
Research Article | DOI: https://doi.org/10.31579/2641-0419/257
1 Bayelsa Specialist Hospital, Yenagoa.
2 University of Port Harcourt Teaching Hospital, Port Harcourt.
*Corresponding Author: Edafe Emmanuel Auchi, University of Port Harcourt Teaching Hospital, Port Harcourt.
Citation: Abd Rabou Hamed, Ahmed Elkersh, Ahmed Hegab. (2022). Electrocardiography Diagnostic Performance in the Assessment of Significant Coronary Artery Disease and its Anatomical site in Comparison with Coronary Angiography among Nigerians: A Pilot Study. J. Clinical Cardiology and Cardiovascular Interventions, 5(4); Doi:10.31579/2641-0419/257
Copyright: © 2022 Edafe Emmanuel Auchi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 March 2022 | Accepted: 21 March 2022 | Published: 29 March 2022
Keywords: coronary arterial dominance; percutaneous coronary artery intervention; hospital stay; follow up
Background: Coronary vessel dominance, defined by the coronary artery that supplies the posterior descending artery (PDA) and posterolateral branches, influences the relative contribution of the different coronary arteries to the total left ventricular blood flow. This work aimed to evaluate the prognostic value of coronary arterial dominance post primary PCI, during hospital stay and at 3-month follow-up, which include; cardiac mortality, heart failure, non-fatal myocardial infarction, re-vascularization, stroke/TIA and re-admission for ACS.
Methods: This prospective observational study included 100 patients a with STEMI who underwent successful primary percutaneous coronary intervention with TIMI III flow and without procedural complications. Patients were divided into 3 groups according to coronary dominance: Right coronary dominant group (RCD), left coronary dominant group (LCD) and balanced coronary dominant group (BCD). All patients were subjected to transthoracic echocardiogram and coronary angiography and Primary percutaneous coronary intervention.
Results: Ticagrelor and clopidogrel during hospital stay and on hospital discharge were significantly used more with RCA group than LCX group and LCX & RCA group (P=0.021, 0.012), (P=0.018, 0.014), respectively. GPIIB/IIIA was significantly more used during hospital stay with RCA group than LCX group and LCX & RCA group(P=0.014). Nitrates was significantly used more on hospital discharge with RCA group than LCX group and LCX & RCA group (P<0.001).
Conclusions: Coronary arterial domi¬nance showed significant prognostic value in cases of myocardial Infarction after PCI, heart failure in LCX cases and in revascularization, heart failure, and stroke/TIA cases in RCA. Further, readmission for ACS was the most common outcome in all groups after 3-months follow-up.
Early diagnosis of coronary artery disease is mainly based on some risk stratification approaches. This includes medical history, physical examination, electrocardiogram and serum cardiac marker measurements. [1,2] The diagnosis requires a careful review of cardiac ischemia manifestations. Coronary artery disease (CAD) is a life-threatening condition that necessitates rapid decision-making. [1,2]
Coronary angiography (CAG) is a useful diagnostic tool in patients with suspected CAD especially in patients that are at high risk. [4,5,6] CAG is the gold standard for diagnosis of significant coronary stenosis. However, it can be associated with certain risks.[6]
The use of noninvasive assessment tools for predicting CAD is considered because it offers safety, patient convenience, and faster performance. The aim of the study was to assess the predictive value of 12-lead electrocardiogram (ECG) in patients with suspected coronary artery disease (CAD).[1]
Methods
Patients between 40 and 98 years of age who presented with new onset chest pain were recruited. They all had standard 12 lead electrocardiogram done. The ECG changes were interpreted by the two Cardiologists.
The ECG was recorded as normal or abnormal depending on:
Regional changes in ST segment (ischemic-appearing ST depression or elevation)
T-wave inversion (≥ 1 mm) and Q-wave appearance (≥ 0.04 s or ≥ 25% of R-wave.
On admission, a resting standard 12-lead ECG was recorded and the ECG changes were interpreted by the cardiologist. The ECG was recorded as normal or abnormal depending on regional changes in ST segment. The ECG was recorded as normal or abnormal depending on regional changes in ST segment (ischemic-appearing ST depression or elevation), T-wave inversion (≥ 1 mm) and Q-wave appearance (≥ 0.04 s or ≥ 25% of R-wave).
The III, aVF and II leads were used to detect RCA involvement; V5, V6, lead 1 and aVL to detect LCx involvement, and V1, V2 or V3, and V4 were used to detect LAD involvement. ECGs were taken at a paper speed of 25 mm/s and calibration of 10 mm. All enrolled participants had coronary angiography using the femoral artery. Patients with a stenosis ≥ 50% diameter, were classified as having significant CAD.
We excluded patients with other severe concomitant diseases and patients previous bypass surgery. Also excluded are those with positive troponin and chronic kidney disease. Ethical approval was obtained from the hospital. An informed consent was also obtained from all participants. Approval was given by the ethical committee of the hospital and informed consents were obtained from all participants.
Quantitative data was presented as Mean ± standard deviations or percentages. Descriptive statistics including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of ECG in determining significant coronary artery stenosis were calculated. Predictive values of ECG between the two genders were compared using chi-square test. Statistical analyses for these parameters were performed by an independent statistician, using SPSS version 25 (SPSS Inc., Chicago, IL, USA).
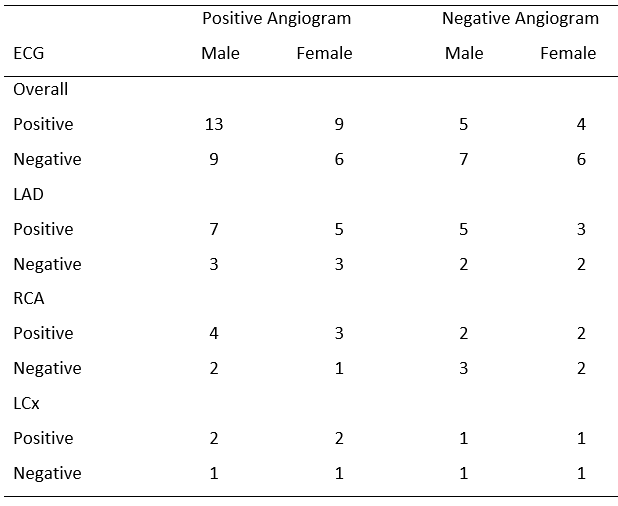
A total of 59 patients were recruited for the study over a 12-month period. The mean age is 61.2 ± 14. Of the coronary angiography reports, 37 out of 59 participants had significant coronary artery stenosis, with a prevalence of significant CAD was 62.7%. The coronary angiography did not detect significant stenosis in 22 of the patients (37.3%). ECG correctly detected significant stenosis in 21 patients out of the 59. It brings the overall sensitivity per patient was 64.9% and specificity of 68.2%. [see Tables 1, 2 and 3]
ECG correctly detected significant stenosis in 21 out of 59 patients. The overall sensitivity per patient was 59.5% and specificity of 59.1%. [Table 2] ECG Sensitivity and specificity for LAD (60.0% and 40.0% respectively) [Table 2]. ECG sensitivity and specificity for RCA (63.6% and 62.5% respectively) [Table 2]. ECG sensitivity and specificity for LCx (66.7% and 50.0% respectively) [Table 2]. Over ECG positive predictive value is 71.0% [probability of indicating coronary vessel disease in persons with the disease]. Over ECG negative predictive value is 46.4% [probability of negative findings that is less likely to indicate the absence of disease] [see Table 2].
Predictive power of electrocardiogram for the diagnosis of coronary artery disease comparison with coronary angiogram in men and women is shown in Table 3. There is no difference in the ECG capability in the diagnosis of coronary artery disease among men and women as there is no statistically difference in sensitivity and specificity with p-values of 1.000 and 0.866 respectively. See Table 3.
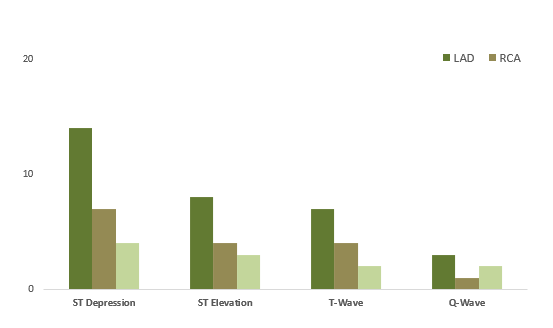
The figure 1 showed the distribution of ST segment, T-wave and Q-wave changes. ST-segment changes are more with Left Anterior Descending Artery [LAD], followed with Right Coronary Artery [RCA] and then the Left Circumference artery [LCx]. Q-wave changes are more with LAD, followed with LCx and then RCA. [ see Figure 1].
Keywords: RCA, right coronary artery; LCx, left circumference; ECG, electrocardiogram.
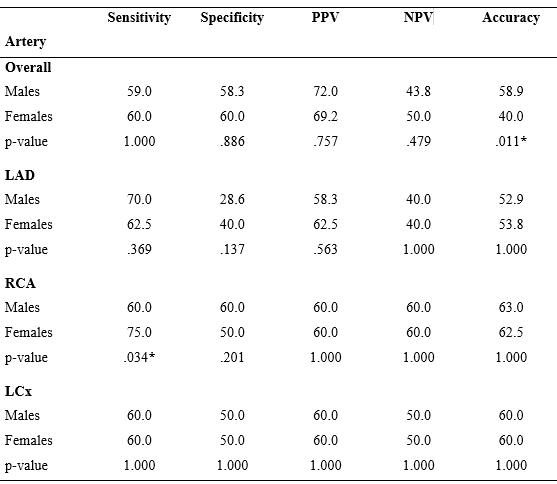
Key: PPV, positive predictive value; NPV, negative predictive value; RCA, right coronary artery; LCx, left circumference; ECG, electrocardiogram; LAD, left anterior descending artery.
LAD, left anterior descending artery; LCx, left circumference artery; RCA, right coronary artery
12 lead ECG has been known as an important routine part of the assessment of patient presenting with chest pain.[7] electrocardiography is an integral part of patient evaluation for suspected coronary artery disease.[1] Among the patients with chest pain, the prompt and accurate detection of acute coronary syndrome remains an important clinical challenge for specialists.[7]. This is what the pilot study showed. First, our study showed that electrocardiography is safe, non-invasive and easily available tool to be used in the emergency room in detecting patients with chest pain suspected coronary artery.
There are studies that focused on cost-beneficial aspect and feasibility of this tool, and on its prognostic and predictive values. [8, 9,10, 11] Our study showed that electrocardiography is valuable in the emergency room. Mahmoodzadeh et al in a study of electrocardiography, correctly detected significant stenosis in 176 out of 400 patients with an overall sensitivity per patient of 51.5% and specificity per patient of 66.1%. [12] Of the 59 patients in the present study, the sensitivity and specificity are 59.5% and 59.1% respectively. The current study had similar sensitivity and specificity even when our study had fewer number of patients.
Somani and his colleagues in a study of correlation of electrocardiography Changes with Coronary Angiographic Findings in Patients of Coronary Artery Disease, involved 200 participants. Their study showed a sensitivity and specificity of electrocardiography to diagnose myocardial infarction or ischemia ranged from 87.50% to 96.63% and 91.30% to 95.45%, respectively.[13] Their study also showed diagnostic accuracy of electrocardiography to detect myocardial infarction or ischemia, ranged from 89.36% to 96.40%. these findings were higher than the present study. The possible reasons could be due to race difference, and the prevalence of the disease from the former study.
Based on the present findings, each electrocardiography parameters independently could poorly predict coronary artery disease with very low sensitivity. But, when considered together, predictive power was significantly increased. Similarly, Holubkov and colleagues showed that using at least two electrocardiography parameters in any set of contiguous leads cause notable higher odds of significant angiographic coronary artery disease than those without concomitant ECG parameters changes. [14] furthermore, the judgment about the presence of coronary artery disease should be performed on the sum of electrocardiography parameters findings.
Electrocardiography has been well known as an attractive method for patients’ risk stratification. [15] Recent studies found that the changes in electrocardiography parameters such as ST-segment depression and T-wave inversion could effectively predict long term mortality and morbidity of patients with acute coronary syndrome and also those who undergoing cardiac revascularization.15, 16] Despite poor value of electrocardiography to predict appearance of sudden cardiac attack, it may be potentially useful for predicting late outcome of cardiac diseases in comparison with invasive strategies that should be strongly considered.
ECG is useful in risk stratification of patients with CAD. It is valuable in the diagnosis of CAD especially in resource poor settings.
This is a pilot study with small sample size.
The management of Bayelsa Specialist Hospital for the cooperation during the data collection. The patients who gave informed consent for their information to be used in research work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
