
Research Article | DOI: https://doi.org/10.31579/2690-4861/1137
1Associate professor of Pediatric hematology oncology department, Hakim children hospital, Tehran University of Medical Science, Tehran, Iran.
2Associate professor of cardiology, Lorestan University of Medical Science, Khoramabad, Iran.
3Assistant professor of Pediatric cardiology department, Hakim children hospital
*Corresponding Author: Babak Abdolkarimi., Associate professor of Pediatric hematology oncology department, Hakim children hospital, Tehran University of Medical Science, Tehran, Iran.
Citation: Babak Abdolkarimi, Arash Amin, Amir Banazadeh, Niki Panahi, (2026), Efficacy of Transarterial Chemoembolization (Tace) And Intra-Arterial Chemotherapy (Iac) in Pediatric Inoperable Tumors in Iran, International Journal of Clinical Case Reports and Reviews, 36(4); DOI:10.31579/2690-4861/1137
Copyright: © 2026, Babak Abdolkarimi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 June 2026 | Accepted: 10 July 2026 | Published: 13 July 2026
Keywords: neuroblastoma; transarterial chemoembolization; intra-arterial chemotherapy; pediatric oncology; inoperable tumor
Background: Management of inoperable tumors in pediatric patients remains a clinical challenge. Transarterial chemoembolization (TACE) and intra-arterial chemotherapy (IAC) have emerged as targeted approaches to reduce tumor size and facilitate surgical resection.
Methods: Five pediatric patients with inoperable neuroblastoma, aged 2–5 years, underwent a total of 16 TACE and IAC sessions. Each patient received an average of three treatment sessions. The primary outcome was the feasibility of complete tumor resection after therapy.
Results: All patients achieved complete tumor resection following the intervention. One patient died due to tumor progression, unrelated to the procedure. No major procedure-related complications were reported.
Conclusion: TACE and IAC are effective and safe methods for reducing tumor burden and enabling surgical resection in children with inoperable tumors. These findings support the use of targeted intra-arterial therapies in specialized pediatric centers.
Inoperable tumors in pediatric patients, particularly neuroblastoma, pose significant treatment challenges. Traditional systemic chemotherapy may be limited due to toxicity and inadequate tumor targeting. These tumors typically encase large, vital vessels such as the aorta, renal arteries, or paravertebral vessels. TACE and IAC offer targeted delivery of chemotherapeutic agents directly to tumor vasculature via the tumor-feeding artery, which allows for complete delivery without metabolic elimination by the liver and kidneys, while also occluding the tumor-feeding artery at the end of the delivery process, resulting in tumor necrosis. This potentially increases efficacy while minimizing systemic side effects. These techniques can reduce tumor volume, improve the possibility of complete surgical resection, and potentially improve patient outcomes.
Study Design and Participants
This descriptive case series was conducted at a tertiary pediatric oncology center in Iran. Five pediatric patients diagnosed with inoperable neuroblastoma, aged 2 to 5 years, were included. Inclusion criteria were: (1) confirmed diagnosis of neuroblastoma via histopathology and imaging, (2) tumor deemed inoperable by a CT angiography of the abdominal and pelvic vessels and reconstruction of the vascular images of the camping procedure and finding the feeding arteries of the tumor, (3) no prior intra-arterial therapy, and (4) adequate organ function to tolerate interventional procedures. Exclusion criteria included severe comorbidities contraindicating anesthesia or vascular interventions.
Pre-Procedural Evaluation
All patients underwent comprehensive pre-procedural assessment, including complete blood count, liver and renal function tests, coagulation profile, and detailed imaging studies (CT angiography and 3D-reconstruction of the vascular images) to evaluate tumor size, vascularity, and relationship to surrounding structures. Cardiac evaluation was performed to ensure the safety of anesthetic procedures and chemotherapeutic agents.
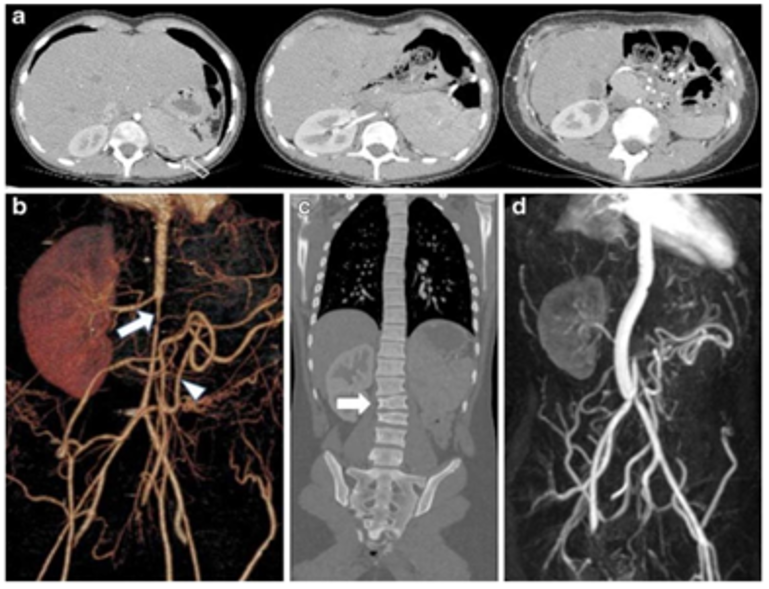
Imaging studies of a girl with stage IV neuroblastoma who developed hypertension and abdominal pain 7 years after tumor surgery, chemotherapy and IORT. a, b Axial contrast-enhanced CT angiograms (a) and 3-D reconstruction (b) show an extremely narrowed infrarenal aorta (arrow), as well as absent celiac, superior mesenteric and left renal arteries. The left kidney is not visible due to marked atrophy (a open arrow). Multiple abdominal collateral vessels
Sedation and Pediatric Considerations
Procedures were performed under sedation with Ketamin (1mg/kg) and Midazolam (0.1 mg/kg) and Atropin (0.01 mg/kg) with continuous monitoring of vital signs. Pediatric anesthesiologists ensured airway protection, hemodynamic stability, and appropriate dosing of analgesic and sedative-hypnotic agents according to body weight and age. Intra- procedural pediatric nursing support was provided to monitor oxygenation, heart rate, and blood pressure continuously.
Transarterial Chemoembolization (TACE) Procedure
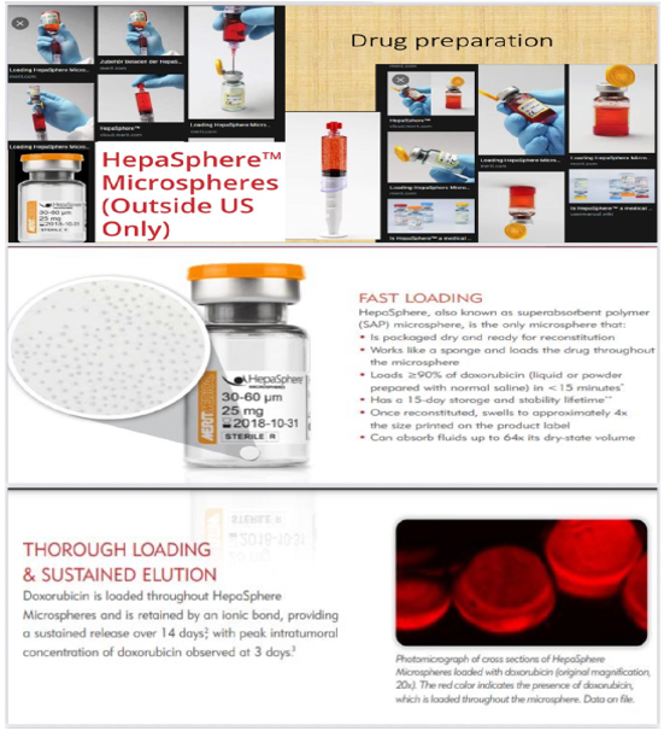
TACE was performed by interventional cardiologist experienced in pediatric procedures. A femoral arterial approach was used in all patients. Under fluoroscopic guidance, a microcatheter was advanced selectively into tumor-feeding arteries. Chemotherapeutic agents, including doxorubicin or cisplatin (dual therapy) or triple therapy (doxorubicin or cisplatin, Avastin) combined with Hepa Sphere™ (It is a thoroughly examined embolic material/loadable device available in four different sizes. In vitro experiments, animal studies and clinical trials, give insight on its mechanics and pharmacokinetics.) were infused directly into the tumor vasculature, followed by embolic particles to achieve vascular occlusion. Care was taken to minimize ischemic injury to surrounding normal tissues.
Intra-Arterial Chemotherapy (IAC) Procedure
IAC involved selective infusion of chemotherapeutic agents directly into the feeding tumor artery without embolization. Drug dosage was calculated based on patient body surface area, age, and renal function. (in our patients drug dosages were 10 mg for Cisplatin and Doxorubicin) Continuous fluoroscopic monitoring ensured correct catheter placement and avoided non-target perfusion.
Treatment Schedule and Follow-Up
Each patient received an average of three sessions (range: 2–4), with intervals of 3–8 weeks between procedures to allow recovery and assessment of tumor response. Tumor response was monitored through serial imaging studies such as ultrasonography or CT angiography and clinical evaluation. The primary endpoint was the feasibility of complete tumor resection by Release of abdominal and pelvic vessels encased by tumor following the intra-arterial therapy course. Secondary endpoints included procedure-related complications, tolerance of therapy, and overall clinical outcomes.
Safety and Adverse Event Monitoring
Special attention was given to potential pediatric-specific complications, including vascular injury, post-embolization syndrome, infection, and hematologic toxicity. Patients were closely monitored during and after the procedure (prepheral pulses in lower limb or neurologic signs) in a pediatric intensive care or step-down unit as needed. Analgesics and antiemetics and antibiotic were administered according to pediatric dosing guidelines.
Ethical Considerations
The study protocol was approved by the institutional ethics committee. Written informed consent was obtained from all parents or legal guardians. All procedures adhered to international guidelines for pediatric interventional oncology, emphasizing patient safety and minimizing procedural risk.
Patient Characteristics
A total of five pediatric patients (three males and two females) with inoperable neuroblastoma were included in this study. The mean age at diagnosis was 3.6 ± 1.1 years (range: 2–5 years). All patients presented with large abdominal masses and had previously received systemic chemotherapy before being deemed inoperable by a multidisciplinary tumor board.
| Summary of outcomes | Results |
| Total patients | 5 |
| Total procedures | 16 |
| Mean sessions per patient | 3.2 |
| Complete tumor resection | 5.5(100%) |
| Mortality (unrelated procedure) | 1.5(20%) |
| Long term disease free survival (12 months) | 4.5(80%) |
| Sex(male/female) | 3/2 |
| Age range | 2-5 years |
| Tumor location | Abdominopelvic in a majority of cases |
| histology | Neuroblastoma (unfavorable) |
| Disease stage | III-IV (INSS classification) |
Table 1: summarizes the baseline characteristics of the patients.
Procedural Data
A total of 16 intra-arterial procedures were performed, with an average of 3.2 sessions per patient (range: 2–4). All procedures were successfully completed without intraoperative technical complications such as arterial spasm, dissection, or non-target embolization.
In four patients, transarterial chemoembolization (TACE) was the main technique, while one patient received intra-arterial chemotherapy (IAC) alone due to vascular anatomy unsuitable for embolization.
The mean duration of each procedure was 85 ± 20 minutes, and the average hospital stay per session was 2.4 days.
Tumor Response
All five patients showed a significant reduction in tumor size after the TACE/IAC cycles. The mean tumor volume reduction was 58% (range 45–70%), as measured by MRI using volumetric analysis after the final session.
Following the intra-arterial treatment course:
Tolerability and Safety
All procedures were well tolerated. The most common post-procedural symptoms were low-grade fever and transient abdominal pain, consistent with post-embolization syndrome.
No major complications such as vascular injury, liver failure, or renal toxicity were observed.
Adverse events (according to CTCAE v5.0):
All patients recovered within 3–5 days after each session.
Laboratory and Imaging Findings
Follow-up
All patients were followed for a median of 14 months (range 10–18 months).
At the end of follow-up:
No patient developed delayed vascular or organ complications attributable to the procedures.
The present study demonstrates that transarterial chemotherapy (TACE) and intraarterial chemotherapy (IAC) are effective treatment modalities for pediatric patients with inoperable neuroblastoma. In all five patients, these targeted therapies allowed for complete tumor resection, highlighting their potential as neoadjuvant interventions in high-risk pediatric tumors. Our findings are consistent with previous reports that suggest that local intraarterial chemotherapy can increase tumor drug concentrations while minimizing systemic toxicity compared with conventional intravenous chemotherapy. This is particularly beneficial in pediatric patients, who are more susceptible to the side effects of systemic chemotherapy due to their developing organs and tissues. By delivering chemotherapeutic agents directly into the tumor vasculature, TACE and IAC can increase tumor necrosis, reduce tumor size, and improve surgical resection. Various drugs have been used in this procedure in different studies, including melphalan and topotecan. The mortality observed in one patient was attributed to tumor progression rather than procedural complications, suggesting that the procedures themselves are relatively safe when performed in specialized centers. This low complication rate is consistent with other studies of pediatric TACE and IAC and reinforces the appropriateness of these interventions for children with complex or high-risk tumors. Although our study is limited by the small sample size and lack of a control group, the complete tumor resection in all cases provides strong initial evidence for the efficacy of intra-arterial therapies. Of course, our study patients were patients who had not received an adequate response to classical surgery and systemic intravenous chemotherapy in different centers in Iran. Future studies with larger cohorts and long-term follow-up are needed to evaluate the survival outcomes, recurrence rates, and possible late complications of these interventions. In addition, careful patient selection remains crucial. Factors such as tumor vascularity, anatomical considerations, and overall patient health should guide the decision to use TACE or IAC. Interdisciplinary collaboration between pediatric oncologists, surgeons, and interventional radiologists or interventional cardiologists is essential to optimize outcomes and minimize risks. In conclusion, TACE and IAC offer promising strategies for the management of inoperable pediatric tumors, especially neuroblastoma. They have the potential to convert previously inoperable tumors into operable ones and improve overall prognosis while maintaining an acceptable safety profile. Ongoing research and multicenter studies are essential to establish standardized protocols and confirm the long-term benefits of these targeted therapies in pediatric oncology.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
