
Research Article | DOI: https://doi.org/10.31579/2692-9562/061
1 Başakşehir Çam and Sakura City Hospital, Department of otorhinolaryngology, İstanbul/Turkey
2 Uskudar State Hospital, Department of internal medicine
*Corresponding Author: Ahmet Baki, Başakşehir Çam and Sakura City Hospital, Department of otorhinolaryngology, İstanbul/Turkey.
Citation: Ahmet Baki, Selçuk Gündoğar. (2023). Effects of vitamin B12 on olfactory functions. Journal of Clinical Otorhinolaryngology 5(1); DOI: 10.31579/2692-9562/061
Copyright: © 2023, Ahmet Baki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 December 2021 | Accepted: 20 January 2022 | Published: 28 January 2023
Keywords: Vitamin B12; smell test;olfactory function
Objective: To evaluate the effects of vitamin B12 on olfactory functions.
Materials and Methods: The smell scores of 48 patients with vitamin B12 deficiency were compared before and after the treatment. The patients followed in the internal medicine were referred to the otolaryngology for the smell test. Smell test was done to the patients before the treatment. After three month of treatment, patients whose vitamin B12 levels reached normal limits were given a smell test.
Results: There were 28 female and 20 male patients in the study. The ages of the patients participating in the study ranged from 24 to 45, and the mean age was 33.9±5.4 years. While the threshold, identification, and total score values of the patients were 2,45±0,5, 3,52±0,5, and 2,98±0,34, respectively, after treatment, 4,7±0,94, 5,32±0,7, and 5,02±0,66. A statistically significant difference was found in the comparison of scores before and after treatment. (p=0.001)
Conclusion: Vitamin B12 treatment provides an improvement in olfactory functions.
Olfaction plays an important role in our daily lives, and olfactory dysfunction causes a significant decrease in the quality of life. Approximately 20% of the general population complains about olfactory dysfunction, and 5% of these individuals are anosmic [1]. Psychophysical and electrophysiological tests are often used to evaluate olfaction function. Even though psychophysical tests are generally used for the clinical evaluation of people with smell dysfunction, electrophysiological tests are mostly used for further investigation [2]. The Connecticut Chemosensory Clinical Research Center (CCCRC) olfactory test evaluates the butanol threshold and smell identification [3]. It is validated for the analysis of smell capacity in the Turkish society [4]. It is easy to prepare, cheap, and simple to administer [4]. Because vitamin B12 is not produced in the body, it must be taken from the diet [5]. Vitamin B12 deficiency may be due to insufficient intake, as in vegetarians; however, malabsorption is an essential factor for deficiency [5]. The relation of vitamin B12 deficiency to neurological symptoms has been shown for a long time [5]. Subacute combined degeneration of the spinal cord is the best manifestation of the neurological findings of vitamin B12 deficiency. The dorsal and lateral columns of the spinal cord are affected in this disease. In the case of vitamin B12 deficiency, neurological symptoms such as paresthesia, sensory ataxia, fatigue in the lower extremities, dementia, and optic atrophy can be seen. Rarely, extrapyramidal symptoms such as cerebellar ataxia, dystonia, and chorea may also be seen [6]. Previous studies showed that vitamin B12 deficiency might lead to deficiency in olfactory functions [7]. In this study, we aimed to analyze the olfactory function with the CCCRC olfactory test in individuals with isolated vitamin B12 insufficiency and to reveal the changes in the olfactory level after vitamin B12 replacement therapy.
This study included 48 patients with vitamin B12 insufficiency was conducted between june and December 2019. The participants were selected from the internal medicine clinic on the basis of their vitamin B12 testing and then referred to the ENT clinic for olfactory testing. A detailed history was taken from all the patients, and a routine ear, nose, and throat examination was also performed. Patients with nasal septum devia- tion, acute or chronic rhinosinusitis, active upper respiratory tract infection, nasal polyposis, history of nasal surgery, allergic rhinitis, smoking, systemic diseases (e.g., diabetes mellitus, hypothyroidism, hypertension, chronic renal failure, and chronic liver failure), neurological diseases, <18>
Smell assestant
The CCCRC test comprises of a butanol threshold and an identification as already reported [4]. It was administered pre- treatment and in the 12th week post-treatment.
Butanol threshold test
The participants were given two glass bottles of the same color and uniform view, one of which contained water and the other a dilute concentration of butanol during the test. They were then ordered to close one nostril and place the tip of the first bottle quickly below the other one. The second bottle was then sampled in a similar manner, and the participant had to select which of the bottles contained something other than water. If the selection was incorrect, a more potent concentration of butanol was submitted along with the bottle having only water. Possible scores ranged from 0–9, but scores ≥7 were scored as 7 per the olfactory test protocol. For the final score, the average of both nostril scores was taken.
Identification test
Cinnamon, Vicks, chocolate, Turkish coffee, peanut butter, carbonate, soap, and baby powder were added to opaque bot- tles. The ability to sniff out Vicks showed unimpaired trigeminal nerve function, and all the subjects easily recognized it; therefore, it was not added to the final score. Possible scores ranged from 0 to 7. For the final score, the average of both nostril scores was taken.
Total score
Scores for the butanol threshold and identification tests were later averaged to reach a total score, which was classified as defined by Cain et al [9].
Statistics
Statistical Package for the Social Sciences 22 program was used for statistical analysis. The suitability of parameters to normal distribution was evaluated by Shapiro-Wilks test. Descriptive statistical methods (mean and standard deviation) were determined when evaluating the study data. Wilcoxon Signed Rank test was used to evaluate the dependent non-parametric data. One-way Analysis of variance test was used to compare the groups in terms of stages. P<0>
There were 28 female and 20 male patients in the study. The ages of the patients participating in the study ranged from 24 to 45, and the mean age was 33.9±5.4 years. While the threshold, identification, and total score values of the patients were 2,45±0,5, 3,52±0,5, and 2,98±0,34, respectively, after treatment, 4,7±0,94, 5,32±0,7, and 5,02±0,66. A statistically significant difference was found in the comparison of scores before and after treatment. (p=0.001). While before treatment B12 vitamin levels was 139,56±10,8 ng/L after traetment 548,3±29,2 ng/lt.
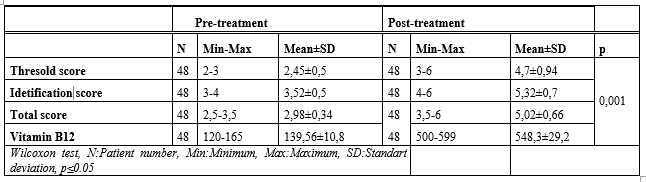
Table 1: Comparison of scores before and after treatment
Olfactory dysfunction may occur because of conductive or sensorineural problems. Conductive dysfunction may occur because of nasal pathologies, whereas sensorineural dysfunction may develop owing to the olfactory receptor and subsequent central pathways [10]. This study reports that vitamin B12 insufficiency is associated with smell abnormality. Mean olfactory test scores are significantly increased in people with vitamin B12 insufficiency after a vitamin B12 replacement protocol. The number of patients with anosmia and hyposmia decreased after vitamin B12 replacement therapy. Previous studies have shown that vitamin B12 deficiency affects the central and peripheral nervous system. The most common neurological disorder as a result of vitamin B12 deficiency is peripheral neuropathy. Also is, subacute combined degeneration well-known and common neurological disorder in vitamin B12 deficiency [11]. Acute chorea, cerebral ischemia, infratentorial and supratentorial leukoencephalopathy are rare diseases that occur as a result of vitamin B12 deficiency [12]. It has been shown that olfactory functions improve after B12 deficiency treatment in a very few cases with olfactory dysfunction (13). Our study shows the positive effect of vitamin B12 treatment on olfactory functions. The pathophysiologic mechanisms of vitamin B12 deficiency in the nervous system are unclear. It is claimed to occur as a result of insufficient remethylation of homocysteine to methionine. The pathophysiological mechanisms of vitamin B12 deficiency in the nervous system are unclear. However, insufficient remethylation of homocysteine to methionine and excessive propionyl-CoA formation lead to degenerative conversion of methylmalonyl-coenzyme A (CoA) to succinyl-CoA, resulting in a decrease in the supply of methyl groups [14]. As a result of deteriorated fatty acids and a defect in the methylation of myelin basic protein, the myelin sheath, which is a component of the nervous system synthesis, deteriorates. In addition, increased plasma homocysteine concentrations can have a direct toxic effect on neurons [15]. Another study claimed that olfactory dysfunction was caused by vitamin B12 deficiency and high homocysteine levels leading to myelin damage in the olfactory nerve [16]. It has been shown that the olfactory threshold is positively correlated with the vitamin B12 level [16]. Chronic rhinosinusitis, infectious diseases and trauma are the most important causes of olfactory functions. Healton et al reported that involvement of the nervous system in 40% of patients with vitamin B12 deficiency [17].
In addition to neurological, metabolic, and endocrinological diseases, toxic factors and drugs can cause deterioration in olfactory functions [18]. In our study, we performed an smell test on patients with vitamin B12 deficiency.
Vitamin B12 deficiency causes various neurological disorders as well as olfactory dysfunction. Vitamin B12 treatment provides improvement in olfactory functions. Further studies may be needed to add vitamin B12 therapy to the treatment protocol in patients with olfactory disorders.
Financial disclosure: There is no financial support.
Conflict of Interest: There is no conflict of interest in this article.
Ethical approval: All procedures performed in studies involving human participants were by the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the ethical research committee of the Zeynep Kamil Women's and Children's Disease Training and Research Hospital in Istanbul,
Informed consent: Routine informed consent was obtained from all patients before the hospitalization and also inform consent from the individuals of the control group was obtained in the study. There is no support source that requires confirmation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
