
Research Article | DOI: https://doi.org/10.31579/2690-8816/119
1 Speech Language Pathologist & Clinical Coordinator, 1 special Place
2 Ph D Scholar, Manial Academy of Higher Education, Manipal, India
3 Assistant Professor in Language Pathology, Department of Speech Language Pathology AIISH Mysore
*Corresponding Author: Abhishek BP, Assistant Professor in Language Pathology, AIISH, Mysore.
Citation: Ayesha Anjum, Haritha Mohan and Abhishek BP., (2024), Efficacy of Telerehabilitation in speech-language therapy for Traumatic Brain Injury: A case study, J Clinical Research Notes, 5(1); DOI:10.31579/2690-8816/119
Copyright: © 2024, Abhishek BP. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 November 2023 | Accepted: 20 December 2023 | Published: 02 January 2024
Keywords: telerehabilitation; traumatic brain injury; speech therapy; aphasia
Background Telerehabilitation in speech-language therapy has gained traction in the recent years in India; for delivering speech-language assessment and evaluation services. This study aims to evaluate the feasibility and efficacy of Telerehabilitation in speech-language therapy for a person with TBI.
Method: A longitudinal treatment case study was carried out for an adult participant with traumatic brain injury; undergoing tele-speech-language therapy. The scores of several standardized assessment tests and treatment goals were evaluated and reported at regular intervals during the treatment process to document progress of the client in the tele-speech-language therapy sessions.
Results and Discussion: The results revealed a trend of consistent improvement across sessions in all the domains considered for telerehabilitation. Marked improvement in the participant’s performance was noted by the decrease in error percentage and increase in overall percentage of correct responses across linguistic and cognitive domains targeted for therapy. Improvements were noted in the performance across linguistic and cognitive goals targeted for treatment displays the efficacy of telerehabilitation in the present study.
Traumatic brain injury (TBI) is caused by a head injury that disrupts brain function. The damage can either be focal or diffuse [1]. TBI is the leading cause of neurological disorders among adults, and is a threat to public health systems. The annual incidence of Traumatic brain injury is estimated to be 27 to 69 million. Hence the prevalence rate can be stated as high to very high
The assessment and management of Traumatic Brain Injury is often a challenging task to Speech-Language Pathologists (SLPs). In India, the scenario is particularly challenging because of the large geographical area. Individuals with TBI often lack access to cognitive-communicative rehabilitation services due to several factors. Two major factors that contribute are mobility difficulties in individuals with TBI and unavailability of service providers. One potential solution to overcome this is to utilize the telecommunications technology for delivering clinical services. Telerehabilitation (TR) is defined as the remote delivery of rehabilitation and home health care services (Rehabilitation Engineering Research Center on Telerehabilitation, 2007). TR enables Speech-Language Pathologists to conduct assessment and management of individuals with communication disorders over geographical barriers. This enables persons with TBI to avail clinical services at their doorsteps through a personal computer or any device which supports information and communication technology (ICT).
Studies comparing outcomes of online and in-person assessment have found no significant difference between the two modes in individuals with aphasia [ 2]. Videoconferencing has found to be effective for assessment of cognition in persons with TBI [3]. Furthermore a study [4]. found that video teleconferencing was as effective as in-person supervision for their client with TBI.
Tele-assessment and Tele- intervention in persons with TBI have gained momentum in the Indian scenario recently. However, there is no published research on telerehabilitation of TBI in India. Owing to the rise in the incidence of Road Traffic Accidents (RTA) in India and the unavailability of service providers in rural locations, telepractice can serve as an excellent alternative. Telerehabilitation facilitates immediate use of time post TBI, consequently promoting treatment outcomes. Thus, the current study aimed to evaluate the feasibility and efficacy of Telerehabilitation in speech-language therapy for a person with TBI.
Participant selection
A right-handed person with Traumatic Brain Injury [19 years] was the participant for the current study. The participant was a successive bilingual with Hindi as the native language (L1) and English as the second language (L2). Premorbid, the participant was equally proficient in both the languages as reported by the caregivers. Participant had completed 10 years of formal education with English as the medium of instruction. The participant had a history of a Road Traffic Accident on 27th February 2021 resulting in a severe Traumatic Brain Injury (TBI). Results of the CT scan revealed left frontotemporo parietal contusion with cerebral edema. He exhibited motor and language impairment following the TBI. Eventually, through physiotherapeutic intervention, significant improvement was reported in his motor skills. However, caregivers reported deficits in communication skills as they had no access to speech and language therapy services post TBI. At the time of inclusion in the study, the participant was 8 months post-onset. An informed written consent was obtained from the participant for the purpose of this study.
Procedure
Stage I: Pre-treatment assessment
A conventional (virtual mode) tele-speech-language assessment was conducted by a speech language pathologist on 20th October 2021. As the participant presented with a majority of linguistic deficits, Western Aphasia Battery was administered. Table 1 shows details of the scores obtained by the participant on Western Aphasia Battery.
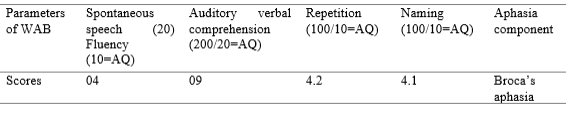
Table 1. Scores obtained on Western Aphasia Battery
The participant’s performance on the various sub sections of Western Aphasia Battery (presented features of Broca’s Aphasia. Further, to screen for cognitive deficits, Mini Mental Status Examination (MMSE) was administered. Performance of the participant is summarized in Table 2.
| Domains on MMSE | Scores obtained |
| Orientation | 10/10 |
| Registration | 1/3 |
| Attention and Calculation | 1/5 |
| Recall | 1/3 |
| Language and Praxis | 3/9 |
| Total score | 16/30 |
Table 2. Performance of the participant on Mini Mental Status Examination (MMSE)
As seen in Table 2 the participant showed deficits on several cognitive domains that are fundamental to fulfil any communicative act. Owing to the presence of language deficits and disturbed cognitive processes, the participant was diagnosed with cognitive-communication disorder post Traumatic Brain Injury.
Stage II: Treatment
The participant was recommended to avail tele speech and language intervention services. Telerehabilitation was suggested as the client had no access to speech and language intervention services at his end.
The speech language pathologist conducted sessions from an office equipped to deliver tele speech language and audiological services. The client availed telerehabilitation sessions from his home. It was ensured by the clinician and the caregiver that a quiet environment to be maintained during the tele-speech and language therapy sessions. Prerequisites followed to ensure effective communication during the therapy sessions included knowledge of computer operation by the participant and good manual dexterity. The technological infrastructure used to deliver telerehabilitation in the present study is summarized in Table 3.
| Sl.no | Technological infrastructure | Therapist Interface | Participant Interface |
| I | Hardware | ||
| Desktop computer | HP Compaq LE1902x, 18.5 inch monitor | Dell Inspiron 3647, 18.5 inch monitor
| |
| Headphones | CREATIVE HS150, on the ear, Supra-aural closed headset behind the ear design with built in microphone | Sony MDR-ZX110AP On-Ear Stereo Headphones with built in microphone
| |
| Webcam | Logitech Carl Zeiss Tessar HD 1080p | Logitech HD C270H 720p | |
| II | Software | Information and Communication Technologies (ICT) with screen sharing | |
| III | Network | 30 Mbps internet speed | 30 Mbps internet speed |
Table 3. Technological infrastructure for telerehabilitation
The duration of the tele speech and language therapy was twice a week, 1 hour per session for a period of 7 months. A total of 44 sessions were held till the date of generation of this report. The participant’s language proficiency was better in English post morbid; therefore, tele speech and language therapy was delivered in English (L2). Considering the outcome of the assessment carried out, the goals taken up for telerehabilitation of speech-language skills focussed on two domains, linguistic and cognitive functions.
a) Remediation of linguistic functions
The linguistic functions worked upon during intervention were spontaneous speech, repetition and naming based on the linguistic profiling. Therapy technique followed to facilitate spontaneous speech was Promoting Aphasics’ Communication Effectiveness (PACE) [5]. (PACE was followed as it incorporates components of a natural in-person conversational structure. The protocol for PACE involved natural interaction sequences in which the client and clinician alternated turns communicating the identity of the stimulus item depicted on Microsoft Office PowerPoint 2007. The target items included pictures of both nouns and verbs and targets were selected based on their frequency of occurrence in a natural conversation.
To remediate the participant’s naming difficulty, Phonological Component Analysis (PCA) [6]. therapy was followed. PCA focuses on generation and analysis of phonological features of targets words (i.e., rhyme first sound, first sound associate, final sound and number of syllables). The PCA enhances and strengthens the association between lexical semantics and phonological word form, thus allowing for correct production. The target stimuli consisted primarily pictures of nouns with high frequency of occurrence depicted on Microsoft Office PowerPoint 2019.
b) Remediation of cognitive processes
The cognitive processes worked upon were visual and auditory attention, memory and executive functions. Table 4 shows examples of the tasks carried out during the treatment sessions to remediate the cognitive deficits.
| Linguistic parameters | Tasks |
| Spontaneous speech | Situational picture description (E.g., Cookie theft picture), Role play / Dialogue (E.g., Conversation between a shop keeper and customer), Narration of a procedure / event in a sequence (Making coffee/ visit to friend’s home) |
| Repetition | Repetition of sentences with increasing length and complexity of utterance. |
| Naming | Confrontation naming (PCA), Generative naming, Word fluency naming, Co-ordinate naming and Super ordinate naming. |
| Cognitive processes | |
| Visual and auditory attention | Activities for improving sustained and divided attention (symbol cancellation, symbol trails, letter cancellation, sound count, letter pair discrimination, month backward counting and stroop tasks) |
| Memory | Verbal and non-verbal working memory tasks such as design memory, completing mazes, carrying out complex commands, syntactic and semantic judgement of sentences, spoken manipulation tasks (e.g., name for oral spelling, odd/ even number of letters in words). |
| Executive functions | Activities centred on linguistic planning and problem solving (sentence disambiguation, sentence formulation, predicting outcome, predicting cause, sequential analysis) and linguistic organization (categorization, analogies, sequencing events) |
Table 4. Tasks carried out during treatment sessions
The activities pertaining to each linguistic parameter and cognitive process followed a hierarchy i.e., gradually increasing the complexity of tasks
during the tele-sessions. The linguistic and cognitive goals were worked upon simultaneously. Responses were scored and recorded to account for the progress achieved by the participant during the treatment sessions. Generalisation for linguistic and cognitive goals were examined in between the treatment sessions (5th, 12th, 20th week) using untrained stimuli.
Scoring and analysis
Audio and video sample of the participant’s performance on all the goals in the 5th, 12th, 20th and 22nd week were analysed and the results were documented.
A quantitative analysis of the participant’s responses for spontaneous speech tasks was done. The number of paraphasic/ circumlocutory/ preservatory errors were calculated and expressed as a percentage of the total number of words spoken.
% Of errors = 
The scoring for each target item on PACE was adopted from the original 6-point rating scale proposed by Davis, 1980. The progress of the participant was charted by calculating the average performance for all the target items presented on 5th, 12th and 20th week.
The scoring carried out for repetition and naming tasks except for confrontation naming task was as follows; a score of 0 for no response/ incorrect response/ unintelligible response, 1 for correct/ intelligible response. Performance of the participant was calculated as follows,
% Of performance = 
The scoring for the participant’s performance on Phonological Component Analysis (PCA) therapy was as follows, a score of 5 for each target item was fixed by the clinician. For every stimulus item on PCA, the participant had to describe 5 parameters and each parameter was scored as 1 for correct response and 0 for incorrect/no response. The participant had to achieve a score of 3/5 on each target item in order to move on to the next stimulus item.
All the cognitive tasks were scored as 0 for no response/ incorrect response and 1 for correct response. Percentage of the participant’s performance on all the tasks in each sub section (attention, memory and executive functions) were averaged and calculated as follows,
% of performance = 
Stage III: Post-treatment assessment on Western Aphasia Battery (Kertesz and Poole, 1982) and Mini Mental Status Examination (Folstein and Mc Hugh, 1975) were done in the 22nd week.
The present study aimed to investigate the efficacy of providing tele-intervention speech-language therapy for an individual with Traumatic Brain Injury. The results are depicted in 1 to 5

Figure 1. Performance of participant on spontaneous speech and repetition.
The spontaneous speech task was scored and analysed based on percentage of errors.
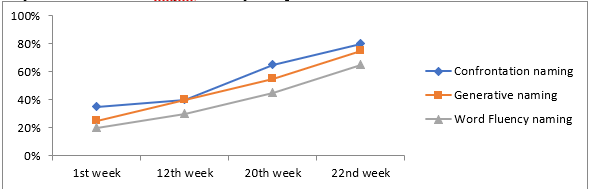
Figure 2. Performance of the participant on naming tasks such as confrontation naming, generative naming and word fluency naming tasks.
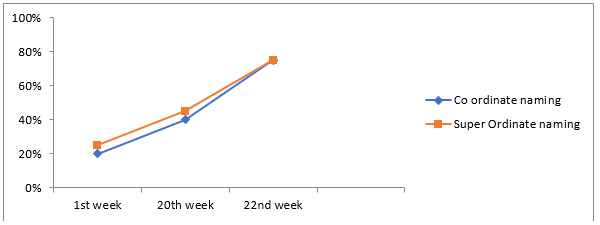
Figure 3: Performance of the participant on naming tasks such as co-ordinate naming and super-ordinate naming.
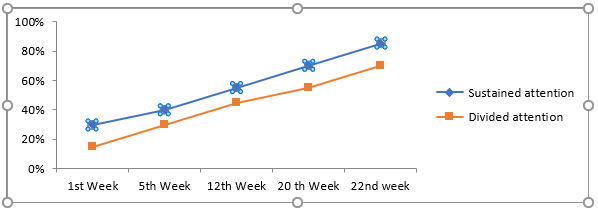
Figure 4. Performance of the participant on sustained and divided attention tasks.
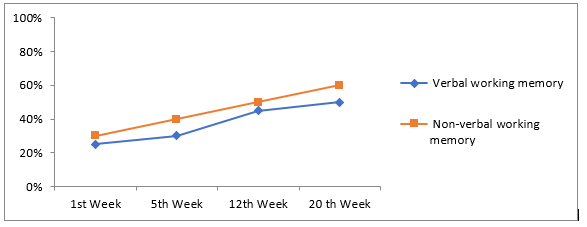
Figure 5. Performance of the participant on verbal and nonverbal working memory tasks.
The results revealed a trend of consistent improvement across sessions in all the domains. Marked improvement in the participant’s performance was noted by the decrease in error percentage and increase in overall percentage
of correct responses across linguistic and cognitive domains targeted for therapy. Post-treatment assessment was carried out through videoconferencing mode. Post-treatment assessment scores on Western Aphasia Battery.
| Parameters of WAB | Spontaneous speech (20) Fluency (10=AQ) | Auditory verbal comprehension (200/20=AQ) | Repetition (100/10=AQ) | Naming (100/10=AQ) | Aphasia component |
| Scores | 07 | 09 | 08 | 07 | Anomic aphasia |
Table 5: Post-treatment scores obtained on Western Aphasia Battery
As it is evident from the Table 3.2, the participant has shown significant clinical improvement in all the language domains targeted for treatment.
Further, it can be noted that the participant had shown considerable progress in the spontaneous speech domain post-treatment with PACE. The performance on the naming task has shown considerable improvements post-treatment with Phonological Component Analysis (PCA) therapy
To screen for post-treatment progress achieved in the cognitive domain Mini Mental Status Examination (MMSE) (was administered 23rd June 2022 are tabulated in Table 3.3.
| Domains on MMSE | Scores obtained |
| Orientation | 10/10 |
| Registration | 3/3 |
| Attention and Calculation | 4/5 |
| Recall | 2/3 |
| Language and Praxis | 8/9 |
| Total score | 27/30 |
Table 6. Post-treatment scores obtained on Mini Mental Status Examination (MMSE)
Overall, the improvements noted in the participant’s performance across linguistic and cognitive goals targeted for treatment displays the efficacy of telepractice in the present study.
The current study aimed to evaluate the feasibility and efficacy of tele speech and language therapy of a participant with cognitive communication disorder. Telepractice can serve as an excellent medium to treat individuals with communication disorders. The participant in the present study had a history of Traumatic Brain Injury as a consequence of Road Traffic Accident. Following a baseline evaluation of language and cognitive skills, the patient underwent tele speech and language intervention over a course of seven months.
Speech and Language therapy techniques followed to facilitate spontaneous speech and naming were Promoting Aphasics’ Communication Effectiveness (PACE) and Phonological Component Analysis (PCA). The scores obtained on Western Aphasia Battery (Kertesz and Poole, 1982) by the participant in all the domains targeted for intervention revealed a trend of consistent improvement across sessions. It can be observed that post treatment spontaneous speech output improved as the percentage of errors decreased. This finding provides insights into the feasibility of implementing Promoting Aphasics’ Communication Effectiveness (PACE) (through telepractice to remediate communication deficits post TBI.
Further, it is noteworthy that significant improvements were noted in the naming skills of the participant post treatment with Phonological Component Analysis (PCA). Improvements in the naming ability subsequent to PCA corroborate previous research on the effectiveness of phonological therapy approaches in aphasia. It can be appreciated that, the phonological cues offered during treatment with PCA has resulted in significant gains for the participant. Particularly, the results indicate that internet-based videoconferencing systems can achieve significant gains in the treatment of individuals with cognitive communication disorders.
However, it should be noted that although the present study has demonstrated significant treatment gains, telepractice poses a number of challenges.
Intermittently, audio and video delays contribute to the major challenge one may face. This may cause difficulties in recording and scoring error responses. Poor audio-visual quality will lead to over estimating or under estimating the patient’s responses. Good technological infrastructure is very crucial in the successful treatment of communication disorders through telepractice. In current telerehabilitation platforms with the advancements in technology, these challenges can be overcome. Overall, the results of this investigation have proved that telerehabilitation can transform remediation of persons with communication disorders.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
