
Research Article | DOI: https://doi.org/10.31579/2692-9406/100
1Professor and Head/Senior Consultant Physician, Department of Medicine/Department of Nephrology, Defence Services Medical Academy, Defence Services General Hospital, Myanmar.
2Consultant Physician, Defence Services General Hospital, Myanmar.
3Public Health Specialist, Defence Services General Hospital, Myanmar.
4Consultant Physician, Phaung Gyi COVID Hospital, Myanmar.
5Consultant Physician, Defence Services Liver Hospital, Myanmar.
6Consultant Physician, Defence Services General Hospital, Myanmar.
7Consultant Physician, Military Hospital, Myanmar.
*Corresponding Author: Khin Phyu Pyar, Professor and Head/Senior Consultant Physician, Department of Medicine/Department of Nephrology, Defence Services Medical Academy, Defence Services General Hospital, Myanmar.
Citation: Khin P Pyar, Aung P Kyaw, Nyan L Maung, Zar N H Aung, Thi H Tun. (2022). Efficacy and Safety of Tocilizumab in Severe Covid-19 Infection in Second and Third Wave of Epidemics in Myanmar: Multicenter Randomized Controlled Trial. Biomedical Research and Clinical Reviews. 6(3); DOI: 10.31579/2692-9406/100.
Copyright: © 2022 Khin Phyu Pyar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 November 2021 | Accepted: 02 February 2022 | Published: 07 February 2022
Keywords: tocilizumab; standard treatment; severe covid-19 infection; survival; inflammatory markers
Background: Coronavirus disease 2019 (COVID-19), emerged in China at the end of 2019, became a major threat to health around the world as it caused significant morbidity and mortality. SARS-CoV-2 infection induces a cytokine storm due to dose-dependent production of IL-6 from bronchial epithelial cells; therefore, Tocilizumab, a monoclonal antibody against the interleukin-6 receptor, is one of the recommended drugs for treatment of COVID-19 infection. It may result in better outcomes in patients with severe Covid-19 infection. The efficacy and timing of Tocilizumab therapy in severe COVID-19 infection in Myanmar was not known clearly.
Methods: A hospital based interventional study design (Randomized controlled trial) was conducted in COVID-19 treatment centers in Myanmar -Yangon and Nay Pyi Taw, from February 2020 to August 2021. Supervised treatment was done; and, both clinical and laboratory data were collected by using standardized forms and analysis was done. We conducted a double-blind, randomized, placebo-controlled trial of intravenous Tocilizumab in adults who were hospitalized with severe COVID-19 infection. Patients were randomly assigned to receive either Tocilizumab or placebo for within 5 days. The primary outcome was the time to recovery, defined by either discharge from the hospital or hospitalization for infection-control purposes only.
Results: A total of 105 patients (55 in Tocilizumab group and 50 in Standard treatment group) with severe COVID-19 infection were included. Baseline characteristics in Tocilizumab group and Standard treatment group were as follows: (1) mean age 64.4 ± 11.9 years and 59.9 ± 15.8 years; (2) BMI 24.3 ± 3.0 and 23.9 ± 5.0; (3) mean duration of symptom onset to hospital admission was 9.5 ± 4.4 days and 6.5 ± 3.8; (4) mean duration of symptom onset to treatment was 12.8 ± 3.8 days and 7.1 ± 3.8 days; (6) mean duration of hospital stay was 20.1 ± 16.5 days and 11.4 ± 4.8 days; (7) associated co-morbidities was 88% and 70%; and, (8) mean CXR severity score by Braxia was 12.0 ± 2.0 and 9.6 ± 3.4 respectively. The survival rate in early treatment receiving group was 80% in Tocilizumab group and 65.5% in Standard treatment group; that of median treatment receiving group was 40% and 62.5% respectively. The survival rate in late treatment receiving group reduced to 36% in Tocilizumab group; however, no one survived in Standard treatment group.
Inflammatory markers (Ferritin, LDH, D dimer and CRP) dropped significantly at 24 hours and 72 hours after Tocilizumab treatment; the difference was noticeable between survivors and non-survivors. Absolute lymphocyte count, liver enzymes (AST and ALT) and procalcitonin levels became normal by 2 weeks. No significant changes were seen in serum creatinine and blood urea level. Both clinical observation and questioning on experienced side effects from patients on recovery revealed that Tocilizumab therapy was tolerable and safe.
Conclusions: Tocilizumab treatment was associated with a lower risk of mortality than Standard treatment group among patients with severe COVID-19 infection. The chance of survival was 36% if Tocilizumab treatment was given late- more than 15 days of symptom onset unlike Standard treatment. The significant inflammatory markers which could predict survival within 24 to 72 hours were serum ferritin, LDH, D dimer and CRP. Tocilizumab treatment in severe COVID-19 infection was safe and effective particularly it was given early.
Coronavirus disease 2019 (COVID-19) has been spreading worldwide since December 2019; it causes global health threat. Once SARS-CoV-2 virus enters host, there is initial phase of high viral replication, followed by the host immune response which lead to a rapid increase in proinflammatory cytokines, an uncontrolled inflammatory response, acute respiratory distress syndrome (ARDS), and multiple organ failure (G. Chen et al., 2020) (García, 2020). The severity of clinical manifestation and survival depend on protective immunity and immune dysregulation. The better the protective immunity, the less severe the clinical status; and, the host wins the battle. On the other hand, if immune dysregulation dominates, the chances of recovery is less likely; the sequence of acute inflammation, cytokine storm, acute lung injury, ARDS, coagulopathy and multi-organ failure occurs one after another (Wu et al., 2020).
The concentration of pro-inflammatory cytokines, such as IL-6, were related with clinical severity; thus, prognosis. The high level of cytokines also indicates a poor prognosis in COVID-19. Moreover, postmortem examination revealed that excessive infiltration of pro-inflammatory cells, mainly involving macrophages and T-helper 17 cells in lung tissues of patients with COVID-19. SARS-Cov-2 virus selectively induces a high level of IL-6 and results in the exhaustion of lymphocytes. In cytokine storm, IL 6 plays a major role; thus IL-6 inhibitor becomes treatment option in severe COVID-19 infection (Bhaskar et al., 2020).
The symptoms of COVID-19 vary from mild to very severe fatal form; the majority of patients infected with COVID-19 are either asymptomatic or mild form and they recover within weeks. The minority of infected patients, moderate, severe and critical form, have clinical features of severe pneumonia, respiratory failure, acute respiratory distress syndrome (ARDS), sepsis with multi-organ dysfunction, septic shock and acute thrombosis: acute coronary syndrome, pulmonary embolism and acute stroke; they require intensive treatment. Thus, early diagnosis, treatment, and prevention of the cytokine storms are extremely important for the patients.
Severe SARS-CoV-2 infection induces hyperinflammation with overproduction of pro-inflammatory cytokines; elevated serum cytokines, including interleukin-6 (IL-6), IL-10, tumor necrosis factor-α (TNF-α) and interferon-γ, may cause fatal ARDS, sepsis, multi-organ failure and acute thrombosis in COVID-19 patients. Among inflammatory cytokines, serum interleukin-6 elevation is strongly associated with COVID-19 severity and mortality; therefore, the inhibition of IL-6 may retard COVID-19-induced cytokine storm and disease progression.
Tocilizumab, a recombinant humanized anti-IL-6 receptor monoclonal antibody, has been approved for uses in patients with rheumatologic disorders and cancers; it is the second drug recommended by the WHO for COVID-19 treatment after recommending dexamethasone in September 2020. In US, it has been used as emergency used authorization for hospitalized adults and pediatric patients (aged 2 years and older) with COVID-19 who are receiving systemic corticosteroids and require supplemental oxygen, noninvasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO) since June 2021. The current evidence indicates that tocilizumab, an IL-6 inhibitor, is relatively effective and safe (Tang et al., 2020). Tocilizumab is a monoclonal antibody against interleukin-6 receptor-alpha that is used to treat certain inflammatory diseases. Better outcomes in patients with severe Covid-19 pneumonia who received tocilizumab have been observed in case reports. Thus, a hospital based prospective comparative study was conducted to detect efficacy and safety of Tocilizumab in severe COVID-19 infection.
Many reports showed clinical benefits of tocilizumab treatment in COVID-19 patients (Zhang et al., 2020) (Xu et al., 2020) (Martínez-Sanz et al., 2021) (Kewan et al., 2020) (Alam & Bizri, 2021) (Liberato et al., 2020). However, minimal benefits was seen in several large-scale, multi-center observations and randomized clinical trials (Tsai et al., 2020) (Stone et al., 2020)(Khan et al., 2021)(C. Chen et al., 2021) (Rosas et al., 2021) (Elsokary et al., 2020)(Colaneri et al., 2020). Therefore, this study aimed to assess the efficacy of Tocilizumab in severe COVID-19 infection in Myanmar.
Study design and participants
A hospital based interventional study (Multicenter andomized controlled trial) was conducted among severe COVID-19 patients attending at COVID-19 treatment centers in Myanmar- Yangon and Nay Pyi Taw, from February 2020 to August 2021. All in patients with severe SARS-CoV-2 infection confirmed by a positive result on RT-PCR testing of a nasopharyngeal sample and WHO severity score were included in this study.
All adult patients (> 18 years) with severe COVID-19 infection confirmed by positive polymerase-chain-reaction (PCR) assay of nasopharyngeal swab with SaO2 less than 92% were included in this study. Patients were excluded if they have active tuberculosis, pregnancy, active malignancy, ESRD and HIV infection. All patients received standard treatment according to Myanmar National guideline; remdesivir, glucocorticoids, antibiotics, prophylactic enoxaparin, oxygen, and nutritional support and supportive care.
Those who could afford to share cost of Tocilizumab were given Tocilizumab in addition to standard treatment. If clinical signs or symptoms did not improve or worsened (clinical status assessed and defined by attending physician), a second infusion of tocilizumab was administered 24 hours after the first dose after discussion with treatment team. The primary analysis was performed at day 28. Primary outcome was clinical improvement or deterioratinn in clinical status at day 28 after treatment assessed by treating physician. Secondary outcome was survivor or non-survivor at day 28 after treatment.
Informed consent was taken from patients or from the patient’s legally authorized representative who could provide oral consent with appropriate documentation by the investigator. This study was approved by the hospital research and ethics committee of No.(1) Defence Services General Hospital (1000-Bedded) Mingalardon, Yangon.
Study area
This study was carried out at four purposively selected treatment centers, Dagon Hospital (500-bedded), Mingaladon hospital (500-bedded) , Phaung Gyi hospital (1500-bedded) and Nay Pyi Taw hospital (1000-bedded) treatment centers, which were designated for confirmed severe COVID-19 patients. Patients from Yangon Region were treated in Dagon hospital, Mingaladon hospital and Phaung Gyi hospital whereas those from Nay Pyi Taw region were hospitalized in Nay Pyi Taw hospital. All treatment centers have ICU facilities and treatment were given by junior physicians, supervised by senior consultant physicians with on line meeting at least daily.
Proportion in group1 (p1) = 0.900
Proportion in group2 (p2) = 0.600
Non-inferiority or superiority margin (δ) = 0.500
Ratio between 2 groups (k) = 1.0
Alpha (α) = 0.05, Z (0.950) = 1.644854
Beta (β) = 0.20, Z (0.800) = 0.841621
Sample size: n1 = 52, n2 = 52
Operational definitions
Body mass index (BMI) was a person’s weight in kilograms divided by the square of height in meters and it an indicator of body fatness. BMI was categorized as underweight (< 18.5 kg/m2), normal weight (18.5 to 24.9 kg/m2), overweight (25.0 to 29.9 kg/m2) and (≥ 30.0 kg/m2) obese. Comorbidity was a presence of more or additional medical conditions or diseases in COVID-19 patients.
Standard treatment group included those receiving dexamethasone, remdesivir, prophylactic enoxaparin, oxygen, and nutritional support. Tocilizumab group included those receiving Tocilizumab treatment in addition to Standard treatment. This study had two arms: in one arm, tocilizumab (400 mg) intravenously was added to standard treatment (dexamethasone, remdesivir, antibiotics, prophylactic enoxaparin, oxygen, and nutritional support) which was named as “Tocilizumab group”. In another arm, standard treatment (dexamethasone, remdesivir, antibiotics, prophylactic enoxaparin, oxygen, and nutritional support) alone was given which was named as “Standard treatment group”.
Depending on timing, mean duration of symptom onset to Tocilizumab treatment in Tocilizumab group and mean duration of symptom onset to Remdesivir in Standard treatment group, they were divided into 3 groups.
Early treatment receiving group in Tocilizumab group was those patients who received the Tocilizumab within 7 days of symptom onset. Early treatment receiving group in Standard treatment group was those patients who received the Remdesivir within 7 days of symptom onset.
Median treatment receiving group in Tocilizumab group was those patients who received the Tocilizumab between 8-14 days of symptom onset. Median treatment receiving group in Standard treatment group was those patients who received the Remdesivir between 8-14 days of symptom onset.
Late treatment receiving group in Tocilizumab group was those patients who received the Tocilizumab more than 15 days of symptom onset. Late treatment receiving group in Standard treatment group was those patients who received the Remdesivir more than 15 days of symptom onset.
Timing/duration of symptoms onset to admission (days) was time from first symptom to arrival at hospital.
Duration of hospital stay was total duration of hospital stay till discharge either in survival state or non-survival state which may be beyond secondary outcome i.e., 28 days.
Primary outcome was clinical improvement or deterioration in clinical status at day 28 after treatment and it was assessed by treating physician. Secondary outcome was survivor state or non-survivor state at day 28 after treatment.
Severity of cardiomegaly in CXR was categorized as “0 to 3” depending on degree of cardiac enlargement: (1) “0” if heart size was normal; (2) “1” if there was mild degree of cardiomegaly; (3) “2” if there was moderate degree of cardiomegaly; and, (4) “3” if there was severe or gross cardiomegaly.
Severity of lung parenchyma involvement in CXR was calculated by Brixia Score as “0 to 18”. lungs were divided into six zones on a postero-anterior (PA) or antero-posterior (AP) projection. In the second step, a score (0 to 3) is assigned to each zone based on lung abnormalities as follows: (1) “0” if there was no lung abnormalities; (2) “1 “if there was interstitial infiltrates; (3) “2” if there was interstitial and alveolar infiltrates with interstitial predominance; and, (4) “3 “ if there was interstitial and alveolar infiltrates with alveolar predominance.Finally, the scores of the six lung zones are then added to obtain an overall CXR score ranging from 0 to 18.
Oxygen requirement was classified as NC (nasal canula), HFM (high flow mask), DFM (oxygen double source with high flow mask), NIV (non-invasive ventilation- CPAP or BiPAP) and, invasive ventilation.
Based on WHO severity score, the clinical severity of COVID‐19 infection was classified into four types: mild,moderate, severe and critical. In mild category, patients have symptoms only, CXR is normal and, SaO2 on air is normal. In moderate category, CXR shows pneumonias and SaO2 on air is ≥ 90%. In severe category, respiratory rate is > 30/min and, SaO2 on air is < 92>
The level of ferritin was defined as elevated when it was higher than 400 ng/mL (30-400 ng/ml). The level of LDH was defined as elevated when it was higher than 225 U/l (135-225 U/l).The level of D dimer was defined as elevated when it was higher than 0.5 μg/ml (< 0>
Data collection and procedures
The data of demographics and comorbidities from confirmed COVID-19 infection by nasopharyngeal swab for PCR were taken on admission; their clinical severity was assessed by WHO severity score. CXR and laboratory tests were done. They were randomly assigned for one of the treatments: standard treatment plus Tocilizumab (Tocilizumab group) or standard treatment alone (Standard treatment group). If their assignment was Tocilizumab group and they were affordable, Tocilizumab was given. If they could not afford Tocilizumab, they received Standard treatment and they were in Standard treatment. All severe patients received standard treatment according to Myanmar National guideline; remdesivir, glucocorticoids, antibiotics, prophylactic enoxaparin, oxygen, and nutritional support and supportive care.
If clinical signs or symptoms did not improve or worsened (assessed and defined by attending physician), a second infusion of tocilizumab was administered 24 hours after the first dose after discussion with treatment team. The primary analysis was performed at day 28. Primary outcome was clinical improvement or deterioration in clinical status at day 28 after treatment assessed by treating physician. Secondary outcome was survivor or non-survivor at day 28 after treatment.
The blood levels of inflammatory markers (ferritin, LDH, D-dimer and CRP), complete picture, liver enzymes, serum creatinine and sugar were done before and after tocilizumab administration (24 hour, 72 hour, 1 week, 2 week, 3 week and 4 week). The most recent ferritin, LDH and D dimer, CRP, complete picture, liver enzymes, serum creatinine and sugar values before tocilizumab administration was selected as the value of before tocilizumab therapy and the changes of the value after tocilizumab administration was observed for 4 week (24 hour, 72 hour, 1 week, 2 week, 3 week and 4 week). The clinical outcome of the patients was evaluated daily till 4 week after treatment. Both clinical, radiological and laboratory data were collected in standardized proforma and confidentiality was maintained. The data were checked by two medical officers and then, supervision, completeness, and consistency of collected data were performed by the principle investigator.
The primary analysis was a stratified log-rank test of time to recovery with Tocilizumab as compared with placebo, with stratification by disease severity (the actual severity at baseline). For time-to-recovery and time-to-improvement analyses, data for patients who did not recover and data for patients who died were censored at day 10.
Prespecified subgroups in these analyses were defined according to sex, baseline disease severity (according to stratification criteria and on the basis of the ordinal scale), age (18 to 39 years, 40 to 64 years, or ≥65 years), race, ethnic group, duration of symptoms before randomization (measured as ≤10 days or >10 days, in quartiles, and as the median), site location, and presence of coexisting conditions. To assess the effect of disease severity on treatment benefit (recovery and mortality), post hoc analyses evaluated interactions of efficacy with baseline ordinal score (as a continuous variable).
We calculated that 105 patients (55 in Tocilizumab group and 50 in Standard treatment group) using a 2-sided significance level of .05. All patients who were randomized and received at least 1 dose of Tocilizumab, or for the standard care group were assessed for efficacy and adverse events. We used SPSS version 23 and SAS version 9.4 for all analyses.
For the primary efficacy end point, each Tocilizumab group was compared with the standard care group at a 2-sided α =0 .05. Proportional odds models were used with treatment as the independent variable; odds ratios and 95% CIs are presented. The assumption of proportional odds was tested using the score test, and supporting P values from the Wilcoxon rank sum test are provided if the proportional odds assumption was not met. Analyses including baseline clinical status as a covariate were also performed.
For the secondary end point of proportion of patients with adverse events throughout the duration of the study, comparisons between each Tocilizumab group and the standard care group were performed using a Fisher exact test; point estimates of the group differences and corresponding 95% CIs were calculated. For the prespecified exploratory end points, death was considered the competing risk in these time-to-event analyses. Patients without the event of interest were censored on the day of the last nonmissing ordinal scale assessment.
All-cause mortality was estimated using the Kaplan-Meier product limit method with all available data. Each Tocilizumab group was compared with the standard care group using the log-rank test, and hazard ratios and 95% CIs were provided.
Durations of oxygen therapy and hospitalization were summarized and compared between groups using the Wilcoxon rank sum test used to compare parameters whenever appropriate. A p value of less than .05 was considered statistically significant. The collected data were entered into Microsoft Excel 2016 and exported to IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp) for analysis. Descriptive statistics were presented as frequency and percentages for categorical variables and mean (standard deviation, SD) for continuous variables. Bivariable logistic regression analysis was performed to assess the relative impact of the predictor variables on the outcome variable. To control for potential confounding factors, multivariable logistic regression analysis was performed. All independent factors with p value < 0.05 in bivariable regression analysis were candidates for the multivariable logistic regression model. The results of group comparisons of risk factors and severity of disease were expressed as adjusted odds ratio (AOR) with 95% CI and a p value was set at < 0.05 for statistical significance.
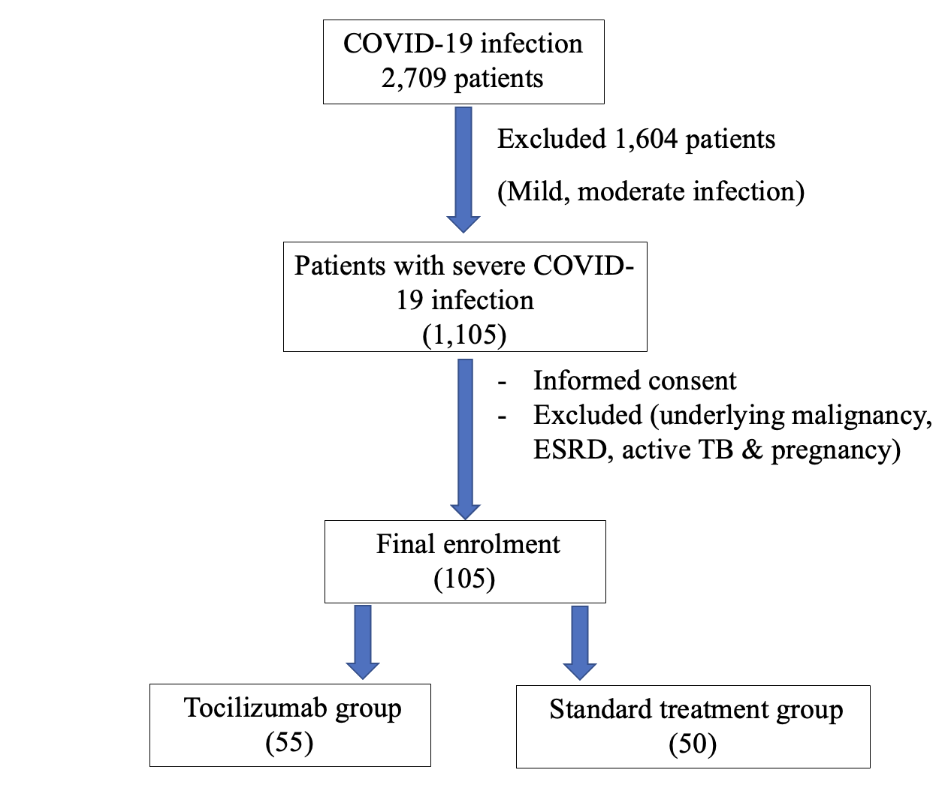
Although initial enrollment included 2,709 cases with COVID-19 infection, 1,604 cases of mild to moderate infections were excluded. Out of 1,105 cases with severe infection, only 105 cases, 55 patients in Tocilizumab group and 50 patients in Standard treatment group, were finally included after obtaining informed consent.
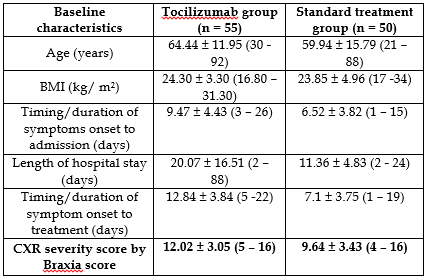
Table (1) shows baseline characteristics of patients in two treatment group. Mean age of patients in Tocilizumab group was 64.6 years whereas it was 59.9 years in Standard treatment group; BMI was almost the same, 24.3 and 23.9 respectively. Duration of symptom onset to hospital admission was longer- 9.5 days in Tocilizumab group and 6.5 days in Standard treatment group.
Duration of symptom onset to treatment was also longer- 12.8 days in Tocilizumab group and 7.1 days in Standard treatment group. Length of hospital stay was again longer- 20 days in Tocilizumab group and 11 days in Standard treatment group. CXR severity score by Brixia score was higher-12 in Tocilizumab group; it was less 10 in Standard treatment group.
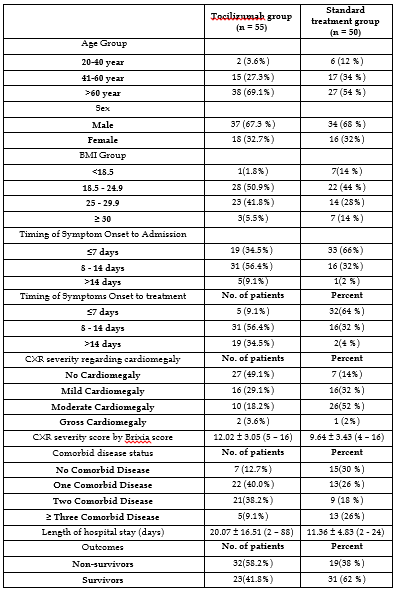
Break down comparison is demonstrated in Table (2). Nearly 90% of patients in Tocilizumab group had co-morbid diseases; however, only 70% of patients in standard treatment group had co-morbidities. Most of the patients in both groups had mild to moderate cardiomegaly in chest radiograph. Only 42% of patients in Tocilizumab group survived; nevertheless, 62% in standard treatment group survived.
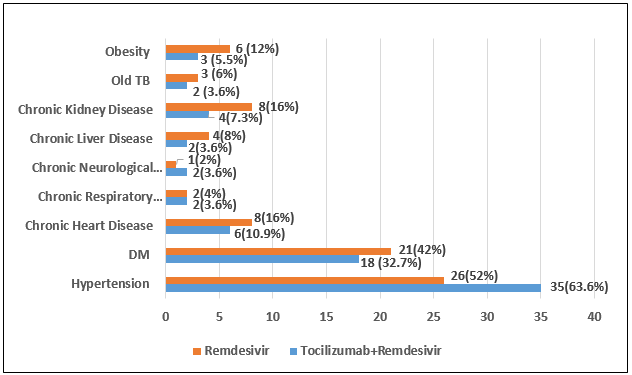
Figure (2) reveals associated co-morbidities in both groups; hypertension, diabetes mellitus and heart disease were common.
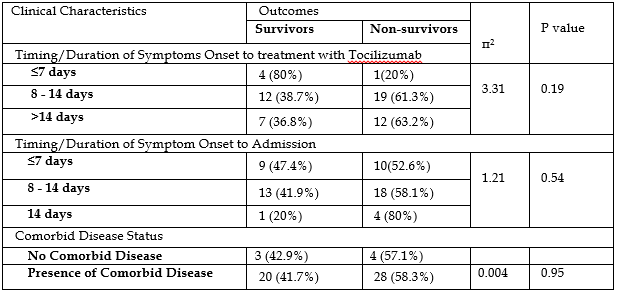
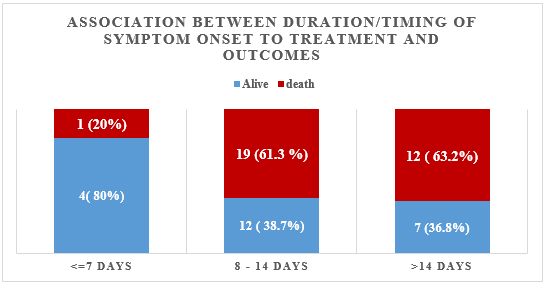
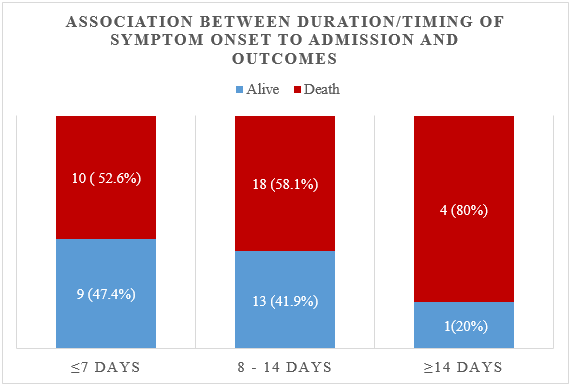
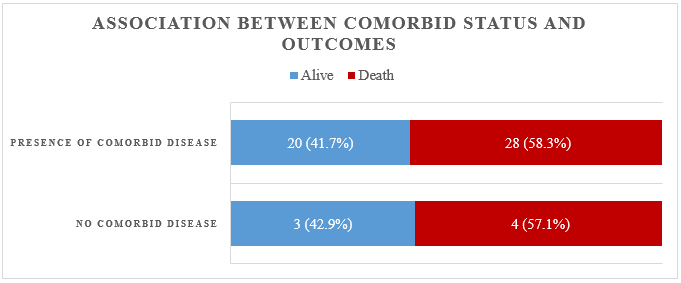
The association between clinical characteristics and outcomes is mentioned for each group in Table (3) and (4). In Tocilizumab group, the chances of survival were highest (80%) in patients who got treatment early- less than 7 days; it dropped to 39% and 37% if they received treatment late- more than 8 days and 14 days respectively. Similar pattern was seen in duration of symptom onset to hospital admission; early comers had highest survival rate. However, presence of co-morbid diseases did not influence the survival.
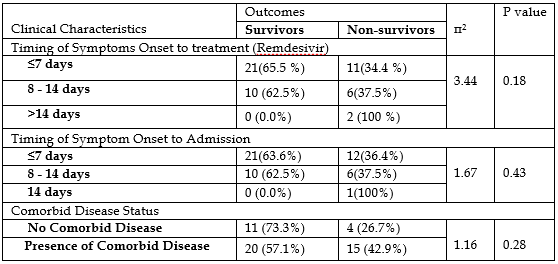
In standard treatment group, the chances of survival were highest (66%) in patients who got treatment early- less than 7 days; it dropped to 63% if they received treatment late- more than 8 days. Similar pattern was seen in duration of symptom onset to hospital admission; early comers had highest survival rate. However, presence of co-morbid diseases did not influence the survival. It is also shown in Figure (5).
Regarding duration of symptom onset to treatment, the striking difference was noted in non-survivors. The chances of death were higher if the treatment was not given earlier; 63% in Tocilizumab group and almost 100% in standard treatment group. In other words, there was chances of survival- nearly 40% if Tocilizumab was given late- 2 weeks after symptom onset. It is clearly seen in Figure (3) and (4).
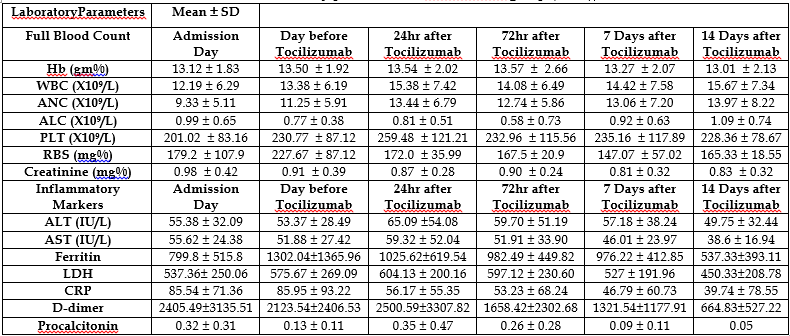
Table (4) demonstrates changes in laboratory parameters. Haematological improvement, normal absolute lymphocyte count, was seen significantly in 2 weeks after treatment whereas inflammatory markers (CRP, LDH and Ferritin) dropped significantly at 24 hours and 72 hours after treatment. Liver enzymes (AST and ALT), D-dimers and procalcitonin levels became normal by 2 weeks. There were no significant changes in serum creatinine and blood urea level.
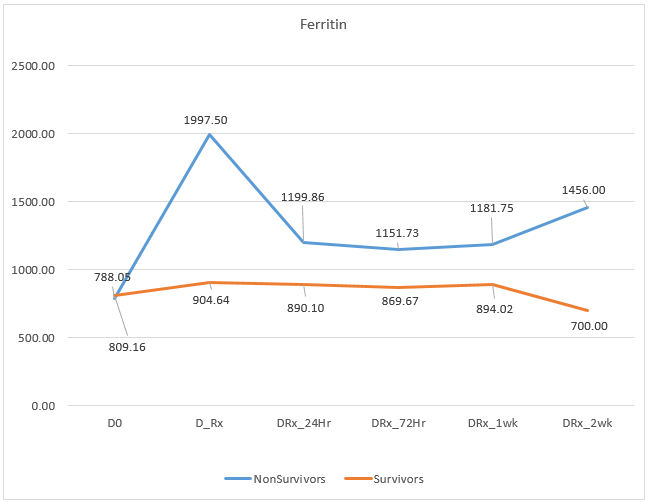
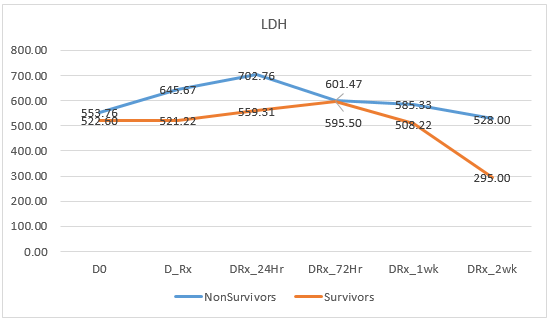
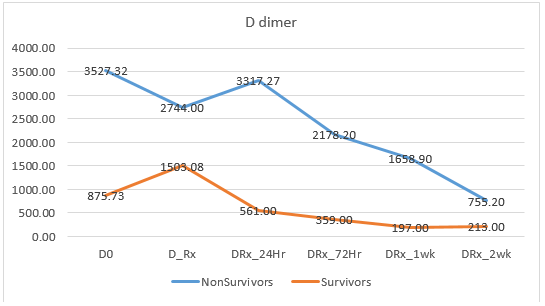
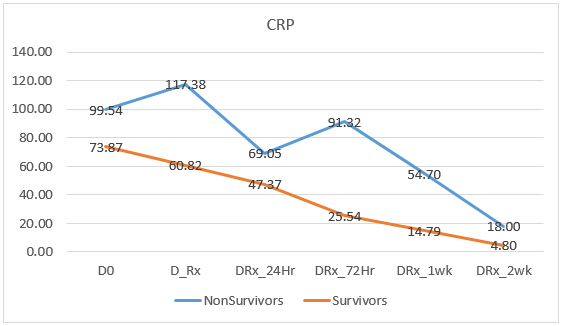
In Tocilizumab group, ferritin level in survivors dropped dramatically than non-survivors; it is demonstrated in Figure (6). Similar changes were seen in both LDH level, D dimer and CRP level; it is drawn in Figure (7), (8) and Figure (9) respectively.
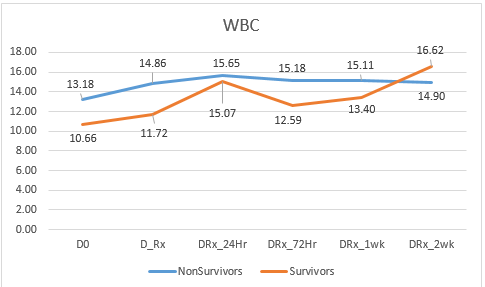
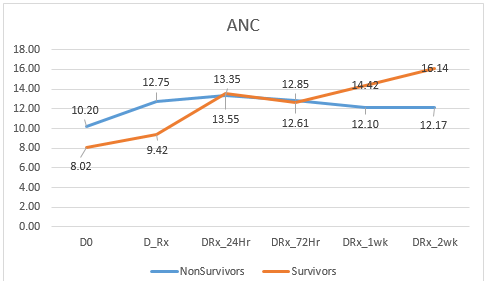
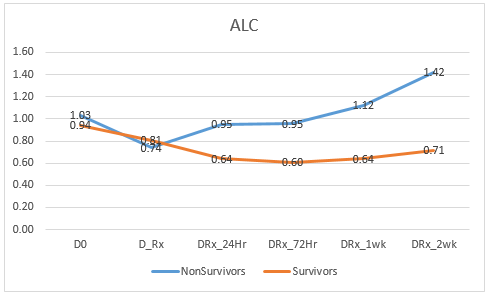
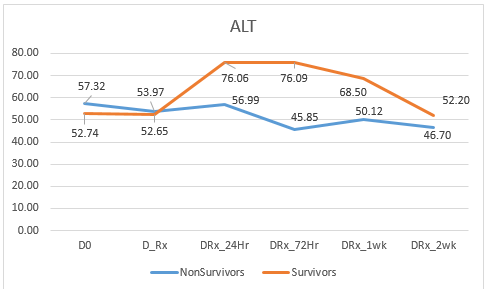
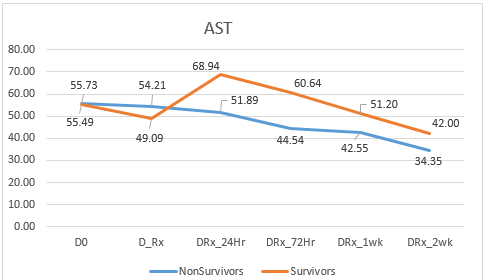
In contrast, haematological parameters like total WBC count, absolute neutrophil count, absolute lymphocyte count and platelet count as well as liver enzymes (ALT, AST) and renal profile (serum creatinine) did not show significant difference between survivors and non-survivors. Figure (10), (11), (12), (13), (14), (15) and (16) have revealed them.
Coronavirus disease 2019 (Covid-19) is associated with immune dysregulation and hyperinflammation, including elevated interleukin-6 levels. The use of tocilizumab, a monoclonal antibody against the interleukin-6 receptor, has resulted in better outcomes in patients with severe Covid-19 pneumonia in case reports and retrospective observational cohort studies. The efficacy of Tocilizumab therapy in patients with severe COVID‐19 infection was studied in second and third wave in Myanmar, developing country.
In this study, base line characteristics in both groups were favorable to poor outcome; however, patients in Tocilizumab group were more severe than Standard treatment group as their mean age was older and their BMI was higher. In addition, they came to hospital late; they got treatment 5 days later than Standard treatment group. Furthermore, nearly 90% of them had co-morbidities compared to 70% in Standard treatment group. Besides, their initial CXR severity score was worse; score 12 in Tocilizumab group and score 9.6 in Standard treatment group. Moreover, Tocilizumab group had longer hospital stay, 20.07 ± 16.51 days, compared to 11.36 ± 4.83 days in Standard treatment group which reflected the need for longer oxygen requirement and ventilatory support. However, the survival rate in early treatment receiving group was 80% in Tocilizumab group and 65.5% in Standard treatment group; that of median treatment receiving group was 40% and 62.5% respectively. The survival rate in late treatment receiving group reduced to 36% in Tocilizumab group; however, no one survived in Standard treatment group.
Thus, Tocilizumab therapy led to lower risk of mortality. Therefore, this study confirmed the earlier reports (Xu et al., 2020) (Zhang et al., 2020) (Alam & Bizri, 2021) (Liberato et al., 2020).
In addition, the oxygen requirement of most of the patients did not increase after Tocilizumab therapy. None of them did not require ventilatory support following Tocilizumab; thus, it proved the fact by Wei et al “ Tocilizumab therapy led to lower risk of mortality and the requirement for ventilatory support” (Wei et al., 2021). Three patients were already on ventilator prior to Tocilizumab therapy; none of them survived because of age (over 75 year), underlying heart failure with huge cardiomegaly and poor ejection fraction, hypertension and chronic kidney disease. Other studies on Tocilizumab included mechanically ventilated cases ; and their findings were positive (Guo et al., 2020) (Alam & Bizri, 2021) (Xu et al., 2020) (Somers et al., 2021). In this study, nasopharyngeal swab conversion to negative PCR results after Tocilizumab therapy was done in only 20 cases; it took 7-10 days to get PCR conversion. In Indonesia study, nasopharyngeal swab conversion to negative PCR results was quicker with Tocilizumab (Widysanto et al., 2021).
In this study, the chances of survival were highest (80%) in patients who got treatment early- less than 7 days; it dropped to 39% and 37% if they received treatment late- more than 8 days and 14 days respectively. Therefore, the best timing for Tocilizumab therapy should be less than 7 days symptom onset; it pointed out the report by Moreno Diaz et al., (2021) suggesting the timing of Tocilizumab therapy at “10 days” after symptom onset (Moreno Diaz et al., 2021). Farooqi et al.(2020) recommended aggressive early treatment with Tocilizumab to prevent and overcome cytokine storm; best therapeutic effect (Petrak et al., 2021) (Zarębska-Michaluk et al., 2021).
On the other hand, efficacy of Tocilizumab therapy in COVID-19 infection in reducing short term morality was disregarded by other studies and they suggested meta-analysis was required (C. Chen et al., 2021) (Rosas et al., 2021). Some researchers overlooked its use (Elsokary et al., 2020) (Colaneri et al., 2020).
A single dose of Tocilizumab (400 mg one vial) was used in all patients except 4 cases; 3 out of 4 patients survived and they also received convalescent plasma therapy in this study,. Because both clinical improvement and the level of inflammatory markers (serum ferritin, LDH, D-dimer and CRP) were not satisfactory at 24 hours after first dose of Tocilizumab, the treating team decided to give second dose. As the patients were affordable, second dose was given and it saved them. The one who succumbed after second dose was desperate; elderly woman having gross cardiomegaly with chronic heart failure and she was on ventilatory support. If the non-survivors received repeated dosage of Tocilizumab particularly in early state, their outcome would be better. In the study done in Pakistan, they used fix dose of Tocilizumab 600 mg for cost saving; and, the result was favorable (Moes et al., 2021).
The main reason for using single dose in this study was “money factor”; the cost of one vial of Tocilizumab 400 mg/vial was sky rocket high, nearly 100 times its original price, during third wave of epidemic in Myanmar. This point also led to late admission to hospital as well as late treatment. If Tocilizumab was prescribed early i.e., less than one week symptom onset, the outcome would be better. Also, repeated doses might alter the prognosis. One report suggested to give two to three doses in critically ill patients or patients with an extremely higher level of IL‐6. The earliest report from China in 2020 recommended to repeat Tocilizumab especially in critically ill patients with raised IL-6 level (Luo et al., 2020).
In this study, the earliest improvement in inflammatory markers was seen at 24 hours after treatment; and, it became more pronounced at 72 hours. Among the inflammatory markers which dropped more significantly in survivors were serum ferritin, LDH, D dimer and CRP; the initial drop 24-72 hours after Tocilizumab treatment as well as the subsequent fall till 2 weeks were well recognized in survivors. Thus, the significant changes in level of inflammatory markers within 24 to 72 hours after treatment could predict the survival. Moreover, the decision to give repeated dose of Tocilizumab could be made from changes in their blood level in addition to clinical status. Initial slight fall in ferritin within 24 to 72 hours and further spiked in ferritin after one week was clearly seen in non-survivors. Therefore, our findings supported the effectiveness of Tocilizumab in the prevention or treatment of cytokine storms induced by COVID‐19. All inflammatory markers, serum ferritin, LDH, D dimer and CRP level, reflected that Tocilizumab treatment prevented or treated cytokine storms in patients with severe COVID-19 infection though IL-6 levels could not be performed due to economic constraint. Farooqi et al. (2020) proposed early, proactive identification of serum acute phase reactants and aggressive early treatment for cytokine storm, to get optimal therapeutic benefits and obviate the need for mechanical ventilation, thereby decreasing mortality (Farooqi et al., 2020).
No adverse drug reaction was recorded in this study. One case, 91 year old male had recovered from severe COVID-19 pneumonia developed colonic perforation on 17 days after Tocilizumab therapy, day 28 symptom onset. In remaining 54 cases, both liver enzymes level and serum creatinine level did not rise after Tocilizumab therapy in this study. Therefore it was safe, supporting other report (Liberato et al., 2020). Though Tocilizumab may cause neutropenia, superinfections, reactivation of latent infections (Nosheen N et al., 2020), hepatitis, and cardiac abnormalities, there was no evidence of hepatitis or cardiac abnormalities in this study. There was no serious side effect except mild giddiness, appetite loss and nausea although the side effects like hypersensitivity, cytopenias, hepatic injury and gastrointestinal perforation were notable adverse effects of tocilizumab (Afra et al., 2021). Deana et al. (2021) reported pulmonary aspergillosis as a complication of Tocilizumab, the patients in Tocilizumab group did not have such complication within the study period -28 days.
There were several limitations in this study. First, Tocilizumab was very expensive, 100 times its original price particularly in third wave of epidemics in Myanmar; thus, most of the patients could not afford to buy as part of cost-sharing therapy. It caused unlikely to repeat second dose or third dose. The outcome would have changed if the patients received them. Moreover, the timing of tocilizumab therapy matters. If they got tocilizumab therapy early, they would survived more. In addition, this study would be stronger if it was a randomized control trial. Here, one of the inclusion criteria was affordability of Tocilizumab therapy from patient side. Furthermore, the sample size was not large though the study covered 1000-bedded and 300-bedded COVID treatment centers. Besides, blood IL-6 level which is direct evidence of blood level of IL-6 in cytokine storm should be measured rather than measuring other inflammatory markers- ferritin, LDH, D-dimer and CRP. Finally, observation with a sufficient number of COVID‐19 patients in RCT is still needed to document the effectiveness of Tocilizumab.
Although base line characteristics in Tocilizumab group were poorer than Standard treatment group such as older age, higher BMI, late hospitalization, late treatment, longer hospital stay, more co-morbidities and higher CXR severity score by Brixia, the survival rate of Tocilizumab treatment was better than Standard treatment group particularly Tocilizumab treatment was given early in treating patients with severe COVID-19 infection, The chance of survival was 36% if Tocilizumab treatment was given even late- more than 15 days of symptom onset whereas it was almost zero with Standard treatment. The earliest improvement in inflammatory markers was seen at 24 hours after treatment; and, it was more pronounced at 72 hours. Absolute lymphocyte count, Liver enzymes (AST and ALT), D-dimers and procalcitonin levels became normal by 2 weeks. The significant inflammatory markers which can predict survival within 24 to 72 hours were serum ferritin, LDH, D dimer and CRP; and, repeated dose of Tocilizumab is required if their fall is not satisfactory. Tocilizumab treatment in severe COVID-19 infection was safe and effective especially it was given early.
Randomized control trial with large number of cases with repeated dosage of Tocilizumab are required for better information. Solution for use of expensive drugs in clinical trials and treatment should be find out. Inflammatory markers like serum ferritin, LDH, D-dimer and CRP can be used as response to treatment in developing countries who cannot do expensive marker like IL-6 level.
We are thankful to Professor Ko Ko Lwin, Professor Kyaw Zay Ya, Directorate of Medical Services; Dr. Zaw Myo Han, Dagon hospital; Dr Moe Myint, Mingaladon hospital, Dr Khin Aung Tun, Phaung Gyi hospital; and, Dr. Aung Myat Kyaw, Nay Pyi Daw hospital for their administrative support. We are also grateful to all health professionals at the treatment centers for their efforts in providing effective care for the patients.
The data collection using standardized case report forms was approved by Hospital Ethics Review Committee of Defence Services General Hospital, Mingaladon. The permission to collect the data was also approved by the authorities of Hmawbi and Indine COVID-19 treatment centers, Yangon Region, Myanmar. Privacy and confidentiality of information were maintained throughout the study process.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
