the cardiac effects of Lp(a) in specific individuals. [31] One study in ATVAB noted that an Lp(a) cutoff of 50mg/dL might be more appropriate for Caucasians and Hispanics, while a cutoff of 30mg/dL is more appropriate for African American individuals in determining cardiac risk. [31]
As discussed before, the units mg/dL poorly describe Lp(a) risk, but is correct in that different cutoffs are needed for different racial groups. different cutoffs are needed for different racial groups.
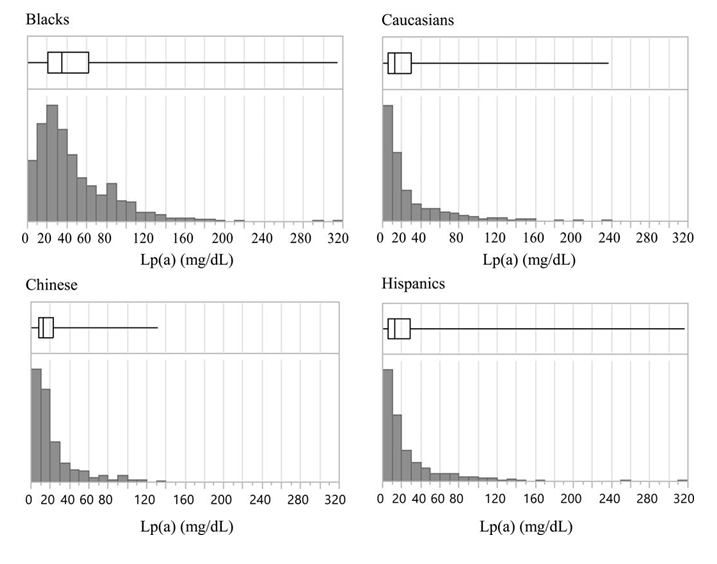
As seen in Figure 2, different ethnic groups, particularly African Americans, have different distributions of Lp(a) levels. For example, blacks have a more symmetrical distribution of Lp(a) levels than Caucasians, Chinese, and Hispanics, implying the need for more flexible cutoffs to determine risk.
High Lp(a) may not be correlated with an increased risk of various cardiac conditions in certain ethnicities. For example, high Lp(a) levels (in mg/dL) were found to be risk factors for calcific aortic valve disease in white and blacks, but not in Hispanics and Chinese-Americans. [32] High Lp(a) (in mg/dL) was a risk factor for peripheral artery disease in whites and Hispanics, but not Chinese-Americans or blacks. [33,34] Similarly, a study in ATVAB found that the “Lp(a)-related risk of carotid plaque” was higher in whites than blacks when measured (in mg/dL). [33]
There is a patent need for a study on Lp(a) that is isoform independent, accounts of LMW apo(a) isoforms, uses fresh plasma samples, and assigns multiple cutoffs for different ethnic groups. Current studies suffer from one or more of these problems. Lastly, as previously discussed, PCSK-9 inhibitors such as inclisiran show promise and should be further analyzed to identify potential contraindications and long-term effectiveness.
We would like to thank Dr. Sarabjeet Singh, the corresponding author, for his assistance in editing the manuscript. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
