
Research Article | DOI: https://doi.org/10.31579/2766-2314/043
1 Department of Physiology, Faculty of Medicine, Sabratha University, Libya.
2 PhD Researcher at Biochemistry, Memorial University, Canada.
3 Department of Medical Laboratory, Faculty of Medical Technology, Sabratha University, Surman, Libya.
4 Faculty of Science, Zawia University, Western Libya.
5 Researcher at National Center for Disease Control, Libya
*Corresponding Author: Azab Elsayed Azab, Department of Physiology, Faculty of Medicine, Sabratha University, Libya.
Citation: Azab E. Azab, Alawaini K., Kushlaf N., Ashraf M. Albakoush, Abdalla S., and Mohamed S. (2021) Effect of Coronavirus Infection on Fasting Blood Glucose, Kidney Function, and Electrolytes in COVID-19 Patients in the Zawia Region, Western Libya. J, Biotechnology and Bioprocessing 2(4); DOI: 10.31579/2766-2314/043
Copyright: © 2021, Azab Elsayed Azab, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 May 2021 | Accepted: 20 May 2021 | Published: 28 May 2021
Keywords: COVID-19, coronavirus, fasting blood glucose, kidney function, electrolytes, zawia region, western libya
Background: Coronavirus disease 19 (COVID-19) is a pandemic infectious disease caused by the novel coronavirus. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). It is an aggressive virus that spread worldwide and is a systemic disease involving multiple systems, including respiratory, cardiovascular, gastrointestinal, hematopoietic, neurological, immune, and urinogenital systems.
Objectives: The present study aimed to evaluate the alteration in fasting blood glucose, serum urea, creatinine, Na+, K+, and Cl- levels among COVID-19 patients in the Zawia region, Western Libya.
Materials and Methods: 416 confirmed COVID-19 patients hospitalized in the Isolation Centre located in Zawia city, Libya. From the 1st May 2020 to the 30th March 2021, were enrolled in this prospective study. Covid-19 patients were defined as positive cases after the detection of SARS-CoV-2 RNA in oro-nasopharyngeal swab samples. Demographic data were extracted from electronic medical records and patient files. Also, 30 healthy individuals without any chronic disease or respiratory symptoms were recruited for the control group. Blood samples were collected via vein puncture for estimating biochemical parameters (fasting blood glucose, serum urea, creatinine, Na+, K+, and Cl- concentrations). The statistical significance of differences between groups was evaluated with the Mann- Whitney (U test). Associations between different parameters were evaluated with the Spearman's test.
Results: The results showed that coronavirus infection induced a significant increase in fasting blood glucose, serum urea, and creatinine concentrations. Infections also induced a decrease in serum sodium ion concentration, compared with healthy individuals. Seventy-six percent of corona virus-infected patients had hyperglycemia. Similarly, high levels of serum urea, creatinine, Cl-, Na+, and K+ were found in 40.9%, 39.9%, 27.9%, 8.9% and 6.5% of patients, respectively. Hyponatraemia, hypokalaemia, and hypochloremia were found in 35.5%, 13.7%, and 12.9% of patients. There were recorded a significant positive association between fasting blood glucose and serum urea, creatinine, and K+ concentration, between serum urea concentration and serum creatinine, K+, and Cl- concentrations, between serum creatinine and K+, and Cl- concentrations, and between serum Na+ and Cl- concentration, and a significant negative association between fasting blood glucose and serum Na+ and Cl- concentrations and between serum K+ and Na+ concentrations.
Conclusion: It can be concluded that coronavirus infections induced increases in fasting blood glucose, serum urea, and creatinine, and a decrease in Na+ concentrations. There was a significant association between different parameters. These biochemical changes may help the clinicians to understand COVID-19 better and provide more clinical treatment options and prevent the serious complications of the disease. Thus, clinicians should pay special attention to fasting blood glucose, kidney function and electrolyte status of COVID-19 patients. Changes in fasting blood glucose, kidney function, and electrolyte levels can be a good indicator of disease progression.
Coronavirus disease 19 (COVID-19) is a pandemic infectious disease caused by the novel coronavirus Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Old age and comorbidities, including diabetes, are associated with a more severe course and a higher fatality rate [1]. Since March 6, 2021, over 115 million cases have been reported globally, with more than 2 million deaths [2, 3]. The global pandemic secondary to the SARS-CoV-2 is leading to unprecedented global morbidity and mortality. Common symptoms include cough (50%), fever (43% of patients), and dyspnea (29%) but other features such as diarrhea (19%), myalgia (36%), hypogeusia, and anosmia (10%) are also common [4, 5].
The coronavirus disease 2019 is an aggressive virus that spread worldwide and caused a pandemic infection. It is a systemic disease involving multiple systems, including the respiratory, cardiovascular, gastrointestinal, hematopoietic, neurological, and immune systems. The urinogenital system is also affected by the disease and its complications [3, 6-8].
Hyperglycemia can occur in diabetic and non-diabetic patients hospitalized for COVID-19 and is common among acute hospital admissions and critically ill patients, encompassing those with no previous history of hyperglycemia [9-11].Also,Wang et al. [12] indicated that the level of fasting blood glucose at the time of admission is a significant prognostic factor for COVID-19. The meta-analysis carried out by Chen et al. [13] provides evidence that severe COVID-19 is associated with increased blood glucose. This finding highlights the need to effectively monitor blood glucose to improve prognosis in patients infected with COVID-19. Also, previous studies were suggested that uncontrolled hyperglycemia causes an increase in length of hospitalization and mortality caused by SARS-CoV-2 infection [14, 15].
The kidneys have a wide range of roles, including urine formation, hormone secretion, blood pressure regulation, acid-base balance, and osmolality regulation, so their normal function is essential [3, 16]. They play an essential role in maintaining fluid and electrolyte balance in the body. Disturbance to their functioning can lead to an imbalance of fluid and electrolytes. Impaired fluid and electrolyte balance can be dangerous if left unchecked [3]. Recently, the novel COVID-19 has attracted the attention of scientists where it has a high mortality rate among older adults and individuals suffering from chronic diseases, such as chronic kidney diseases [17]. Recent reports indicate that renal impairment is more common in patients with COVID-19 [3, 18-20]. In previous reports, the incidence of acute kidney injury (AKI) in patients with COVID-19 ranged widely from 0 to 36.6% [21-25]. Coronavirus enters the cell by binding to the angiotensin-converting enzyme 2 (ACE2) receptors [3, 26, 27]. Due to the high level of these receptors in kidney cells, the kidneys are not immune to coronavirus invasion [3]. The kidney's involvement with pathogens can disrupt a wide range of body mechanisms and cause many problems such as fluid and electrolyte imbalances. Therefore, monitoring renal function can prevent severe complications in patients involved with COVID-19 and operates an essential role in reducing mortality [3, 28].
The most common renal complication in COVID-19 hospitalized patients is electrolyte disorders [3, 28-30]. Various clinical and histopathological studies have demonstrated evidence of hypokalaemia, hyponatraemia, the syndrome of inappropriate antidiuretic hormone (SIADH), incomplete Fanconi syndrome, and tubulopathy in patients with SARS-CoV-2 infection [5]. Studies on COVID-19 confirm electrolyte disturbances in patients, including sodium, potassium, chlorine, and calcium imbalances [3, 19, 31]. Also, the results of Sarvazad et al. [15] study showed that hyponatraemia was more common in outpatients than in severe patients. However, all cases of hypernatraemia were observed in patients with severe disease. Electrolyte imbalances lead to cardiovascular and renal involvement [15, 32]. Because many electrolyte disorders have significant consequences to help identify the pathophysiological mechanisms underlying COVID-19 and patient management, they can provide new therapeutic opportunities [3, 29].
The present study aimed to evaluate the alteration in fasting blood glucose, serum urea, creatinine, Na+, K+, and Cl- levels among COVID-19 patients in the Zawia region, Western Libya.
Materials and Methods
416 confirmed COVID-19 patients hospitalized in the Isolation Centre located in Zawia city, Libya, from the 1st May 2020 to the 30th March 2021, were enrolled in this prospective study. Covid-19 patients were defined as positive cases after the detection of SARS-CoV-2 RNA in oro-nasopharyngeal swab samples. This study was approved by the Research and Ethical Committee of the Faculty of Medical Technology, Sabratha University. Demographic data were extracted from electronic medical records and patient files. Also, 30 healthy individuals without any chronic disease or respiratory symptoms were recruited for the control group. Blood samples were collected by vein puncture 5 ml of venous blood withdrawn from each participant in the study by using disposable syringes under an aseptic technique; they then transferred to a sterile tube for estimating biochemical parameters.
Fasting blood glucose, serum urea, creatinine, Na+, K+, and Cl- concentrations were determined using automated COBAS E411 and INTEGRA 400 machines in the Zawia Isolation Centre laboratory.
Continuous variables were presented as medians (interquartile range [IQR]); categorical variables were presented as counts (%). The data were analyzed using Graph Pad Prism software version .7. The Kolmogorov-Smirnov test was used to assess the normality of the distribution of continuous variables. The statistical significance of differences between COVID-19 patients and healthy individuals groups was evaluated with the Mann-Whitney (U test). Associations between the different parameters were evaluated with the Spearman's test. A P-value of <0>was used to establish statistical significance.
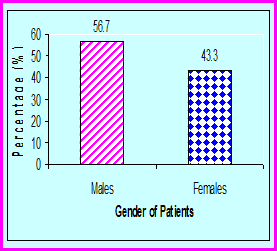
Four hundred and sixteen confirmed COVID-19 patients, 236 males (56.7%) and 180 females (43.3%) were included in the current study (Figure. 1).
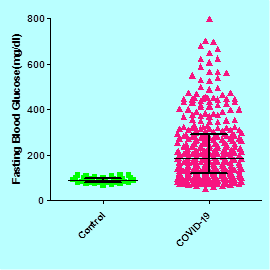
The results in table.1 and figure .2 show that patients with COVID-19 had a significant (P< 0>
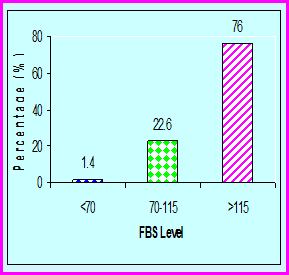
The results in table.2 and figure.3 show the percentages of corona virus infected patients with normoglycemia [(70-115) mg/dl] were 22.6%, hypoglycemia (<70>115 mg/dl) were 76%.
The results in table.1 and figure .4 show that patients with COVID-19 had a significant (P< 0>
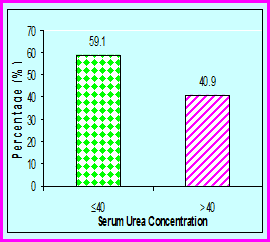
The percentages of corona virus infected patients with normal serum urea concentration (≤40 mg/dl) were 59.1%, and with uremia (>40 mg/dl) were 40.9% (Table. 2 & Figure.5).

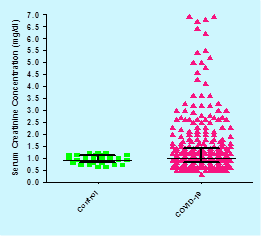
Data in table.1 and figure .6 show that patients with COVID-19 had a significant (P= 0.0223) increase in serum creatinine concentration [(median (IQR) mg/dl], 1 (0.8-1.7) compared with the healthy individuals 0.9 (0.8-1.1).
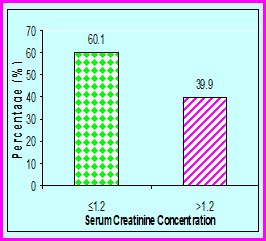
The percentages of corona virus infected patients with normal serum creatinine concentration (≤1.2 mg/dl) were 60.1%, and with high serum creatinine concentration (>1.2 mg/dl) were 39.9% (Table. 2 & Figure. 7).
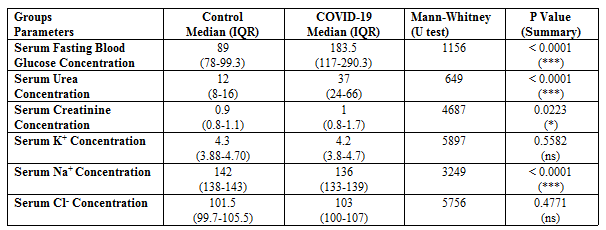
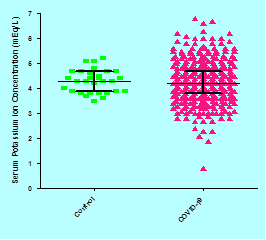
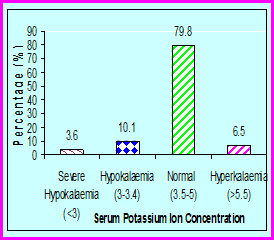
Data in table.1 and figure .8 show that patients with COVID-19 had a none significant (P= 0.5582) changes in serum potassium ion concentration [(median (IQR) mEq/L)], 4.2 (3.8-4.7) compared with the healthy individuals 4.3 (3.88-4.70).
The percentages of corona virus infected patients with hypokalaemia (<3>5.5 mEq/L) were 6.5% (Table. 2 & Figure. 9).
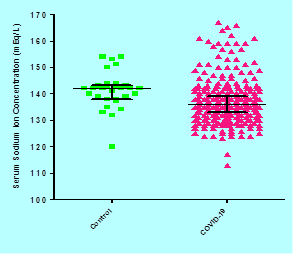
Data in table.1 and figure .10 show that patients with COVID-19 had a significant (P<0>
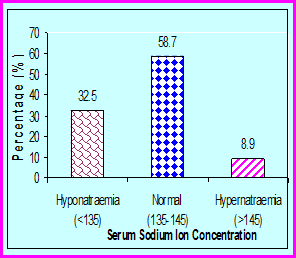
The percentages of corona virus infected patients with hyponatraemia (<135mEq>145mEq/L) were 8.9% (Table. 2 & Figure. 11).
Data in table.1 and figure .12 show that patients with COVID-19 had a none significant (P= 0.4771) changes in serum chloride ion concentration [(median (IQR) mEq/L)], 103 (100-107) compared with the healthy individuals 101.5 (99.7-105.5).
The percentages of corona virus infected patients with hypochloremia (<98mEq>106mEq/L) were 27.9% (Table. 2 & Figure. 13).

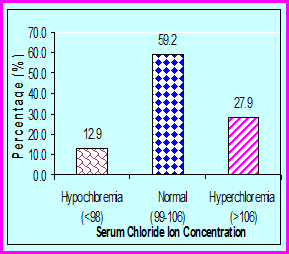
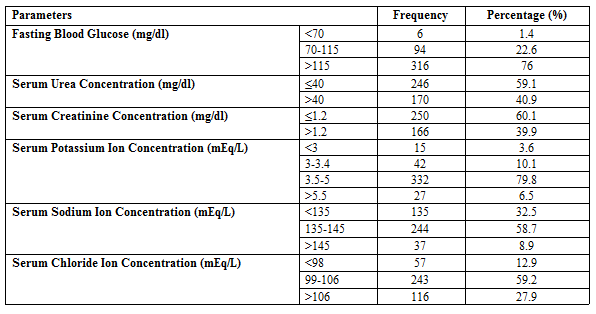
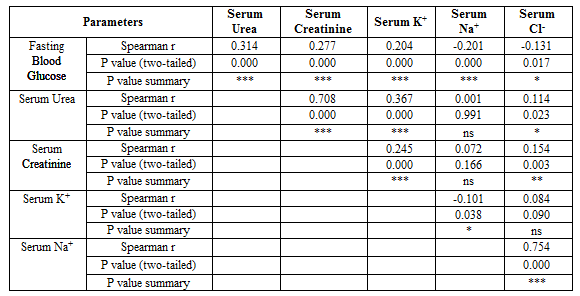
Table 3 shows a significant positive association between fasting blood glucose& serum urea, creatinine, and K+ concentration, between serum urea concentration& serum creatinine, K+, and Cl- concentrations, between serum creatinine and K+, and Cl- concentrations, and between serum Na+ and Cl- concentration. The same table show a significant negative association between fasting blood glucose and serum Na+ and Cl- concentrations and between serum K+ and Na+ concentrations, and a none significant association between serum urea and Na+ concentrations, between creatinine and Na+ concentrations, and between serum K+ and Cl- concentrations.
Hyperglycemia can result from related conditions such as severe sepsis, systemic inflammatory response syndrome, and traumatic brain injury. The initial response to these conditions is an increase in cytokines, accompanied by high levels of blood glucose. It has been shown that there is a association between glucose blood levels and morbidity/mortality of patients [15, 33, 34]. McGuinness [35] reported that infection leads to profound alterations in whole-body metabolism, including protein, glucose, and fat. Also, people with diabetes have higher risks of various infections [36]. Therefore, these diabetic patients might be at increased risk of COVID-19 and have a poorer prognosis [36]. Studies of risk factors for the mortality and morbidity of community-acquired pneumonia, SARS, and Middle East respiratory syndrome have shown that hyperglycemia and/or diabetes are involved [15, 37].
The present study showed that coronavirus infection induced a significant increase in fasting blood glucose levels in patients. The percentages of corona virus-infected patients with hyperglycemia were 76%. These results agree with the results of the previous studies [11, 12, 14, 15, 28]. Sarvazad et al. [15] found that from all included COVID-19 patients, 49.1% hyperglycemia were observed. There was a statistically significant difference between the outpatient and ICU groups in terms of FASTING BLOOD GLUCOSE (p < 0>Sarduet al. [11]recorded that 57.6% of COVID-19 patients were normoglycemic, and 42.4% were hyperglycemic. At baseline, IL-6 and D-dimer levels were significantly higher in the hyperglycemic group than in the normoglycemic group (P < 0>et al. [42] reported that the pancreas could be the target of coronavirus attack since SARS-CoV was detected in the pancreas. Also, Yang et al. [41] found that SARS-CoV damaged the endocrine part of the pancreas, indicating that SARS-CoV may cause acute insulin-dependent diabetes mellitus.
The prevalence of mild to moderate chronic kidney disease (CKD) in older patients with established diabetes (aged ≥65 years) ranges from 35% to 40% (38, 43]. CKD is associated with an increased risk for pneumonia and pneumonia-related mortality [38, 44, 45]. In severely affected COVID-19 patients, associated hypoxaemia, heart involvement (e.g. acute myocardial infarction, myocarditis, shock, exacerbation of heart failure, and arrhythmia), cardiovascular instability, and endothelial injury may also contribute to kidney injury, in what is considered a brand new cardiorenal syndrome [7, 46]. In addition to direct virus infection, kidney injury may result from the systemic response to infection or damage to other organs. While most commonly manifested as acute kidney injury, other forms of kidney injury and electrolyte abnormalities have been described [7]. Recent studies have shown that the prevalence of renal failure upon admission and the progression of acute kidney injury during hospitalization of COVID-19 patients was high, which was associated with increased in patient mortality [17, 21]. In COVID-19, the kidney and GIT are at risk, and a variety of complications have been reported that are very common [3, 47, 48]. Fluid and electrolyte disturbances are complications of kidney and GIT injuries in COVID-19 patients. Fluid and electrolyte disturbances can lead to many problems and even death. As such, clinicians should monitor fluid and electrolyte balance in COVID-19 patients, especially in patients under intensive care who are at elevated risk of fluid and electrolyte disturbance [3, 49].
The results of the current study showed that coronavirus infection induced a significant increase in serum urea and creatinine concentrations, and a decrease in serum Na+ concentration in COVID-19 patients. The percentages of coronavirus-infected patients with high levels of serum urea, and creatinine were 40.9%, and 39.9%, respectively, and with hyponatraemia, hypokalaemia, and hypochloremia were 35.5%, 13.7%& 12.9%, respectively. Our results are similar to previous studies [7, 15, 17, 19, 21, 29, 31, 50-54]. Sarvazad et al. [15] found that from all included COVID-19 patients, 38% hyponatremia, and 7.3% hypokalemia were observed. Unlike the mean of age and the level of K+, there was a statistically significant difference between the outpatient and ICU groups in terms of Na+ (p<0>Moreno et al. [52] described 306 COVID-19 patients in Spain with potassium measured in the first 72 h of admission. They found that hypokalemia was independently associated with requiring invasive mechanical ventilation, but mortality was not influenced by low potassium. De Carvalho et al. [54] carried out a case-control study in three hospitals in France, including adult patients visiting the emergency department (ED) (≥ 18 years old). A total of 594 ED case-patients in whom infection with COVID-19 was confirmed were matched to 594 non-COVID-19 ED patients (controls) from the same period, according to sex and age. Hyponatremia was defined by sodium of less than 135 mmol/L (reference range 135–145 mmol/L), hypokalemia by potassium of less than 3.5 mmol/L (reference range 3.5–5.0 mmol/L), and hypochloremia by chloride of less than 95 mmol/L (reference range 98–108 mmol/L). Hyponatremia was more common among case-patients than among controls, as was hypokalemia and hypochloremia [54]. In a study including one hundred seventy-five COVID-19 patients, 18% were classified as having severe hypokalemia, 37% had hypokalemia, and 46% had normokalemia [55].
Carriazo et al. [7] reported that hyponatraemia is common in COVID-19 patients. The cause appears to be outside the kidneys as the occurrence of the syndrome of inappropriate antidiuretic hormone has been well characterized by Ravioli et al. [56]. Also, hyponatraemia was found in 8% of patients with community-acquired pneumonia, with nearly half of the cases having SIADH [57]. Also, hyponatraemia has been reported in COVID-19 [15, 19, 31, 53, 58]. In a retrospective study conducted by Zhang et al. [53], the association between hyponatraemia and the severity of COVID-19 was considered. In a review study of electrolyte imbalances in patients with COVID-19, five studies were identified with a total of 1415 participants, indicating a relationship between decreased blood sodium and disease severity [15, 29]. Pourfridoni et al. [3] reported that the coronavirus infects the host by binding to the ACE2 receptors. Due to the presence of ACE2 receptors in the kidneys and gastrointestinal tract (GIT), kidneys, and GIT, damage arising from the virus can be seen in patients and can cause acute kidney injury (AKI) and digestive problems for the patient. Increased ACE2 leading to direct viral invasion along with hypercoagulation could explain the high risk of acute kidney injury in patients with COVID-19 even without the preexisting renal disease [38]. As one of the expression sites of the ACE2 receptor is in the proximal tubule [15, 59], hyponatraemia can occur due to increased expression of the ACE2 receptor in the proximal tubule. In an individual with severe hyponatraemia, it was shown that SARS-CoV-2 causes a syndrome of inappropriate secretion of antidiuretic hormone and manifestations of hyponatremia [15, 60].
People with COVID-19, who are taking drugs that inhibit the renin-angiotensin-aldosterone (RAS), reduce the production of aldosterone, and this can cause fluid and electrolytes imbalances in the patient. Mineralocorticoid receptor (MR), which has different types, is expressed in various tissues, including the kidneys, GI tract, central nervous system (CNS), and heart, and is known as the aldosterone receptor. Activation of MR leads to changes in the concentration of ions (such as sodium and potassium). These changes are necessary to maintain the balance of fluid and electrolytes in the body. Still, due to MR’s presence in the large intestine [3, 61-63], if the aldosterone pathway is disrupted, the absorption and secretion of ions in the colon are disrupted, and fluid and electrolyte imbalance occurs. Hypokalemia, a complication of COVID-19, can exacerbate acute respiratory distress syndrome (ARDS) and increase the risk of heart injuries in patients [3, 29]. The number of ions, including sodium and potassium, is a significant indicator in COVID-19 patients [3, 49]. In some people with SARS-CoV-2 infection, the syndrome of inappropriate antidiuretic hormone secretion (SIADH) has been reported [3, 5], leading to disturbances in fluid and electrolytes [3].
Hypokalaemia exacerbates acute respiratory distress syndrome and acute cardiac injury, which are common complications in COVID-19, especially in patients with underlying lung or heart disease. Hypokalaemia also provides a pathophysiologic clue; SARS-CoV-2 binds to its host receptor, ACE2 and likely reduces ACE2 expression, leading to increased angiotensin II, which can cause increased potassium excretion by the kidneys, ultimately leading to hypokalaemia (29, 55, 64]. Increased plasma angiotensin II concentration has been described in patients with COVID-19, possibly acting as a mediator of acute lung injury, as earlier confirmed in SARS-CoV animal models [29, 64, 65]. A second potential contributor to hypokalaemia and other electrolyte imbalance in some COVID-19 patients may be gastrointestinal losses, with diarrhea and nausea present in as many as 34.0% and 3.9% of cases, respectively [29, 66].
It can be concluded that coronavirus infections induced increases in fasting blood glucose, serum urea, and creatinine, and a decrease in Na+ concentrations. There was a significant association between different parameters. These biochemical changes may help the clinicians to understand COVID-19 better and provide more clinical treatment options and prevent the serious complications of the disease. So, clinicians should pay special attention to FASTING BLOOD GLUCOSE, kidney function and electrolyte status of COVID-19 patients. Changes in FASTING BLOOD GLUCOSE, kidney function, and electrolyte levels can be a good indicator of disease progression.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
