
Research Article | DOI: https://doi.org/10.31579/2578-8965/119
1Professor of Maternity & gynecological Nursing, Faculty of Nursing, Ain Shams University, Egypt
2 Assistant Lecturer of Maternal & Newborn Health Nursing, Faculty of Nursing, Beni-Suief University.
3 Professor of obstetrics and women’s health, Faculty of Nursing, Benha University
4 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
Citation: Kamilia R. Abou-Shabana, Aml A.Hassan, Somaia R. Eid, Hanan E. Hassan (2022) Effect of CounsellingSessions on Women’s Satisfaction during Gynecological Examination. J.Obstetrics Gynecology and Reproductive Sciences 6(4); DOI: 10.31579/2578-8965/119
Copyright: © 2022, Hanan Elzeblawy Hassan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 February 2022 | Accepted: 19 March 2022 | Published: 26 April 2022
Keywords: counseling; knowledge; pain; discomfort;, satisfaction; gynecological examination
Background: Gynecological examination was а nursing concern because the nurse is expected to be beside female pre, during, and post-gynecological-examination. Nurses had very important role in preparing women before an examination.
Aim: This study was conducted to evaluate the effect of pre-gynecological-examination-counseling-session on relieving women’s pain, discomfort and enhancing their satisfaction, as well.
Setting: The study was conducted at the gynecological clinic at Beni-Suef University Hospital.
Subjects and methods:design: A quasi-experimental research design was utilized in this study (an intervention pre/post-test). Sampling: 60 women who were attended the previously mentioned study setting for the first time. Sample type: Α purposive sample. Tools: six tools of data collection were used. (I): Interviewing questionnaire; (II): Comfort and pain scale; (III): Visual analogue scale; (IV): Patients’ satisfaction questionnaire sheet; (V): Counseling interviewing sheet; (VI): An Instructional supportive brochure.
Results: there was a marked improvement in knowledge of the studied sample about gynecological examination post-implementation of an instructional supportive guideline with a highly statistically significant difference (P<0.01) between pre and post-implementation of the instructional supportive guideline. There was a positive correlation between the level of pain of the studied sample and their discomfort, satisfaction, self-reported barriers during gynecological examination, and satisfaction level post gynecological examination.
Conclusion: Counseling sessions regarding pre-gynecological examination had a positive effect on relieving women’s pain, discomfort and enhancing their satisfaction.
Recommendation: Nurse administrators must be designed, and apply a monitoring system to certain that nurses are well competent during providing pre-gynecological examination counseling sessions.
Gynecological examination procedures aim to assess the health of a woman’s reproductive system. The general examination usually makes usage of a speculum for a view of the vagina and cervix. More specialized procedures include the Pap-Smear for the detection of cancer of the cervix. In the diagnosis of possible infertility, useful procedures include Rubin’s test, which helps determine whether the fallopian tubes, the slender hollow structures through which the eggs travel from the ovaries to the uterus, are occluded; hysterosalpingography, or X-ray of the uterus and fallopian tubes after injection of a contrast medium; the evaluation of ovulation and hormonal factors by the laboratory examination of cervical and uterine tissues and by the determination of blood and urine levels of estrogenic hormones. [1-3]
Few studies have addressed patient preference concerning pelvic examinations alone, but about 45% of women reported that they would prefer a female doctor for their gynecologic care, 4.2% reported that they would prefer a male doctor, and the remaining women expressed no preference. [4-7]
The following are complaints that would warrant a gynecological exam: sexually transmitted infection testing or screening, screening exams by primary care physicians and gynecologists in females above the age of 21, pain, discharge, pregnancy or postpartum, infection, itching, swelling, bleeding, menstrual abnormalities, sexual development abnormalities, sexual or physical trauma, neurological conditions, incontinence, and pelvic floor disorders. [8-11] some clinicians combine a routine pelvic exam along with other preventative procedures like a breast examination and pap smear. [12-14]
Many burdens and effects of gynecological examination are tactile sensation, worry about getting a pelvic exam. It's very communal for fair sex to be especially disordered and upset about having their first gynecological exam; as she tones anxious or uneasy. [15, 16]
Patients will have a more positive experience if they feel that adequate time was allowed for their visit and that the practitioner was prepared to answer questions. A study of adolescents' views about their first pelvic exams showed that a positive experience was associated with a sense of control during the examination. This depended on a thorough explanation of the procedure before it was undertaken, allowing the patient to participate in decision making, and receiving assurance that the exam could be discontinued at any point. [17, 18]
Moreover, this intimate physical examination may provoke many negative feelings such as embarrassment, shame, anxiety, and awkwardness. The first pelvic examination in a women’s life and the attitude of health providers may lay the foundation for subsequent pelvic exams. [19, 20]
The nurse must recognize the women's vulnerability and assure the women of strict confidentiality. For many women, modesty and fear of the unknown make the assessment, the interview, physical examination, and particularly pelvic examination an ordeal. Many women are informed, misguided by myths, or afraid to appear stupid by asking questions about sexual and reproductive functioning. The nurse must be sensitive to this issue. [21-23]
The nurse helps women to understand the importance and benefits of using gynecological examinations types to the whole family and community. She also helps a client to understand the differences between lifesaving and death control, and to acquire knowledge about the reasons and concerns of using gynecological examinations methods. The rear many types of motivation such as talking to people about the advantages of gynecological examinations, encouraging them to talk with each other about it, using the different methods so mass media communication, giving group discussions about gynecological examinations. [24-26]
Satisfaction with the gynecological exam is one factor that motivates women to seek and continue the gynecological examination. The term 'motivation' is used to refer both to our reasons for action and to our enthusiasm for doing it. It has been defined in the psychology literature as the psychological military force or pushes that impel a person towards a specific goal [27].
Counseling is a part of communication and helping process through which an individual with special knowledge and skills, contact with a client who needs problem-solving for better adapting, deals with misconcepts, culture, and beliefs, and improve women positive response to the gynecological exam with the counselor help providing free choices and options leaving the decision making to the client to choose and decide. [16]
The aim of counseling is to free the person being counseled to live more fully and such fuller living comes through action as counseling must have a practical aim, she must encourage the women to become confident enough to choose a particular course of action and complete it. [28]
The gather model was advocated by the population communication services of john Hopkins school of hygiene and public health it has been used in many countries including Egypt. Counseling continues to take place throughout the whole screening process nurses should reinforce that negative screening result means that no evidence of cancer exists, what signs to report for further evaluation, and the interval and recommendation for further screening as well as the importance of follow-up visit. [15]
Pre-gynecological examination-counseling is a wonderful twentieth-century invention. We live in a complex, busy, changing world. In this world, there are many different types of experiences that are difficult for women to cope with. Most of the time, women get on with life, but sometimes women are stopped in their tracks by an event or situation that they do not, at that moment, have the resources to sort them. Most of the time, women may find ways of dealing with gynecological problems in living by talking to health care workers, or their family doctor. But occasionally their advice is not sufficient, or we are too embarrassed or ashamed to tell them what is bothering us, or we just do not have an appropriate person to turn to. [29-31]
Pre-gynecological examination Counseling is a really useful option at these moments. In most places, pre-gynecological examination counseling is available fairly quickly and costs little or nothing. The gynecological nurse does not diagnose or label the woman but does her best to listen to the woman and work with her to find the best ways to understand and resolve her gynecological problem. [11,32,33]
The gynecological examination was а nursing concern because the nurse is expected to be beside female pre, during, and post gynecological examination, the nurse had а very important role in preparing women before an examination. Additionally, preparing equipment, women during an examination, instructing women about comfort and suitable position for gynecological examination, instructing women about laboratory investigation, medical treatment as well as follow up visits to the clinic to enhance women positive response to attend regularly to the gynecological clinic. [22,33]
Gynecological examination (Gyne. Ex.) is any procedure performed to the female al exam genital tract where an instrument, is inserted directly into the vagina. [18]
Counseling is a purposeful relationship between two people, who approach a mutually defined problem with mutual consideration of each of them to the end that the troubled one or less mature is aided to a self-determined resolution of his problem. [20]
This study was conducted to evaluate the effect of pre-gynecological examination counseling sessions on relieving women’s pain, discomfort and enhancing their satisfaction as well.
4.1. Design: A quasi-experimental research design was utilized in this study (an intervention pre/post-test)
4.2. Setting: The study was conducted at the gynecological clinic at Beni-Sued University Hospital.
4.3. Sampling:
4.4Tools of data collection: Six tools were utilized in this research as the following:
4.4.1. The first tool was interviewing questionnaire: It was included two parts:

The first part: To assess female general characteristics (age, occupation, residence, education, and marital status).The second part: To assess women’s knowledge regarding gynecological examination (definition, Importance, time, indication, preparation, ways, equipment, contraindications,Etc)
The scoring system for or evaluating women’s knowledge was developed as the following: Knowledge was scored as a correct and incorrect answer for each knowledge question. Each question was given 1 score for the correct answer and 0 scores for an incorrect answer. The total knowledge of more than 60 % will be correct and less than satisfactory level of knowledge and less than 60 % will be unsatisfactory level of knowledge.
4.4.2 The second tool: Comfort and pain scale [34]
A standardized tool for assessing women's comfort was utilized during gynecological examination. Updated by Erica Jacques (2019) it was included eight items (Alertness, Calmness, Crying, Physical movement, Muscle tone, Facial tension, Blood pressure, Heart rate) upon each (1-3).
The scoring system was three Likert scales from 1 to 3 score in front of each statement the woman responds 1, 2, 3 scores. The total score was 8-16 indicate comfort and (17-24) indicates discomfort.
4.4.3 The third tool: The visual analogue scale to assess pain level [35]
Α Visual Analogue Scale (VΑS) is a measurement instrument that tries to measure a characteristic or attitude that is believed to range across а continuum of values and cannot easily be directly measured. It is usually a horizontal line, 100 mm in length, anchored by word descriptors at each end, as illustrated in the figure below.
The level of pain associated with gynecological procedures was measured by asking the participants to place а line perpendicular to the VΑS line at the point that best indicates their pain at the present time. The score was considered as the following: 0=no pain, 1-3=mild pain 4-6=moderate pain, 7-10=sever pain.
4.4.4 The fourth tool: Patients’ satisfaction questionnaire sheet. Albashayeh et al. (2019) [36]
This tool was utilized for two groups Post gynecological examination. This tool was adopted from Albashayeh et al. (2019). It was included 13 statements and modified by the researcher upon each statement patients’ responded to.
The scoring system was utilized, two Likert scales (1=dissatisfied and 2 =satisfied). The total score of satisfaction was 26. Satisfy ≥ 60% (that mean ≥16 score), and Dissatisfy < 60>
4.4.5 The fourth tool: Self-reported barriers
Barriers that facing women during the gynecological examination as self-reported barriers by the women designed by the researcher; included five statements upon each statement the participant respond yes or no post-intervention.
The scoring system was utilized, two Likert scales (0=no and 1=yes). The total score of self-reported barriers was 6.
4.4.6 The fifth tool: Counseling interviewing sheet (Rinehart et al. (1999) [36]
Counseling interviewing sheet following gathering model of counseling (GATHER approach to counseling about gynecological examination adapted from Rinehart et al. (1999) including the following parts:
Part I: G: great the patient and A: asking about the following general characteristics: (Age, name, area of residence, education level, and marital status)
Part II: T: Telling patient; Orientation about gynecological examination clinic, position during the gynecological examination, about equipment will be utilized, types of gynecological examinations, the importance of gynecological examination, advantages, and disadvantages of gynecological examinations)
Part III: H: helping women to:
Part IV: E: explaining for women
Part V: R: Referral: Give the patient follow up card including the following
This tool will be used pre-gynecological examinations, and immediately after the post-gynecological examination.
4.4.7 The sixth tool: An Instructional supportive brochure
An instructional supportive brochure was designed and distributed among women at the end of the counseling session to enhance their comfort and satisfaction. The brochure includes the definition of gynecological examination, position during the gynecological examination, equipment that will be utilized, types of gynecological examinations, and the importance of gynecological examination, advantages, and disadvantages of gynecological examinations.
4.5. Validity of the tools:
All tools of data collection were sent to three specialized University Professors, according to their comments modifications were considered.
4.6. Ethical considerations:
A letter of approval to conduct the study was obtained from the dean of faculty of nursing at Benha University. Then approval from the ethical research committee at Benha faculty of nursing was obtained to conduct the study. Another letter of approval for Beni-Suef University Maternity Hospital director included the title and the aim of the study. Informed consent was obtained from each participant in the study; the aim of the study was explained before starting the study for each participant. Each participant had the right to withdraw from the study at any time. The tools of data collection were not touching the participant’s dignity, culture, and ethical issues. The participant was interviewed individually in a private room. After data collection and statistical analysis, all tools of data collection were burned to maintain the confidentiality of the study.
4.7. Fieldwork: The study was conducted through three phases:
4.8. Statistical design: Data were analyzed using a statistical program for social science (SPSS) version 20.0. Quantitative data were expressed as mean±SD). Qualitative data were expressed as frequency and percentage, T-test was used. P-value>0.05; Not significant (NS), P-value≤0.05; Significant (S), P-value≤0.01; Highly Significant (HS).
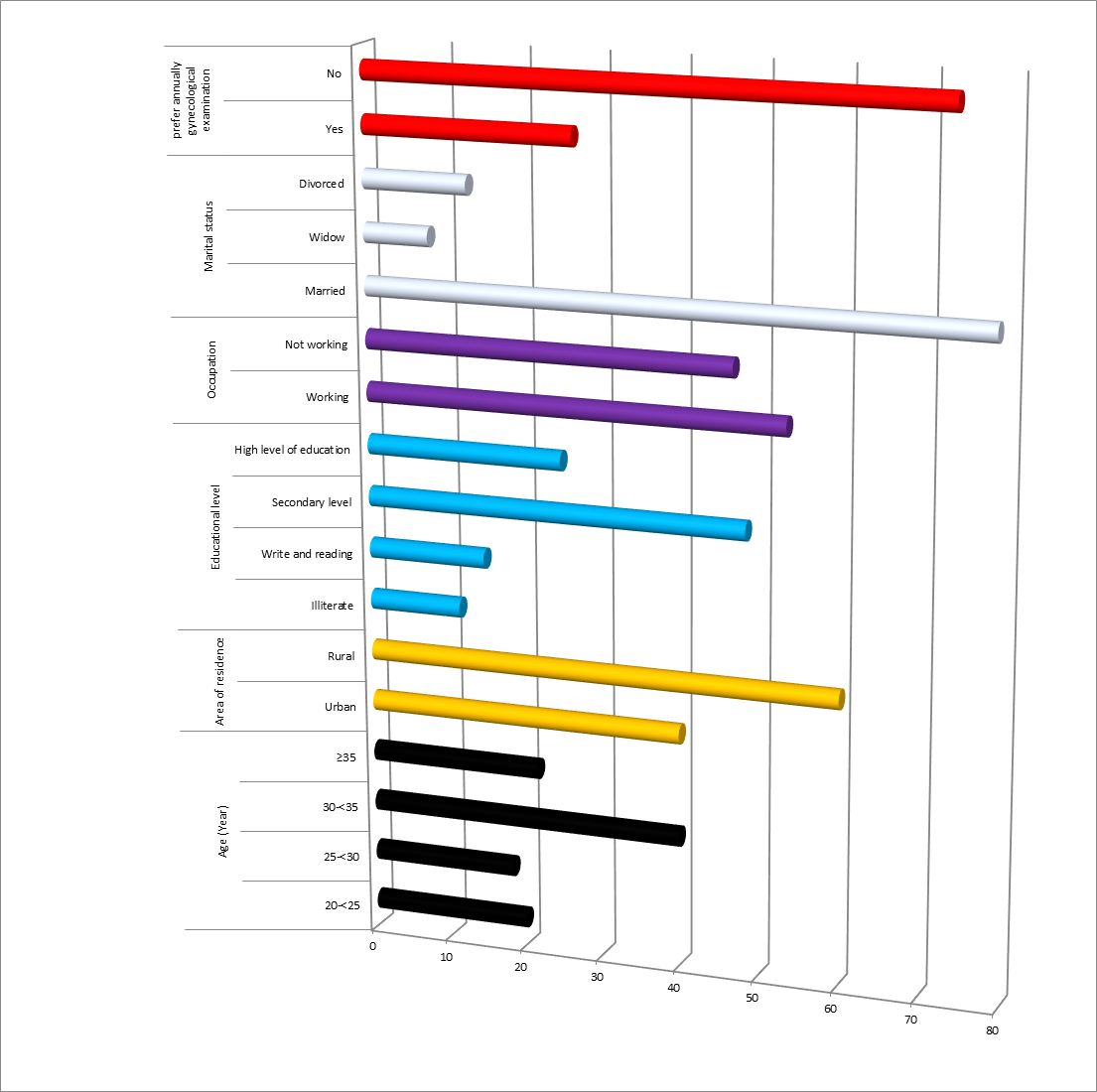
Figure (1) presented that 40% of the studied sample their age was 30-<35>
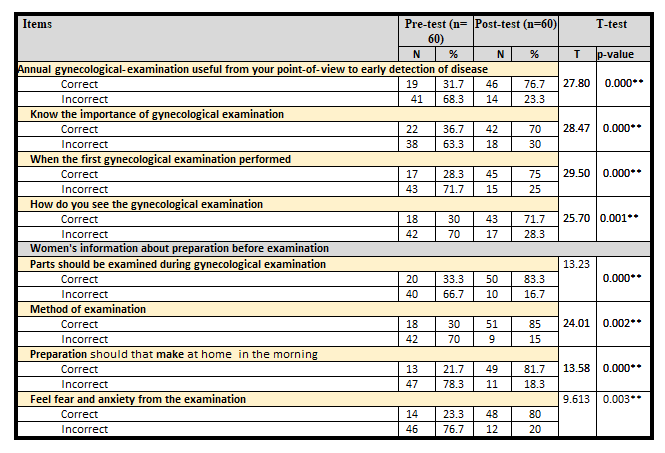
Table (1) revealed that there was a marked improvement in knowledge of the studied sample about gynecological examination post-implementation of an instructional supportive guideline with highly statistically significant difference (P<0>
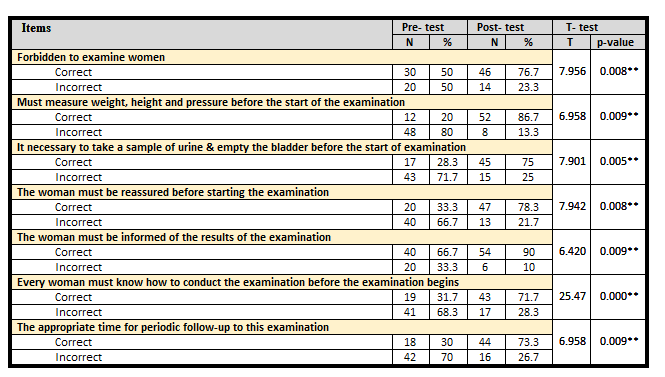
Table (2) demonstrated that there was a marked improvement in knowledge of the studied sample about pre-gynecological -examination procedures post-implementation of an instructional supportive guideline with highly statistically significant difference (P<0>
Table (3) showed that there was a marked improvement in total knowledge of the studied sample about gynecological examination post-implementation of an instructional supportive guideline with highly statistically significant difference (P<0>
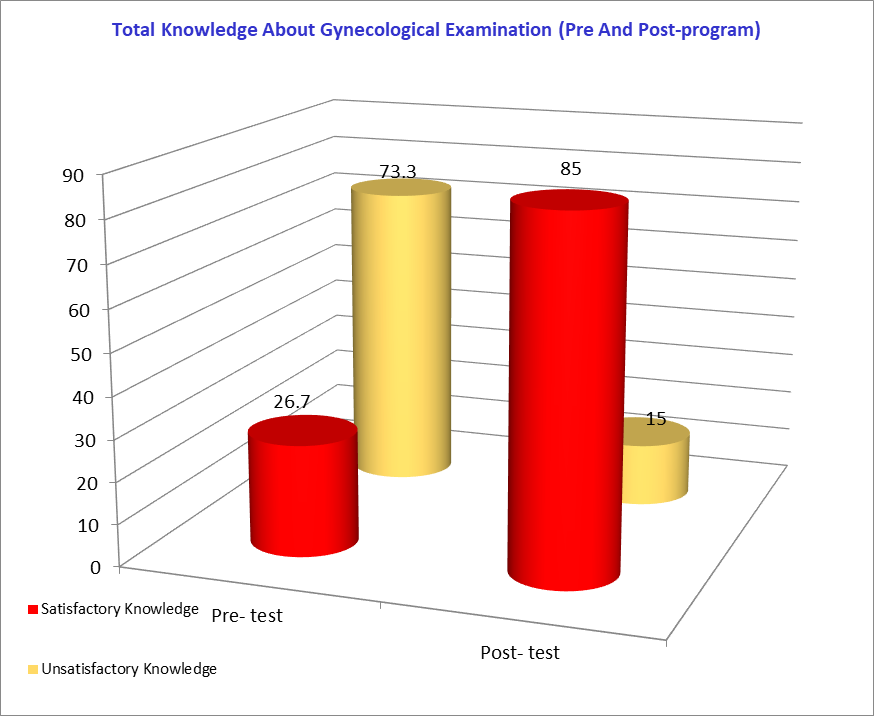
Figure (2) illustrated that (73.3%) of the studied sample had unsatisfactory knowledge about gynecological examination at pre-implementation of an instructional supportive guideline. While, (85%) of them had satisfactory knowledge about gynecological examination at post-implementation of an instructional supportive guideline, respectively.
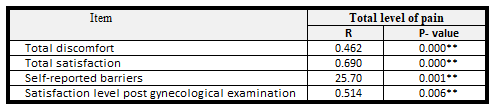
Table (4) revealed that there was a positive correlation between the level of pain of the studied sample and their discomfort and satisfaction, as well, during the gynecological examination and their satisfaction post gynecological examination, (p=0.000). The same table demonstrated that there was a positive correlation between levels of pain of the studied sample and self-reported barriers during gynecological examination (p=0.001). Moreover, there was a positive correlation between levels of discomfort during gynecological examination and satisfaction level post gynecological examination (p=0.006).

Pre-gynecological counseling is very important. It aims to help an women to help herself to overcome her gynecological problem, Counseling is The process that occurs when a women and gynecological nurse set aside time to explore difficulties which may include the stressful or emotional feelings of the women. The act of helping the women to see things more clearly, possibly from a different view-point can enable the women to focus on feelings, experiences or behavior, with a goal of facilitating positive change, and a relationship of trust. Confidentiality is paramount to successful counseling. Professional gynecological nurse will usually explain their policy on confidentiality. They may, however, be required by law to disclose information if they believe that there is a risk to life. [37,38]
Gynecological examination is one of the physical examinations which are essential for assessing the female (internal & external) reproductive system. In Egyptian, there are many traditions and concepts related to the gynecological examination. Some women were usually in а culture rejecting to perform any gynecological examination for the first time. They pay little attention and may absolutely refuse gynecologist counseling for а female reproductive system. So, when the women face this exam, they become very anxious, stressed, and fearing from а situation, because she considered it is immoral issues to expose her intimate part to another person. So, it was important to assess their response regarding their first gynecological examination. [20,22]
The aim of the present study was to evaluate the effect of pre-gynecological examination counseling sessions on relieving women's pain, discomfort and enhancing their satisfaction, the aim was significantly approved within the framework through the present study hypothesis which was "application of pre-gynecological examination counseling will minimize pain discomfort and maximize patient satisfaction, the women who attend pre-gynecological examination counseling sessions will be will be expected to improve their pain level and discomfort and enhancing their satisfaction" this hypothesis was significantly achieved from the present study research finding. It was observed in the present study that there was a marked improvement in knowledge of the studied sample about gynecological examination procedure post-intervention with a highly statistically significant difference at (pless than0.01) between pre and post-intervention. the majority of the studied sample (78.3%) had incorrect knowledge about preparation for gynecological examination pre-intervention incomparable with Eid et al., (2019) who reported that more than half among the studied sample had incorrect knowledge regarding the meaning of gynecological examination. [22] The majority of the studied sample had incorrect knowledge regarding the technique of gynecological examination may be due to reproductive health illiteracy among Egyptian females, so present study research stated that increasing knowledge about gynecological examination was one factor that motivated women to seek and continue the gynecological exam. Even so providing, good communication, active interaction can assist in decreasing barriers and clarifying any misconception, and even so, this improves knowledge.
In the current study, It was observed that the majority among studied sample had incorrect knowledge regarding meaning, importance, parts of the gynecological examination, and there was a marked improvement in knowledge of the studied sample about gynecological examination post-implementation of an instructional supportive guideline with a highly statistically significant difference at (P less than0.01) between pre and post-implementation of an instructional supportive guideline, this agrees with Hassan et al. (2018) who had revealed that majority among the present studied sample had incorrect knowledge concerning definition, importance, complication & preparation. [39] Similarly, Freyens et al. (2017) reported that the majority of women in Egypt had incorrect knowledge regarding reproductive issues because culture and tradition prevent them from discussing these issues of reproductive and gynecological health. [40] However, this disagrees with Norrell et al. (2016) who found that approximately one-half of the participants stated that they knew the examination's purpose. [41]
In the current study, there was a marked improvement in knowledge of the studied sample about pre-gynecological-examination procedures post-implementation of an instructional supportive guideline with a highly statistically significant difference at (Pless than0.01) between pre and post implementation of an instructional supportive guideline. Hassan et al. (2013) reported that the scores of all skills were higher compared to the pretest, reaching statistically significant differences in the skills of determining material usefulness, applying the information to individual cases, disseminating new ideas about care to colleagues, and reviewing own practice. The total score increased from 4.3 to 4.9 although the difference did not reach statistical significance (p=0.13). [39] Moreover, Hilden et al. (2003) stated that most women felt emotional discomfort regarding the gynecologic examination. [42]
In the present patients, there was a highly statistically significant relationship between the total knowledge of the studied sample about gynecological examination at the post of an instructional supportive guideline and their education level at (P less than0.01).
In the current study, there was a positive correlation between the level of pain of the studied sample and their discomfort during the gynecological examination and their satisfaction post-gynecological examination. There was a positive correlation between levels of pain of the studied sample and self-reported barriers during the gynecological examination and there was a positive correlation between levels of discomfort during gynecological examination and satisfaction level post gynecological examination. This agrees with Güneş and Karaçam, (2017) reported a positive correlation between discomfort during vaginal examinations and emotional violence and post-traumatic stress disorder but a negative correlation between discomfort during vaginal examinations and the number of live births. [43].
Finally, pre-gynecological-examination-counseling had an important effect on relieving women's pain, discomfort and enhancing their satisfaction. Some of the different effects that are espoused either explicitly or implicitly by counselors are listed, Insight. The acquisition of an understanding of the origins and development of emotional difficulties helping women to increase capacity to take rational control over feelings and actions relating with others helping women to become better able to form and maintain meaningful and satisfying relationships with other people: for example, health care workers within the examination room. Self-awareness helps women to become more aware of thoughts and feelings that had been blocked off or denied, or develop a more accurate sense of how the self is perceived by health workers. Self-acceptance is the development of a positive attitude towards self, marked by an ability to acknowledge areas of experience that had been the subject of self-criticism and rejection.
Based on the result of the present study the following can be concluded: The present study concluded that counseling sessions regarding pre-gynecological examination had a positive effect on relieving women’s pain, discomfort and enhancing their satisfaction so the hypothesis was supported and accepted, and the study aim was achieved.
1- Reapplication of the present study intervention in another setting and on another sample.
2- Nurse administrators must design and apply monitoring systems to certain that nurses are well competent during providing pre-gynecological examination counseling sessions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
