
Case Report | DOI: https://doi.org/10.31579/2690-4861/507
1UOC of Oncology, Sant'Andrea University Hospital – Rome, Italy.
*Corresponding Author: Eva Mazzotti, UOC of Oncology, Sant'Andrea University Hospital – Rome, Italy.
Citation: Monia Specchia, Eva Mazzotti, Federica Mazzuc, (2024), Electrochemotherapy to Treat a Single Thoracic Metastasis in Patient with Breast Cancer., International Journal of Clinical Case Reports and Reviews, 19(1); DOI:10.31579/2690-4861/507
Copyright: © 2024, Eva Mazzotti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 August 2024 | Accepted: 26 August 2024 | Published: 02 October 2024
Keywords: elettrochemotherapy; breast cancer; loco-regional procedure; electropulsation; clinoporator; case report
Electrochemotherapy represents one of the therapeutic breakthroughs in the oncology field. In this case report, we describe a woman diagnosed with breast cancer in 2005. The case was treated surgically with right breast mastectomy, with axillary dissection for estrogen receptor positive ductal carcinoma, followed by a course of chemotherapy. Radiotherapy and hormonal adjuvant therapy with aromatase inhibitor were used for 8 years and the treatment plan was completed in 2014.
After 17 years from the surgery, a thoracic Hight Resolution Computed Tomography scan showed a single node localized in right intercostal space, treated with a loco-regional treatment without complications. This allowed us to make the patient disease-free again.
This case opens a choice in a loco-regional treatment to offer at a patient a new chance.
Breast cancer is the most common tumour in women and the leading cause of death from cancer in women worldwide [1,2]. The prevalence of long-term survivors increased and therefore also the risk of late breast cancer recurrence gets higher [3,4].
The most common metastatic target sites are 60% of metastatic breast cancer patients have lung or bone metastasis in their life [5,6].
Oligometastatic breast cancer is characterized by a limited number and sites of metastasis, it may have a definitive remission with individualized treatment and multidisciplinary management [7,8]. Standard treatments for oligometastatic breast cancer include local treatments (surgery and radiotherapy); systemic therapies according to histological type (chemotherapy, endocrine therapy, and immunotherapy) are generally avoided [9,10]. Due to lack of randomized trials and the heterogeneity of breast cancer biology, treatment options for patients with oligometastatic breast cancer are different [9,10].
Electrochemotherapy (ECT) is an option in this setting based on preclinical and clinical studies [11]. ECT combines electropulsation of tumour cells, by local application of electric pulses, and administration of antineoplastic drugs such as cisplatin or bleomycin, either intravenous or intratumoral. Several clinical studies have demonstrated that ECT provides safety and efficacy in non-invasive locoregional treatment for chest wall breast cancer recurrence [12].
We are describing herein the case of a postmenopausal patient with an history of HER2 positive breast cancer who presented a single thoracic node after 17 years of clinical and instrumental exams during follow up.
A 65-year-old Caucasian woman in good clinical conditions presented during a visit programmed in follow up a thoracic pain in the high right intercostal space.
The patient was diagnosed with breast cancer in 2005 and treated surgically with right breast mastectomy, with axillary dissection for estrogen receptor positive (ER) ductal carcinoma, followed by adjuvant radiotherapy and chemotherapy.
Immunohistochemical results highlighted PgR positive, Ki 50%, HER2 FISH amplified, stage III.
After surgery patient was treated with adjuvant chemotherapy with Epirubicine and Cyclophosphamide (EC) for 4 cycles followed by Paclitaxel and Trastuzumab weekly for 12 cycles and subsequently subcutaneous administration of Trastuzumab alone every three weeks for 1 year of treatment. She received radiotherapy and hormonal adjuvant therapy with aromatase inhibitor for 8 years. Treatment was completed in 2014.
Patient underwent to regular follow up visits, laboratory tests and imaging exams every six months.
Seventeen years after surgery, in November 2021, patient reported outbreak of thoracic pain in the last right intercostal spaces.
Total body Computer Tomography (TbCT) scan was negative for bone and visceral metastasis. Breast ultrasound and mammography were also negative to signs of local relapse. She started a generic anti-inflammatory therapy without benefit. Followed by specific treatment with Gabapentin assuming late chemotherapy-induced neuropathy, with minimal response in pain relief.
One month later patient underwent to thoracic Hight Resolution Computed Tomography (HRCT) scan that showed a single node localized in right intercostal space (Figure 1).
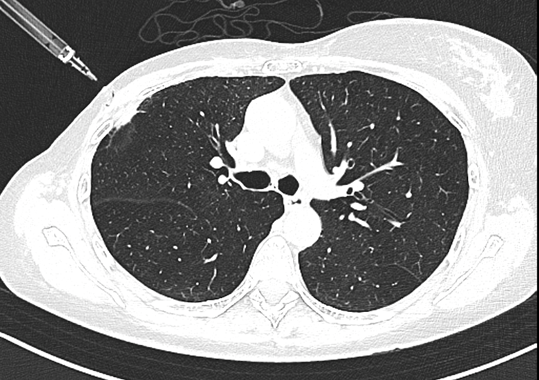
Figure 1: Thoracic Hight Resolution Computed Tomography image.
A single node localized in right intercostal space is detected (December, 2021).
Positron emission tomography (PET/CT) with fluorodeoxyglucose (FDG) confirmed the presence of a single metastatic lesion in right costal space that received contrast.
Three different treatment proposals have been made: superior right lobectomy was the surgeon suggested treatment, single stereotaxic short court radiotherapy, and ECT treatment.
For ECT there were not contraindications, patient was in good general condition, ECOG performance status scale was 0, she had not known significant comorbidities she did not use any drugs. Thoracic nodule was single, stellar shape, adjacent to the coast, it was not impossible to be reached with electrode.
Multidisciplinary team discussion was performed and radiotherapy, surgery and ECT were the options suggested by the clinicians.
Patient refused radiotherapy because she experienced toxicity. She experimented a sever cutaneous toxicity during adjuvant treatment of
breast cancer after surgery and she rejected this possibility. Surgery with pulmonary lobectomy is also refused by the patient as pulmonary lobectomy is a burdensome surgical treatment associated with long post-operative rehabilitation and a decrease in lung function. ECT was the choice treatment.
One day before the treatment physical examination, laboratory tests (blood count, coagulation, renal and hepatic functionality) and cardiologic evaluation were carried out. A written informed consent to the ECT and to the publication of the study results were obtained. Treatment was performed under general anesthesia (deep sedation with Propofol) with standard hemodynamic monitoring.
This procedure was conducted in the presence of a multidisciplinary team constituted by oncologist, interventional radiology, anesthetist and specialized nurse. Procedure was performed under CT scan guide. The Cliniporator EPS-02 produced by IGEA was adopted (Figures 2 and 3).

Figure 2 Electrochemotherapy procedure.
Preparation for ECT procedure.

Figure 3: Electrochemotherapy procedure.
The electrodes’ introduction.
According to European Standard Operating Procedures on Electrochemotherapy (ESOPE) guidelines, ECT was performed with bleomycin intralesional. Three electrodes were introduced in intercostal space with CT scan imaging guide. International units (IU) of bleomycin were introduced in the lesion. After the intralesional chemotherapy administration three electrodes were introduced and needles extruded to penetrate the whole lesion so that the electric field could cover the entire volume of it. The entire procedure lasted 20 minutes, and a sample of the lesion was taken for histological confirmation. The patient was hospitalized for 2 days receiving antibiotic prophylaxis with cephalosporins.Procedure was well tolerated, without side effects. The histological examination confirmed the presence of single Metastasis originating from the previous carcinoma of the breast.Thoracic HRTC was performed one day after ECT treatment and no signs of lung damage were found. Thoracic HRTC performed one month after the procedure showed downstaging of the lesions (Figure 4).
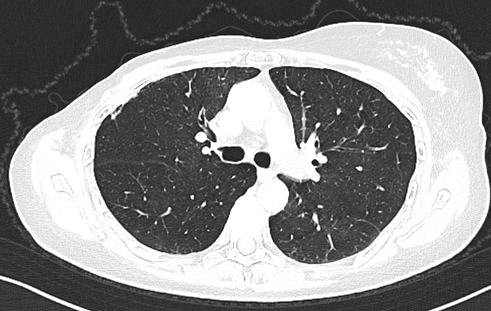
Figure 4: Thoracic Hight Resolution Computed Tomography (HRCT) image.
Lesion necrotic pattern (January, 2022).
Subsequent instrumental chest examinations first highlighted the necrotic pattern of the lesion and then the complete resolution of the case (Figures 5 and 6).

Figure 5: Thoracic Hight Resolution Computed Tomography (HRCT) image.
Lesion necrotic pattern (September, 2022).
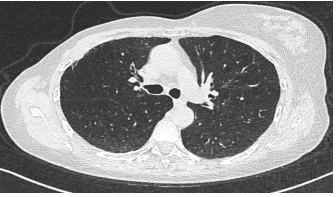
Figure 6: Thoracic Hight Resolution Computed Tomography (HRCT) image.
Lesion resolution (February, 2023).
Three months after, a Thoracic Hight Resolution Computed Tomography (HRCT) showed an additional downstaging of the treated lesion (Figure 7).
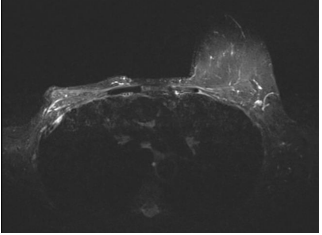
Figure 7: Thoracic Hight Resolution Computed Tomography image.
Additional downstaging of the treated lesion (April, 2023)Patient remain in good clinical condition, she did not report pain, skin was clear, there were no signs of injury. Currently (2024), at clinical and instrumental checks, she is negative for disease recurrence.
Electrochemotherapy is a valid alternative treatment to conventional locoregional treatment especially when patient have a single or multiple cutaneous lesions.
Different molecular subtypes of breast cancer have different behaviors in the sites of distant metastases: Hormone Receptor (HR)+ HER2+ breast cancer subtypes have a major risk of bone metastases, HR– HER2+ subtypes are frequently associated to brain and liver metastasis, lung metastasis is common in all cancer subtypes [13]. The incidence of oligometastatic disease has increased, and the correct definition of the treatment options must be recommended by specialized centers, to allow an improvement in the patient’s quality of life and an increase in overall survival. Radiotherapy and surgery are the most common treatment options for oligometastatic breast cancer. Stereotactic body radiotherapy (SBRT), image-guided radiotherapy (IGRT), radiosurgery are different new types of radiotherapy emerged as potentially curative treatment [7]. Surgery is a good option, but its role is unclear in isolated thoracic metastases from breast cancer [14].
More recently ECT has emerged as an option for the treatment of oligometastatic cancer. It is a local ablative treatment based on reversible electroporation: it combines administration of antineoplastic drug (systemically of locally) with locally applied electric pulses that allow chemotherapy drugs to penetrate in the cell and have a cytotoxic effect [15]. ECT determine high response rate with few side effects.
ECT role is undiscussed in the treatment of cutaneous and subcutaneous lesions, in melanoma and, more recently, ECT treatment in deep tumors has been reported with promising results [11,16], although randomized clinical trials are lacking.
Its greatest advantage is that it is effective in areas previously treated by surgery and radiotherapy and can be used in patients already undergoing chemotherapy without causing systemic toxicity.
Another aspect to highlight is the immediate improvement of the psychological burden of the patient with the complete resolution of the painful symptoms almost immediately.
The peculiarity of this case report is the use of electrochemotherapy in variable geometry with intralesional bleomycin in the only thoracic metastasis from breast cancer.
This case report confirms the excellent local disease control achieved with electrochemotherapy and highlights the need for a multidisciplinary discussion to define the best treatment to propose to a patient who has already undergone multiple treatments such as surgery and radiotherapy.
Acknowledgement
We are grateful to the patient for accepting the idea of publishing this clinical case with the diagnostic images.
None
None
Obtained
Substantial contributions to the conception of the work (FM, MS, EM); Acquisition, analysis, interpretation of data (FM, MS, EM); Drafting the work and revising it critically for important intellectual content (FM, MS, EM); Final approval of the version to be published (FM, MS, EM); Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (FM, MS, EM).
Yes, if requested
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
