
Case report | DOI: https://doi.org/10.31579/2578-8868/368
1Assistant Professor, Neuroanesthesia super speciality cell, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India
2Resident, Department of Anesthesia, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India.
3Resident, Division of Neuroanesthesia under Department of Anaesthesia, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
4Resident, Department of Neurosurgery, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India.
*Corresponding Author: Kunal Kumar Sharma, Assistant Professor, Neuroanesthesia super speciality cell, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India
Citation: Kunal K. Sharma, Shoyab Aktar SM, Bharti Chauhan, Akshay Behera, (2025), Effect of Endotracheal Intubation in Lateral Decubitus Position on Intracranial Pressure in Patients Undergoing Spine Surgery- A Case Report, J. Neuroscience and Neurological Surgery, 17(4); DOI:10.31579/2578-8868/368
Copyright: © 2025, Kunal Kumar Sharma. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 06 March 2025 | Accepted: 25 March 2025 | Published: 09 April 2025
Keywords: intracranial pressure; optic nerve sheath diameter; transcranial color-coded duplex; endotracheal intubation
This case report explores the effect of endotracheal intubation in the lateral decubitus position on intracranial pressure (ICP) using non-invasive optic nerve sheath diameter (ONSD) assessment in patients undergoing spine surgery. While ICP monitoring traditionally requires invasive techniques, ONSD measurement via ultrasound has gained popularity as a reliable non-invasive tool for assessing changes in ICP.Endotracheal intubation in lateral decubitus position has been rarely described during spine surgery. This can alter venous return and intracranial dynamics, potentially affecting ICP. The present cases investigate how the combination of the lateral decubitus position and endotracheal intubation influences ONSD and subsequently ICP. Intracranial pressure is a critical factor influencing patient outcomes in neurosurgical procedures, especially in the setting of spinal surgeries that often involves peculiar positioning and airway management. Limited data exists regarding effect of endotracheal intubation in lateral decubitus position on ICP. The present case report aims to explore potential changes in ICP during this procedure and highlight the clinical implications.
Intracranial pressure (ICP) is a essential parameter that requires meticulous monitoring in patients undergoing spine surgery. The lateral decubitus position, which involves the patient being placed on their side, can alter both venous return and cerebrovascular dynamics, leading to potential modifications in ICP. Furthermore, endotracheal intubation, a standard procedure in anesthetic management, can influence respiratory mechanics, thus affecting ICP. Although the lateral decubitus position is infrequently employed for endotracheal intubation in spine surgery, we encountered two cases in which the patients were unable to tolerate the supine position due to severe back pain. These patients underwent endotracheal intubation in the lateral position, during which we monitored ICP non-invasively at pre-defined time intervals. A thorough review of the literature revealed a dearth of comprehensive data concerning the quantitative effects of lateral positioning on ICP, particularly with respect to non-invasive measurement techniques.
Historically, ICP monitoring has relied upon invasive methods, such as ventricular catheters. However, with the advent of non-invasive modalities, such as the measurement of optic nerve sheath diameter (ONSD) and transcranial color-coded duplex (TCCD) ultrasonography, there is emerging level of evidence on these techniques to estimate ICP.1,2 A known correlation exists between an increase in ONSD and elevated ICP. In the present case report, we utilized the Xing & Wang equation to calculate ICP based on ONSD measurements. Despite the clinical relevance, the influence of endotracheal intubation in the lateral decubitus position on ICP remains inadequately explored, and this case report seeks to investigate this interaction.
This case report adheres to the CARE (CAse REport) guidelines for reporting clinical case studies. Two patients with who were unable to tolerate the supine position due to severe back pain, were admitted to the neurosurgery operating room at our institute. Both patients were free from any pre-existing intracranial pathology that could contribute to elevated ICP, and they neither had any history of glaucoma or vitreous disease. Anesthetic induction was performed in accordance with the standard neuroanesthetic protocols, utilizing propofol, fentanyl, and vecuronium. The patients underwent endotracheal intubation in the lateral decubitus position, and the quality of intubation was evaluated using the Viby-Mogensen criteria3 (Figure 1). Detailed demographic data and other patient parameters are summarized in Table 1.

Figure 1: a,b,c,d depict lateral intabation with McIntosh laryngoscope blade in case 1. Whereas e,f,g,h depict lateral intubation with Videolaryngoscope in case 2
| Parameter | Case 1 | Case 2 |
| Age | 69 | 57 |
| Gender | Female | Male |
| B.M.I (body mass index) | 18 | 29 |
| Diagnosis | Pott's spine | Pseudomeningocele after MISS for D5-D6 burst compression fracture |
| Surgery | Decompressive laminectomy and biopsy | Theco-peritoneal shunt |
| Anesthetic Induction | Propofol 100 mg; Fentanyl 100 µg; Lidocard 60 mg; Vecuronium 8 mg | Propofol 140 mg; Fentanyl 100 µg; Lidocard 60 mg; Vecuronium 10 mg |
| Viby-Mogensen score (Quality of Intubation) | 13 | 14 |
| Anesthetic Maintenance | O2:Air + Isoflurane Dexmed @ 32 mcg/kg/hr | O2:N2O + Isoflurane Leviteracetam 1 g iv slow |
| ONSD baseline (cm) | 0.42 | 0.45 |
| ONSD after intubation (cm) | 0.51 | 0.53 |
| ONSD prior to positioning prone (cm) | 0.53 | 0.54 |
| ONSD after extubation in supine position (cm) | 0.45 | 0.47 |
| EtCO2 immediately after intubation | 28 | 30 |
| EtCO2 prior to positioning prone | 31 | 34 |
Table 1: Demographic parameters and intra-operative data
ONSD measurements were performed at four distinct time points: prior to intubation, immediately post-intubation in the lateral position, prior to repositioning the patients to a prone position for surgery, and after extubation in the supine position. ONSD was measured using a 2 MHz linear transducer from a Sonosite ultrasound machine, focusing on the
non-dependent orbit (Figure 2). ICP in mmH2O was calculated using the equation developed by Xing & Wang.4 A conversion factor of 0.0736 was applied to convert the ICP values from mmH2O to mmHg.
ICP = - 111.92 +77.36 x ONSD
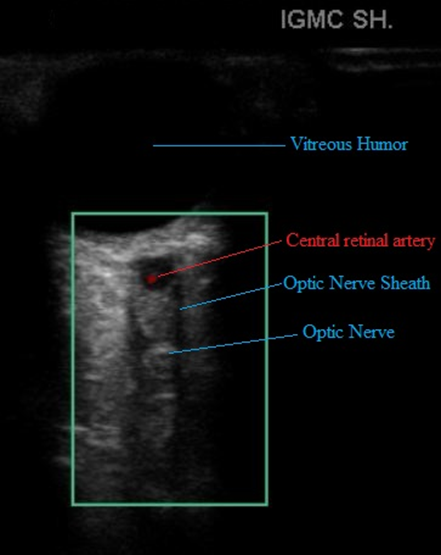
Figure 2: The Optic nerve sheath and associated sonoanatomy
Additionally, other clinical parameters were recorded at each time point, including mean arterial pressure (MAP), heart rate (HR) and peripheral oxygen saturation (SpO2).
Both patients exhibited an increase in ONSD following endotracheal intubation in the lateral decubitus position (Figure 3). However, despite the observed rise in ONSD, there were no clinical manifestations of elevated ICP, such as postoperative neurological deficits, altered mental status, or abnormal pupillary response. Additionally, there were no significant fluctuations in blood pressure or heart rate indicative of an acute intracranial event.
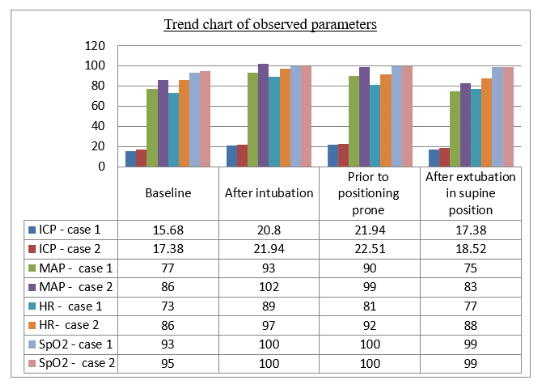
Figure 3: Trend of observed parameters
The conventional anesthetic induction agents have been extensively studied in conjunction to neuro-monitoring in the recent era.5 Even anesthetic induction algorithms with dexmeditomidine has also been evaluated in neurosurgeries.6,7 However, ICP monitoring still remains elusive in spine surgeries, especially when it is to be done under a difficult airway scenario like in present cases.
The observed increase in ICP following intubation in the lateral decubitus position may be attributed to changes in venous return and alterations in the cerebral perfusion gradient induced by the lateral positioning. The transient rise in ICP returned to baseline levels once the patients were repositioned to the supine position at the end of the anesthesia procedure for extubation. This elevation in ICP was moderate and transient, with no clinical evidence of raised ICP, such as pupillary changes or altered neurological status. Furthermore, ICP returned to normal after extubation, when the patients were positioned supine.
A cadaveric study conducted by McCormack et al. sought to quantify the effect of laryngoscopy on ICP.8 This study, which involved five adult cadaveric heads, found an increase in ICP by a mean of 5 mmHg following endotracheal intubation. However, this study's findings are limited by the small sample size and the inability to extrapolate the results to living humans due to the absence of cerebrovascular autoregulation in cadavers. Also, the intubations performed in the cadavers was in supine position, in contrast to the present study.
The lateral decubitus position is known to affect both venous return and cerebral perfusion pressure. In the present cases, the increase in ICP following intubation is likely a result of increased intracranial venous pressure, which can occur due to altered venous drainage from the brain in the lateral position. This effect may be exacerbated by the mechanical ventilation and positive pressure ventilation that accompany endotracheal intubation, both of which can influence cerebral blood flow and ICP.
Kim et al. performed a study on 13 patients undergoing craniotomy, utilizing invasive cerebral epidural catheters to monitor ICP. The study found a mean increase of 7.1 ± 7.23 mmHg in ICP during intubation.9 However, this study's patient population included individuals with intracranial pathology, which differs from our cohort of patients undergoing spine surgery with no intracranial pathology.
Endotracheal intubation with positive pressure ventilation has the potential to elevate intrathoracic pressure, thereby reducing venous return from the brain and increasing cerebral venous pressure. This effect, combined with the altered venous return caused by the lateral decubitus position, may account for the transient increase in ICP observed in this study. While a moderate increase in ICP was documented, there were no clinical signs of deterioration or neurological compromise in either patient. This suggests that the rise in ICP was clinically insignificant, though it underscores the importance of monitoring ICP in such settings.
Moss et al. observed similar trends in ICP during anesthetic induction in 20 patients scheduled for craniotomy. While a slight increase in ICP was noted, it did not reach statistical significance, and the changes were transient.10 As with the study by Kim et al., the findings are not directly applicable to our patient population, as their study cohort was composed of individuals with pre-existing intracranial pathology.
The utility of ONSD measurement as a non-invasive method to assess changes in ICP has been demonstrated in various clinical scenarios. The slight but consistent increase in ONSD following intubation and during surgery in the lateral position suggests that the positioning may lead to transient alterations in ICP. Importantly, the absence of clinical manifestations of raised ICP and the subsequent normalization of ONSD after surgery indicate that the rise in ICP was mild and temporary.
This case report demonstrates that endotracheal intubation in the lateral decubitus position during spine surgery results in a transient increase in ICP, as evidenced by the increase in optic nerve sheath diameter (ONSD). However, the observed increase in ICP was moderate, transient, and did not result in any clinical symptoms of raised ICP. Non-invasive ONSD measurement provides a reliable method for monitoring ICP changes. Although no overt clinical complications were observed, these findings suggest that continuous monitoring of ICP during spine surgery is prudent, especially in patients with pre-existing risk factors for elevated ICP. Further studies with larger patient populations are necessary to confirm these findings and refine clinical guidelines for the management of ICP in patients undergoing spine surgery in the lateral decubitus position.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
