
Research Article | DOI: https://doi.org/10.31579/2641-0419/348
Hegau Bodensee Klinikum Singen, Gesundheitsverbund Landkreis Konstanz, Virchow Str. 10, 78224 Singen.
*Corresponding Author: © 2024, Marc Kollum. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Citation: Sabrina Geng, Jonas Haberland, Elisabeth Haberland, Julia Hromek, Heidi Zimmermann, et al, (2024), Effects on Fatigue and Depression 11 And 19 Months after a Sars-Cov-2 Infection a Case Control Study, J. Clinical Cardiology and Cardiovascular Interventions, 7(2); DOI:10.31579/2641-0419/348
Copyright: © 2024, Marc Kollum. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 February 2024 | Accepted: 13 February 2024 | Published: 19 February 2024
Keywords: fatigue; cognitive fatigue; motor fatigue; depression; post-covid; sars-cov2
Background:
Long- and post-COVID syndrome still needs research. Providing help to the large number of affected individuals in a professional manner is only possible if convincing data on their pathophysiology and the duration of symptoms is provided.
Objectives:
To investigate the incidence of symptoms of fatigue and depression 12 months and 19 months after SARS-CoV-2 infection in comparison to a SARS-CoV-2 negative control cohort.
Materials and methods:
The presence of fatigue and depression was evaluated in both groups via Fatigue Scale for Motor and Cognitive Functions (FSMC) and Patient Health Questionnaire (PHQ-9).
Results:
185 SARS-CoV-2 PCR-positive subjects and 168 subjects with negative SARS-CoV-2 antibody titers were recruited.
General fatigue symptoms were more common in the SARS-CoV-2 positive group (OR initially 3.8; 95% CI 2.1 to 6.7). During follow up the odds ratio concerning the development of symptoms of fatigue decreased while still being statistically significant (OR follow-up 2.6; 95% CI 1.5 to 4.6).
The association of the infection with motor fatigue, is higher in comparison to cognitive fatigue (OR initial 3.5 and follow-up 3.2 vs OR initial 3.0 and follow-up 2.4).
After 19 months, clinically relevant depressive symptoms are no longer significantly more frequent in the SARS-CoV-2 positive cohort (OR initial 3.0 ; 95% CI 1.4 to 6.1/OR Follow-Up 1.1; 95% CI 0.6 to 2.0).
Conclusion:
Symptoms of fatigue and depression were initially registered more than twice more frequently in SARS-CoV-2 positive subjects. During follow-up, the association of general fatigue and SARS-CoV-2 infection decreased, while still being significant. In this context motor fatigue showed the strongest association with SARS-CoV-2 infection. However, the association between symptoms of depression and the initial infection could no longer be observed.
In medicine, the term “fatigue” is used for a symptom of tiredness. If fatigue is considered as a symptom complex or disease it is nowadays most frequently referred as chronic fatigue syndrome (CSF) or myalgic encephalomyelitis (ME).
Pooled prevalence of CSF/ME using the the Centers for Disease Control (CDC)-1994 definition is 0,89%. However the prevalence of CFS/ME shows a wide range depending on definition and diagnostic method [1]. Chronic fatigue syndrome is most frequently, in more than 50% of cases [2], triggered by viral infections. Nevertheless the etiology and pathophysiology of fatigue or CFS/ME have not yet been fully clarified.
Objective disease-specific, biological parameters and imaging diagnostics, such as computed tomography and magnetic resonance therapy, for fatigue or diagnosis of CSF are current research goals. Clinical presentation of CFS/ME is very heterogeneous. The main symptoms are excessive fatigue, lack of energy and exhaustion lasting over 6 months, which cannot be relieved by rest or recuperation [3]. The slightest physical or mental exertion aggravates the symptoms and causes post-exertional malaise (PEM)[4]. Sleep disorders, cognitive impairments such as memory, attention and concentration disorders, non-specific myalgias/arthralgias with pathological muscle fatigue and ataxia are common [4]. In addition, there are psychiatric symptoms such as emotional instability, anxiety and depression[4].
During the course of the pandemic, an international meta-analysis showed that 56.9% of COVID-19 patients still had symptoms for at least two months after infection [5]. The most common symptoms were fatigue (31.4%), dyspnoea (24.1%), pain (19.9%), anxiety (18.9%) and sleep disorders (17.8%)(5). According to the guideline recommendation of the British National Institute for Health and Care Excellence (NICE) [6] persistent symptoms from 4 -12 weeks after acute SARS-CoV-2 infection not explained by an alternative diagnosis are titled ongoing symptomatic COVID-19 and after 12 weeks Post-COVID-syndrome.
The possible mechanisms for the development of Post-COVID-syndrome can be divided into 3 categories: viral persistence, long-lasting inflammation and disturbed autoimmunity [7].
Study Design
The study at hand was designed as a sub-study of the FSC19-KN [8]. It was conducted as a monocentric cohort study in a controlled setting. Its main objective was to investigate the incidence of mental health disorders in SARS-CoV-2 positive subjects living in the local district of Constance (Baden Wurttemberg, Germany). Approval was given by the ethics committee of the Albert-Ludwigs-University (Freiburg). The study was registered on the German Clinical Trials Register and Clinicaltrials.gov.
Participants
In the main study FSC19-KN [8] 280 participants had a Polymerase-Chain-Reaction (PCR)-confirmed SARS-CoV-2 infection and 238 controls showed negative SARS-CoV-2 antibody titers. During initial visits, the age, gender, medical history, presence of symptoms of COVID-19, necessity of hospitalization, monitoring in an intensive care unit/mechanical ventilation, pre-existing medical conditions and cardiovascular risk profile was recorded systematically.
We contacted all subjects of the main study and asked them to participate in our sub-study (Figure 1).
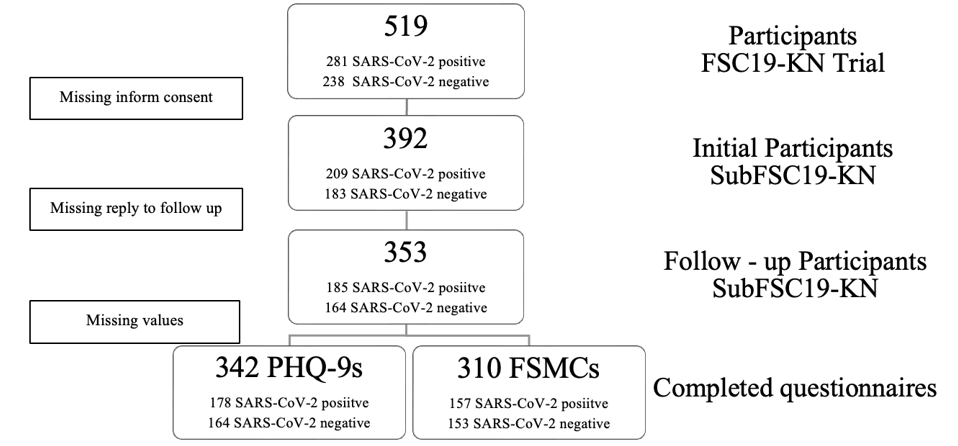
Figure 1
The presence of fatigue (Fatigue Scale for Motor and Cognitive Functions, FSMC), depression and anxiety disorder (Patient Health Questionnaire, PHQ-9/-PD) was evaluated via online questionnaires or by post using paper versions.
Questionnaires
In multiple sclerosis patients fatigue is well known and has a high prevalence up to 78.0% as a secondary illness [9]. It can be further divided into cognitive or motor fatigue [10]. The FSMC is highly sensitive and specific in detecting fatigue in multiple sclerosis patients and its internal consistency and reliability are high [11]
The FSMC general fatigue score (20-100) categorizes none to mild (score < 53>
fatigue score (10-50) categorizes none to mild (score < 28>
The Patient Health Questionnaire-9 (PHQ-9) comprises nine questions concerning depression. Its total score (0-27) is used to determine the degree of depression (none to severe) [12].
The PHQ–9 is a validated survey for major depression with a sensitivity of 88% and a specificity of 88% at a cutoff score of 10 or higher [12]. The score categorizes none to mild (score < 10>
Ethical Consideration
The task of filling out the questionnaires can be stressful for subjects with preexisting mental disorders and lead to an aggravation of their psychological state. To address this problem personal consultation, assistance completing the questionnaires and further information on possible contact addresses were provided to the participants if necessary.
Descriptive statistics were used for a comparative presentation of sociodemographic data. All statistical analyses were performed with STATA (StataCorp. 2019, Texas, USA). FSMC and PHQ-9/-PD score results are given as mean ± standard deviation (SD). Differences in means (DM) and their respective 95% confidence intervals (CI) were calculated via t-test for independent samples with pooled variances. The strength of the association between two events was quantified by odds ratios (OR). The respective 95%-confidence intervals were determined by log odds ratio function. Missing values were not included during data analysis but recorded accurately. All study data were collected and managed using a Research Electronic Data Capture (REDCap) platform [14,15] hosted at https://redcap.glkn.de. The accuracy of the data entries was verified by an external monitor according to guidelines for good clinical practice.
At the time of study inclusion only 7 subjects (3,5%) of the SARS-CoV-2 positive subjects were hospitalized and 1 subject (0,5%) was ventilated mechanically and monitored in an intensive care unit. The mean tie from PCR testing to initial survey in September 2021 is 341±89 days (11.4 ± 3.0 months). The mean time from PCR testing to follow-up survey from January to June 2022 is 572 ± 77 days (19.1 ± 2.6 months).
Regarding only participants with completed follow-up, 185 SARS-CoV-2 PCR-positive subjects and 168 subjects with negative SARS-CoV-2 antibody titers were included. The average age of the SARS-CoV-2-positive participants is 48.7 years, in the control group 49.9 years. In total, 106 of the SARS-CoV-2-positive subjects (57.3%) and 98 of the control subjects (58.3%) are female, the rest are male (Table 1).
SARS-CoV-2 Positive n=185 | Controls n=168 | |
| Age– Years (M ± SD) [95% CI] | 48,7±15,3 | 49,9±14,1 |
| 18-39 – Number(%) | 53 (28,6) | 36 (21,4) |
| 40-59 – Number(%) | 91 (49,2) | 90 (53,6) |
| 60-79 – Number(%) | 40 (21,6) | 42 (25,0) |
| ≥ 80 – Number (%) | 1 (0,5) | 0 (0,0) |
| Sex | ||
| Male – Number(%) | 79 (42,7) | 70 (41,7) |
| Female – Number(%) | 106 (57,3) | 98 (58,3) |
Legend: M (mean); SD (standard deviation); CI (confidence interval); OR (odds ratio)
Table 1: Distribution of age and gender among the study population
During the follow-up, 33 subjects (18.3%) of the SARS-CoV-2-positive cohort reported having had another positive PCR test. In the control group, 49 (29.3%) positive PCR tests were recorded during follow-up.
Moderate to severe general fatigue is determined with the FSMC primarily in 59 participants (32.6%) in the SARS-CoV-2-positive group and in 19 participants (11.4%) in the control cohort. This results in an odds ratio of 3.8 (95% CI 2.1 to 6.9; p<0>
In the SARS-CoV-2-positive group, the average score achieved in the general FSMC score is thus significantly higher (42.5 ± 20.3 vs. 31.8 ± 15.2). The average score achieved by the SARS-CoV-2-positive group is therefore on the borderline of the mild fatigue range (≥ 43 points). However, the average achieved by the SARS-CoV-2-negative group was more clearly within the normal range (<43> Odds Ratio (OR) p-value Missing Values SARS-CoV-2-positive / Controls 42,5±20,3 [39,5;45,5] 40,5±19,4 [37,5; 43,6] 31,8±15,2 [29,5; 34,1] 33,0±17,0 [30,3;35,7] Initial: 4 / 1 FU: 28 / 15 None – Mild Fatigue Number (%) OR Initial 3,8 [2,1;6.7] P<0> OR FU 2,6 [1,5;4,6] P=0,0011 Moderate – Severe Fatigue Number (%) 21,3±10,4 [19,8; 22,8] 20,4±10,2 [18,8; 22,0] 15,9±7,8 [14.6; 17.0] 16,4±8,5 [15,0; 17,8] Initial: 3 / 1 FU: 20 / 11 None – Mild Fatigue Number (%) OR Initial 3,0 [1,6;5,3] P=0,0003 OR FU 2,4 [1,3;4,3] P=0,0031 Moderate – Severe Fatigue Number (%) Score Fatigue motor (M±SD) [95% CI] 21,2±10,3 [19,7;22,7] 20,1±10,0 [18,6; 21,6] 16,0±7,7 [14,8; 17,1] 16,6±8,9 [15,2;18,0] Initial: 3 / 1 FU: 18 / 10 None – Mild Fatigue Anzahl (%) OR Initial 3,5[2,0;6,2] P<0> OR FU 3,2 [1,8;5,8] p=0,0001 Moderate – Severe Fatigue number (%) Score PHQ-9 (M±SD) [95% CI] 5,4±4,8 [4,4; 5,4] 5,1±4,7 [4,3; 5,3] 3,1±3,8 [3,4; 4,3] 4,1±4,8 [4,3; 5,3] Initial: 0 / 1 FU: 7 / 4 None – Mild Symptoms number (%) OR Initial 3,0 [1,4;6,1] p=0,0031 OR FU 1,1 [0,6;2,0] p=0,7512 Moderate – Severe Symptoms number (%) SARS-CoV-2-Positive Controls Initial Follow-Up Initial Follow-Up 185 185 168 168 Score Fatigue overall (M±SD) [95% CI] 122 (67,4) 111 (70,7) 148 (88,6) 132 (86,3) 59 (32,6) 46 (29,3) 19 (11,4) 21 (13,7) Score Fatigue cognitive (M±SD) [95% CI] 134 (73,6) 122 (73,9) 149 (89,2) 137 (87,3) 48 (26,4) 43 (26,1) 18 (10,8) 20 (12,7) 123 (67,6) 116 (69,5) 147 (88,0) 139 (88,0) 59 (32,4) 51 (30,5) 20 (12,0) 19 (12,0) 153 (82,7) 152 (85,4) 156 (93,4) 142 (86,6) 32 (17,3) 26 (14,6) 11 (6,6) 22 (13,4)
Legend: M (mean); SD (standard deviation); CI (confidence interval); OR (odds ratio)
Table 2: Overview of results
Thus, the odds ratio from general fatigue after SARS-CoV-2 infection decreased in the follow-up survey, it remained significantly increased (OR follow-up 2.6; 95% CI 1.5 to 4.6; p=0.0011).
Initially, moderate and severe cognitive fatigue symptoms occurred significantly more frequently in the SARS-CoV-2-positive group with an odds ratio of 3.0 (95% CI 1.6 to 5.3; p<0>
With an odds ratio of 3.5 (95% CI 2.0 to 6.2; p<0>
Looking at the symptoms of fatigue recorded, divided into cognitive and motor, the odds ratio shows an overall higher association of the infection with motor fatigue than with cognitive fatigue (OR initial 3.5 and follow-up 3.2 vs. OR initial 3.0 and follow-up 2.4). The odds ratio and thus the association with SARS-CoV-2 infection was also highest for motor fatigue over the course of the follow-up after approximately 19 months.
Clinically relevant depressive symptoms were significantly more frequent in the SARS-CoV-2-positive group after 12 months (OR 3.0; 95% CI 1.4 to 6.1; p=0.0031). During the follow-up, the number of moderate and severe depressive symptoms in the SARS-CoV-2-positive group decreases and the number in the control group increases, so that the association with SARS-CoV-2 infection is no longer present or significant (OR 1.1; 95% CI 0.6 to 2.0; p=0.7512) (Table 2).
This sub-study shows that even 11 and 19 months after the initial predominantly mild course of COVID-19, a considerable number of SARS-CoV-2-positive test subjects still show symptoms. Symptoms of fatigue syndrome and depressive symptoms are significantly more common after a SARS-CoV-2 infection compared to a control group.
Due to the initially low hospitalization rate in the SARS-CoV-2-positive cohort, the results mainly apply to mild courses. However, the study results can be applied to the majority of infected patients in Germany, as more than 90% of COVID patients in Germany were not hospitalized in 2020/2021 [16].
The prevalence of general moderate and severe fatigue after SARS-CoV-2 infection recorded here is consistent with the descriptions of the prevalence of fatigue in one of the largest meta-analyses. Di Gennaro and colleagues [5] were able to show a prevalence of fatigue after COVID of 31.4% in 2022. However, the majority of the included studies were conducted with subjects after hospitalization and fatigue was predominantly surveyed as a perceived symptom without a questionnaire or classification [5]. One of the few comparable studies with a control cohort from Geneva [17] showed the prevalence of fatigue compared to a negative control cohort at 16.0% and 3.1 months after SARS-CoV-2 infection. Deviating results may be related to patient population, COVID-19 vaccination or the assessment of fatigue using the Chalder Fatigue Score [17].Over the course of the follow-up, this study shows a decrease in fatigue symptoms in the SARS-CoV-2-positive cohort after an average of 19 months after SARS-CoV-2 infection, while an increase was recorded in the control cohort. A decrease in fatigue symptoms in the SARS-CoV-2-positive cohort was in line with the expectations and results of studies with Post-COVID subjects. Tran et al. [18] were able to demonstrate a reduction in symptoms after 12 months in subjects with Post-COVID-Syndrome, but around 85% of the subjects still had persistent symptoms.
The results described here regarding the subdivision of fatigue with a focus on motor fatigue support possible theories of direct muscle damage in patients with Post-COVID-Syndrome. It was shown a decrease in muscle mass [19,20] and a decrease in hand strength [20] in Post-COVID-19 patients with intensive medical therapy.
Moderate to severe depressive symptoms are also initially more than twice as common in the SARS-CoV-2-positive cohort. Before the pandemic, the overall prevalence of depressive symptoms in Germany (determined by PHQ-8 score > 10) of 10.1% was recorded in the GEDA 2014/2015-EHIS study of the Robert Koch Institute [21].
The prevalence of depressive symptoms (PHQ-9 score > 10) in the control cohort was a little lower in our survey. This small deviation can be explained by our smaller patient population or by the additional questioning of suicidality in the PHQ-9.
The increase in fatigue and depressive symptoms in the control cohort could be caused by a SARS-CoV-2 infection during the course of the study or by overall circumstances and the psychosocial impact of the pandemic.
In addition, the subjects answered questions about their thoughts, feelings or behaviors in relation to their mental health. This can lead to a bias in the self-report [22].
A selection bias is also conceivable, as subjects suffering from severe depression or fatigue may have been more likely to refuse to participate in the study [23].
Awareness of the infection itself and its potentially serious consequences influence the SARS-CoV-2-positive group compared with nocebo effect, so that they may report possible symptoms significantly more frequently.
The subjects in the SARS-CoV-2 cohort were infected with the initial coronavirus (alpha variant) in the first and second wave between July 2020 and January 2021. The results are therefore primarily applicable to this variant and not vaccinated persons. At the time of study inclusion, no specific vaccination was yet available.
Co-factors in addition to COVID-19 disease or SARS-CoV-2 infection may also have influenced this observation. Pandemic, social and economic circumstance can play an important role especially within occurance of mental illnesses
Even 11 and 19 months after SARS-CoV-2 infection, almost a third of the initial SARS-CoV-2-positive test subjects still show moderate and severe fatigue symptoms. The control group shows that both, cognitive and motor fatigue, can be significantly more often associated with the infection. The follow-up showed that the focus of the symptoms was on fatigue and no longer on depression. Further studies dealing with this topic are urgently needed to identify the exact mechanisms and optimize the treatment of a large number of fatigue patients. Awareness for the multisystematic illness post-COVID-Syndrome and faster diagnosis could improve medical care. Drug therapy could be developed on the basis of pathophysiological mechanisms.
Acknowledgements
the author would like to thank the Werner Messmer Foundation for its financial support of this publication
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
