
Review Article | DOI: https://doi.org/10.31579/2690-4861/650
1 Department of Medical Oncology, Center for the fight against cancer of Oran. “Emir Abd El Kader” Faculty of Medicine - Ahmed Ben Bella University - Algeria.
2 Department of Medical Oncology, Center for the fight against cancer of Sidi Bel Abbes.” Taleb Morad” Faculty of Medicine – Djillali Liabes University - Algeria.
*Corresponding Author: Zemmour Amel, Department of Medical Oncology, center for the fight against cancer of Oran, Emir Abd El Kader, Faculty of Medicine –Ahmed Ben Bella 1 University-Algeria.
Citation: Zemmour Amel ˲Tabouri Sarah, Zeroual Sarah, Larbaoui Blaha, (2025), Effect of Intermittent Fasting on Cancer, International Journal of Clinical Case Reports and Reviews, 22(4); DOI:10.31579/2690-4861/650
Copyright: © 2025, Zemmour Amel. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 December 2024 | Accepted: 25 December 2024 | Published: 17 January 2025
Keywords: fasting; cancer; treatment; recurrence
Diet is a modifiable factor that may affect cancer risk, treatment and recurrence, currently there is a high level of interest in fasting and cancer in the scientific community but no clear information about the purported health benefits, fasting and fasting mimicking diets leads to wide alterations in growth factors and in metabolite levels giving rise to an unfavorable environment for cell proliferation, there are multiple examples of fasting diets that might regenerate antitumor immunity and may even prevent some types of tumors which are most likely to be sensitive to these dietary interventions, thus, the biologically-relevant interplay between fasting or nutrient deprivation and current cancer treatments encourages the design of future trials to maximize efficacy and achieve the lowest toxicity of current cancer treatments.
Humans evolved in environments where food was scarce, enabling them to function at high energy levels [1]. However, modern sedentary lifestyles and overconsumption of high-calorie foods have compromised health, leading to issues like insulin resistance, obesity, cardiovascular diseases, depression, and even cancer [1,2]. Fasting, a practice dating back to Hippocrates [2,3], is a safe and well-tolerated method that reduces oxidative stress, enhances stress resistance, delays aging, and potentially combats cancer [4,5]. Intermittent fasting (IF) is a specific eating pattern involving alternating periods of fasting (16-48 hours) and eating (8-12 hours) [6,7]. Lifestyle factors, including diet, contribute to approximately 42% of cancers and 45% of cancer-related deaths [8]. Despite significant advancements in oncology, cancer remains a major global health concern, affecting 19.97 million people and causing 10 million deaths in 2022 [9]. Survival rates and prognoses for cancer patients remain unsatisfactory. Recently, the fasting concept has become popular among scientists and the general population. In particular, fasting reputedly slows down ageing, improves overall health [4-7]. Proposed mechanisms for this effect include an induction of autophagocytosis of cancer cells and/or the idea that fasting may also protect healthy cells in cancer patients against the stress induced by chemotherapy [8-9]. In this review, we aim to describe the various types of fasting, their relationships with cancer treatments, and their effects on cancer, treatment responses, and survival in cancer patients.
Types of fast:
Based on traditional, cultural or religious backgrounds, there are many types of periodic fasting, many types of fasting experience no or small caloric intake (eg 500 kcal daily) with an unlimited amount of caloric-free beverages (coffee without sugar or milk, water, diet soft drinks.) (Table1) [8,10].
| Types of fast | Description |
| Complete alternate day fasting | Involves alternating fasting days and feeding days |
| Modified fasting regimens | Severe energy restriction for 2 non-consecutive days per week and ad libitum eating for the other 5 days. |
| Time restricted feeding | Allows ad libitum energy intake within specific time frames, inducing regular, extended fasting intervals. |
| Religious fasting | Variety of fasting regimens undertaken for religious or spiritual purposes. |
| Ramadan fasting | A fast from sunrise to sunset during the holy month of Ramadan, with one large meal after sunset and one lighter mean before dawn. Thus, for about 12 hours of length. |
| Other religious fasts | Some Christians routinely abstain from food and drink for extended periods of time, some seventh –day Adventists consume their last of two daily meals in the afternoon, resulting in an extended nighttime fasting interval. |
Table 1: Type of fasting
Because Calorie Restriction (CR) can have both very positive and negative effects and is unlikely to be adopted by a significant portion of the populations since it unavoidably causes severe weight loss, intermittent and periodic fasting are emerging as novel interventions which could maintain many of the beneficial effects of CR while reducing the burden and many of the side effects [10]. Fasting, the complete elimination of nutrients from the diet, is the most extreme of the dietary restrictions [11,12]. Fasting regimens can be implemented in various formats (table2). Intermittent fasting (IF) involves short-term, frequent fasting periods, such as alternate-day fasting (ADF) or time-restricted eating (TRE) [11-14]. In contrast, prolonged and periodic fasting (PF) entails less frequent but longer periods of fasting, often lasting 2-5 days or involving fasting-mimicking diets (FMD) for 4-7 days [15-18].
| Type of Fasting | Schedule | Description | |
Intermittent Fasting (IF) | ADF | 24 h fast/ 24 h eating period | Water only fasting every other day |
| 5:2 | 2 days fast or very low-calorie consumption (500–700 kcal)/ 5 days eating period | Alternation of 2 days of very low-calorie consumption with a 5 days ad libitum re-feeding period | |
| TRF | 12- to 18 h fast/ 6- to 12 h eating period | Food intake restricted to 6–12 h per day | |
Periodic Fasting (PF) | Prolonged fasting | 2–5 days of water fast/ 7 days eating period (or longer) | Water only fasting period followed by an ad libitum re-feeding period |
| Prolonged FMD | 4- to 7 days FMD/ 10- to 25days eating period | 30–50% of the normal caloric intake using a fasting mimicking diet for 4–7 days followed by an ad libitum re-feeding period |
Table 2: Dietary approaches to promote health span [15]
While IF typically involves alternating fasting and feeding phases, PF can be implemented sporadically throughout the year [11]. Both IF and PF induce metabolic adaptations, including decreased blood glucose levels, reduced glycogen stores, lower leptin levels, and increased fatty acid mobilization with ketone body production [11,18]. Additionally, fasting periods, particularly those involving FMD, can positively impact cognitive function, leading to heightened awareness, attention, mental acuity, vigilance, and reduced depressive symptoms [19].
Circadian Biology Cycle
The master biological clock is in the suprachiasmatic nucleus of the hypothalamus and is entrained to light and dark stimuli, it plays a major role in integrating metabolism and energetics, similar clock oscillators have been found in peripheral tissues (liver, fat and skeletal muscle..) desynchronization of this biological brain and peripheral clock may increase the risk of cancer, a large literature indicates that shift work is associated with increased risks of obesity, diabetes, cardiovascular disease and cancer, similarly consuming the majority of the day’s energy earlier in the day causes a lower weight and improves health [10].
Gastrointestinal microbiota
The diversity of the Gut microbiota is regulated by fasting, it increases production of short chain fatty acids, which can regulate insulin response and decreases inflammation [3].
Intermittent fasting should be contraindicated if there is a history of an eating disorder (anorexia, bulimia, malnutrition.) or pregnancy [3, 20-22].
Intermittent fasting and cancer
Fasting leads to wide alterations in systemic levels of hormones, growth factors (insulin, glucagon, GH, IGF-1) which reduces the ability of tumor cells to adapt and survive, it can modulate cancer initiation, progression, and recurrence [3, 23-25].
In fasting, low serum levels of glucose impose extra stress on tumor cells, while healthy one’s function normally, these different responses cause more DNA damage and apoptosis in tumor cells and protects healthy cells from treatment damages, it is called differential stress sensitization –DSS [26-27].
IF promotes also stem cell-based regeneration, interestingly, in fasting, cytotoxic agents elicited differential response in normal and tumor cells, a phenomenon known as differential stress resistance –DSR- In healthy cells (Figure1), fasting shuts down pathways promoting growth to re-invest in repair pathways, thus tumor cells lose ability to adapt to extreme environments including caloric deprivation [1, 28,29].
This metabolic stress causes insulin levels to drop and glucagon levels to rise, increasing the breakdown of glycogen into glucose and triglycerides into free fatty acids, lipolysis is maintained by glucocorticoids and adrenalin as a result, fasting benefits the brain, muscle, liver, and adipose tissue, IF boosts fatty acid oxidation and induces a transition from aerobic glycolysis to mitochondrial oxidative phosphorylation in tumor cells [30]. The brain progressively adjusts using the ketone bodies in addition to glucose to satisfy its energy requirements, while other tissues use fatty acids to function. “Warburg effect” in fasting, the normal cells can replace glucose deprivation by ketone bodies and fatty acids, in contrast tumor cells depend on glucose, so it stimulates the aerobic glycolysis and produces lactic acid it’s “Warburg effect, sometimes an “anti-Warburg” effect result in oxidative stress and induced apoptosis of tumor cells [20,31,32].
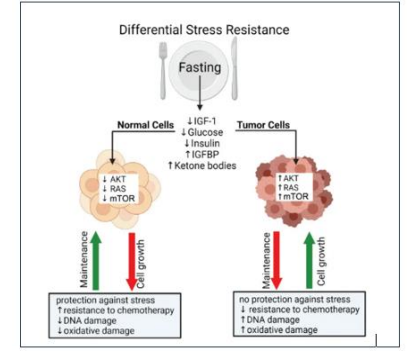
Figure 1: Differential stress resistance mechanisms [30]
The possible mechanisms associated with the differential stress resistance theory. AKT: protein kinase B; IGF-1: insulin-like growth factor 1; IGFBP: insulin-like growth factor binding protein; mTOR: mechanistic target of rapamycin; RAS: rat sarcoma virus.
The related progression on IF combined with tumor therapy was listed in the Table 3.
Fasting has also several effects [3,15,21,31-34]:
However, in practice, many physicians may consider fasting harmful for some kind of cancer patients weakened by a prior chemotherapy (aging with decreased appetite, nausea, taste changes.) [4].
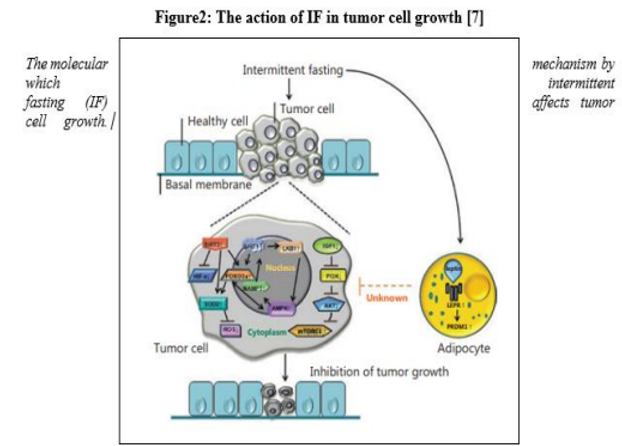
Figure 2: The action of IF in tumor cell growth [7]
The molecular mechanism by which intermittent fasting (IF) affects tumor cell growth. Mechanistically, IF inhib is the IGF-1/AKT and mTORC1 pathways in tumor cells, while the AMPK, SIRT1, and SIRT3 pathways are activated. In addition, AMPK and SIRTs depend on each other in IF-associated metabolic adaptation. However, AMPK can induce activation of SIRT1 through NAMPT, while SIRT1 can activate AMPK through LKB1 regulation. FOXO3a (a downstream molecule of SIRT1 and SIRT3) and AMPK can each enhance the other’s transcriptional activities. Furthermore, SIRT3 inhibits tumor growth by activating FOXO3a and the expression of superoxide dismutase (SOD), thereby reducing the level of reactive oxygen species and negatively regulating the expression of HIF-1α. SIRT3 activates SOD2 via up regulation of FOXO3a. Furthermore, IF can selectively inhibit tumor growth by upregulating LEPR and its downstream signaling path way protein, PRDM1.
| Year | Disease(s) | Dietary regimen | Outcome |
| 2020[35] | Colorectal cancer and other KRAS-mutant tumors | Standard feeding or on the last day of the first IF cycle, vitamin C (4 g/kg in saline) began via intraperitoneal injection twice a day, with at least 6–8 between the 2 daily administrations | The combination of IF and vitamin C represented a promising low toxicity intervention |
| 2019[36] | Orthotopic pancreatic tumors | Fed or fasted for 24 h and then exposed to total abdominal radiation at a dose of 11.5 Gy | IF improved the survival of mice with orthotopic pancreatic tumors subjected to lethal abdominal radiation |
| 2017[37] | Colon cancer | 24 h fasting on alternate days for 2 weeks | IF inhibited colon cancer growth and decreased the production of extracellular adenosine by cancer cells by suppressing CD73 expression |
| 2016[38] | Fibrosarcoma | 48 h fasting (water only) once vs. ad libitum feeding; animals were injected with mitoxantrone or oxaliplatin at the end of fasting | IF improved the efficacy of chemotherapy in an immune system-dependent and autophagy-dependent fashion |
| 2016[39] | Breast cancer; melanoma | 48–60 h fasting (water only) or a 96 h FMD once a week for 2–4 weeks vs. ad libitum feeding; animals were injected with chemotherapy at the end of each fasting and/or FMD cycle | IF slowed tumor progression when combined with doxorubicin or cyclophosphamide, expanded lymphoid progenitors and boosted anticancer immunity |
| 2015[40] | Colon cancer | 48 h fasting (water only) once a week for 2 weeks, 24 h prior to and 24 h after oxaliplatin injection vs. ad libitum feeding | IF improved the anticancer effects of oxaliplatin, exerted anti-Warburg effects and promoted oxidative stress and apoptosis in cancer cells |
| 2015[41] | Lung cancer; colorectal cancer | 48 h fasting (water only) once a week for 3 weeks with daily treatment with crizotinib or regorafenib vs. ad libitum feeding | IF improved the clinical activities of crizotinib and regorafenib |
| 2012[42] | Mesothelioma; lung cancer | 48 h fasting (water only) given once a week for 3 weeks, 32 h prior to and 16 h after cisplatin injection vs. ad libitum feeding | IF sensitized human mesothelioma and lung cancer xenografts to cisplatin |
Table 3: Overview of intermittent fasting (IF) combined with tumor therapy
Intermittent fasting in clinical trials
Most clinical trials of fasting in cancer patients performed to date are retrospective trials, observational studies evaluated in supportive care outcomes or phase I, II clinical trials, currently several well-powered studies are underway to address outstanding questions however, more extensive data are needed before intermittent fasting can be a routine clinical use [3], the DIRECT study evaluated the fasting mimicking diet (FMD) + neoadjuvant chemotherapy in women with HER 2 negative breast cancer, patients in the FMD group had a better pathological response and a decreased chemotherapy induced DNA damage to normal cells [30,43].
Another study on patients with breast cancer identified a potential beneficial of IF on chemotherapy induced toxicity [44].
Fasting and Cancer Prevention
Data on the effect of IF suggest has a beneficial effect in preventing 60% of cancers in animal studies, a Swedish study found a 29% reduction in cancer incidence and 23% lower cancer mortality in a population who underwent a bariatric surgery, the look AHEAD trial of 4859 overweight patients who were randomized to an intensive group of CR (1200-1800 kcal daily) and an observational group, after 11 years patients in the intensive lifestyle group had a 16% lower incidence of obesity-related cancers (including esophagus, colon, rectum, kidney, pancreas, stomach, liver, gallbladder, thyroid, uterine, ovarian…) which the authors proposed was secondary to weight loss, though, there are no known, reproductible diets, to cure or prevent cancer recurrence, future well designed randomized clinical trials should examine the effect of IF over longer periods, different cancers and populations [8,29,45,46].
Fasting during specific treatments of cancer
IF has the potential to lower the ratio of fat to lean body mass, which may benefit patients at risk of weight–related side effects of some cancer treatments, many studies report improvements in quality of life, fatigue and GI toxicities [34], the fasting glucose, insulin and HbA1c of adults with obesity decreases significantly after short alternate- date regimens in some studies [10,47]. Glutamine is another metabolic substrate that has a high conversion rate in tumor cells, the catabolism of glutamine can protect tumor cells from chemical toxicity, fasting can increase chemosensitivity of cancer cells by affecting glutaminase and glutamine transporter levels [32].
Chemotherapy and radiotherapy
Fasting increases autophagy which is a catabolic process providing primary materials such as amino acids, fatty acids, nucleosides/nucleotides, sugars often induced by chemotherapeutic agents [48], many trial evaluates the combination of fasting with chemotherapy represents a potentially promising strategy to increase efficacy, reduce resistance and prevent side effects [25].
Normal cells are protected from chemotherapeutic agents by changes in circulating hormones and metabolites, during nutrient deprivation, they re-invest energy in maintenance and repair that contribute to resistance to chemotherapy while tumor cells are unable to slow-down growth due to mutations in tumor suppressor genes and mitogenic pathways, this different reaction makes tumor cells more susceptible to chemotherapy and other treatments since they violate the anti- proliferation signals required by fasting environment [31].Two days of fasting before chemotherapy treatment is safe and protect against the side effects of chemotherapy, this type of fasting is shown to delay the progression of several tumors especially in mice [27,49,].In addition, IF has been shown to increase tumor sensitivity to radiation therapy (RT) and prolong the survival of fasting experimental animals [Icard]. Specifically, mice with pancreatic tumors subjected to lethal abdominal radiation exhibited improved survival rates when subjected to IF compared to those with ad libitum food access. Additionally, IF did not impair RT-induced tumor cell killing and even enhanced γ-H2AX staining post-RT, suggesting a potential radio sensitizing effect [50]. Encouragingly, preclinical and preliminary clinical data support the notion that IF could serve as a complementary therapy to improve RT outcomes, both in terms of tumor control and reduced normal tissue toxicity [51,52]. While these basic studies have yielded promising results, further preclinical research is necessary to establish clinical relevance, as human data, including clinical outcome studies, safety data, and randomized controlled trials, remain limited [53]. Future investigations should prioritize safety and explore the potential of IF to enhance the efficacy of lower doses of chemotherapy and radiation therapy.
Hormones and fasting
Many studies demonstrate the link between nutrients and particularly protein intake, growth hormones, DNA damage and cancer, two major hormonal pathways appear to affect cancer incidence the IGF-1 and the insulin signaling [15].
Many dietary patterns, including the Western diet, are associated with reduced lifespan and health span and appear to affect cancer incidence by two major hormonal axes/pathways: the growth hormone-IGF1; the insulin signaling [54-56]. Breast cancer, particularly hormone receptor-positive (HR+) breast cancer, represents a significant health challenge. While endocrine therapies like Tamoxifen and Fulvestrant are effective, primary and acquired resistance often limits their long-term efficacy [57, 58].
A periodic fasting or a fasting-mimicking diet can enhance the effectiveness of endocrine therapies in mouse models of HR+ breast cancer. By lowering circulating levels of IGF-1, insulin, and leptin, and inhibiting the AKT-mTOR signaling pathway, these dietary interventions can potentiate the effects of tamoxifen and Fulvestrant. Moreover, combining a fasting-mimicking diet with a cyclin-dependent kinase 4/6 inhibitor like Palbociclib can lead to sustained tumor regression and overcome acquired drug resistance. (57,59) Importantly, fasting and fasting-mimicking diets can also mitigate the side effects of endocrine therapy, such as endometrial hyperplasia caused by tamoxifen. In human clinical trials, fasting-mimicking diets have been shown to induce similar metabolic changes as observed in mice, including reductions in insulin, leptin, and IGF-1 levels. (59,60) These findings suggest that fasting-mimicking diets hold promise as a potential adjuvant therapy for HR+ breast cancer. Further clinical studies are warranted to explore the optimal timing and duration of these dietary interventions and their impact on patient outcomes.
In a study by Lende et al., post-surgical breast cancer patients who fasted prior to surgery demonstrated significantly improved relapse-free and breast cancer-specific survival compared to those who received a carbohydrate-based nutritional supplement. This positive effect was particularly pronounced in patients with estrogen receptor-positive (ER+) breast cancer. Fasting appeared to favorably influence the hormonal environment, potentially enhancing the efficacy of subsequent treatments. While no significant difference was observed in estrogen receptor-negative patients, the study highlights the potential benefits of fasting for a specific subset of breast cancer patients [61].
Fasting and targeted therapy
Intermittent fasting (IF) has been shown to modulate various cellular pathways implicated in cancer progression. By decreasing insulin-like growth factor-1 (IGF-1) levels, IF can activate AMP-activated protein kinase (AMPK) and inhibit the phosphatidylinositol 3-kinase (PI3K)/protein kinase B (AKT) pathway [3,26,31,32]. Additionally, IF can enhance the efficacy of cyclin-dependent kinase 4/6 (CDK4/6) inhibitors, particularly Palbociclib, by reducing pharmacokinetic variability [26]. Furthermore, IF-induced inhibition of mechanistic target of rapamycin (mTOR) and activation of AMPK can stimulate autophagy, a cellular process that removes damaged organelles and misfolded proteins (Kalam, Psara). By reducing IGF-1 levels, IF can also inhibit the RAS/mitogen-activated protein kinase (MAPK) signaling pathway, leading to decreased activity of transcription factors involved in cell proliferation and growth [26, 32]. Overall, these findings suggest that IF can improve the efficacy of targeted therapies, such as tyrosine kinase inhibitors (TKIs), by inhibiting key signaling pathways involved in cancer cell growth and survival [31,32].
Immunotherapy and fasting
When butyrate metabolism is disrupted in colon cancer, it accumulates, inhibits cell development and causes cell death suggesting that microbiota may play a role in immunotherapy as well [10]. There is a growing appreciation for how the metabolic pathways activated in fasting interact with immune responses to control tumor growth [3] Anti-PD1 treatment is effective in melanoma with high levels of A. muciniphila low levels of circulating IGF-1 sensitize tumor cells to anti PD L1 [26,31]. fasting was also associated with fewer instances of immunotoxicity and adverse events. No study has reported the effects of ketogenic diet on immunotherapy outcomes; thus, it is not clear whether the glucose limitation will affect anti-tumor immunity [62].
While intermittent fasting holds significant potential as a tool to combat cancer, its current role in clinical practice remains limited. While preliminary evidence suggests potential benefits in specific contexts, such as reducing side effects of certain treatments, more robust and conclusive data is needed. It's crucial to acknowledge the potential risks, particularly for patients at risk of malnutrition or eating disorders. Unintentional weight loss can severely impact clinical outcomes, making fasting inadvisable in such cases. As such, a personalized approach is essential. Patients with cancer should consult with a registered dietitian specializing in oncology to determine the most appropriate dietary strategy for their individual needs. Future research will undoubtedly shed lighter on the optimal implementation of fasting regimens in cancer care. Ongoing clinical trials are exploring the impact of intermittent fasting on cancer incidence, treatment response, and overall survival. By carefully considering the potential benefits and risks, we can harness the power of fasting to improve cancer outcomes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
