
Research Article | DOI: https://doi.org/10.31579/2641-0419/246
1 Cardiology NHI, Egypt
2 Cardiology Menofia University
3 Cardiology, Alazhar university
*Corresponding Author: Abd Rabou Hamed, Cardiology NHI, Egypt.
Citation: Abd Rabou Hamed, Ahmed Elkersh, Ahmed Hegab, Abdulaziz Aboshahba . (2022). Effect of Coronary Arterial Dominance Post Primary Percutaneous Coronary Artery Intervention (PCI) during Hospital Stay and at 3-Month Follow-up. J. Clinical Cardiology and Cardiovascular Interventions, 5(4); Doi:10.31579/2641-0419/246
Copyright: © 2022 Abd Rabou Hamed, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 January 2022 | Accepted: 18 March 2022 | Published: 28 March 2022
Keywords: coronary arterial dominance; percutaneous coronary artery intervention; hospital stay; follow up
Background: Coronary vessel dominance, defined by the coronary artery that supplies the posterior descending artery (PDA) and posterolateral branches, influences the relative contribution of the different coronary arteries to the total left ventricular blood flow. This work aimed to evaluate the prognostic value of coronary arterial dominance post primary PCI, during hospital stay and at 3-month follow-up, which include; cardiac mortality, heart failure, non-fatal myocardial infarction, re-vascularization, stroke/TIA and re-admission for ACS.
Methods: This prospective observational study included 100 patients a with STEMI who underwent successful primary percutaneous coronary intervention with TIMI III flow and without procedural complications. Patients were divided into 3 groups according to coronary dominance: Right coronary dominant group (RCD), left coronary dominant group (LCD) and balanced coronary dominant group (BCD). All patients were subjected to transthoracic echocardiogram and coronary angiography and Primary percutaneous coronary intervention.
Results: Ticagrelor and clopidogrel during hospital stay and on hospital discharge were significantly used more with RCA group than LCX group and LCX & RCA group (P=0.021, 0.012), (P=0.018, 0.014), respectively. GPIIB/IIIA was significantly more used during hospital stay with RCA group than LCX group and LCX & RCA group(P=0.014). Nitrates was significantly used more on hospital discharge with RCA group than LCX group and LCX & RCA group (P<0.001).
Conclusions: Coronary arterial domi¬nance showed significant prognostic value in cases of myocardial Infarction after PCI, heart failure in LCX cases and in revascularization, heart failure, and stroke/TIA cases in RCA. Further, readmission for ACS was the most common outcome in all groups after 3-months follow-up.
Coronary vessel dominance, defined by the coronary artery that supplies the posterior descending artery (PDA) and posterolateral branches, influences the relative contribution of the different coronary arteries to the total left ventricular blood flow [1].
In a right-dominant circulation, the right coronary artery (RCA) supplies the posterior portion of the inter-ventricular septum and gives off the posterior descending artery. This contrasts with a left-dominant circulation, in which the left circumflex (LCX) artery supplies this territory. In a co-dominant circulation, supply of the posterior inter-ventricular septum is shared by the RCA and LCX. The prevalence of left dominance is 8%, whereas co-dominance has 7% population prevalence, [1] and right dominant system has a reported prevalence of 82–89% [2, 3]. In patients with a left dominant system, 60% of the left ventricular myocardium is supplied by the posterolateral branches and PDA originating from the LCx [4]. This less well-balanced coronary circulation might have a negative influence on prognosis of patients with coronary artery disease (CAD). Currently, the prognostic importance of coronary vessel dominance in patients presenting with first ST-segment elevation myocardial infarction (STEMI) remains uncertain [4].
Variations in coronary circulation are common, particularly with regard to the supply of the posterior wall of the left ventricle. While a right dominant coronary artery is most commonly observed, a left dominant system is considered to be a normal variant of the coronary anatomy [2, 3]. At present, little is known about the clinical relevance of this anatomical variation. A study screening 1620 post-mortem angiograms showed that the prevalence of a left dominant system decreased with age, [3] suggesting a higher death rate among patients with a left dominant coronary artery system. An explanation could be that a larger amount of myocardium is at risk in these patients, resulting in more extensive myocardial infarction in case of a left coronary artery occlusion.
However, there is limited knowledge about the relation between coronary dominance patterns and the risk of various adverse clinical events that can occur following percutaneous coronary interventions (PCI). Previously, Goldberg et al. [5] showed that the presence of a left dominant system was associated with an increased mortality in patients presenting with acute coronary syndrome (ACS). Accordingly, a more recent registry (the Cath PCI registry) observed higher in-hospital mortality after PCI in patients with a left dominant system [1].
Left ventricular (LV) systolic dysfunction and remodeling have been strongly associated with short- and long-term outcomes of patients with STEMI undergoing primary percutaneous coronary intervention (PCI) [6]. Independent correlates of LV systolic dysfunction and remodelling after STEMI include infarct size, heart rate, and severity of coronary artery disease [7-9]. LV dysfunction affected by coronary arterial dominance, as Yip et al. [10] showed that a left dominant system was independently predictive of failed reperfusion in patients with LCx artery infarction. The effect of coronary arterial dominance on LV dysfunction and remodelling at follow-up is unclear [5].
The aim of this work was to evaluate the prognostic value of coronary arterial dominance post primary PCI, during hospital stay and at 3-month follow-up, which include; cardiac mortality, heart failure, non-fatal myocardial infarction, re-vascularization, stroke/TIA and re-admission for ACS.
Patients and Methods
This prospective observational study included 100 patients a with STEMI who underwent successful primary percutaneous coronary intervention with TIMI III flow and without procedural complications. Exclusion criteria: Prior coronary artery bypass graft to assess the effect of specific culprit vessel site without confounding by by-pass grafts, previous PCI, usuccessful PCI, cardiogenic shock, STEMI with mechanical complication, left main disease >50%, previous myocardial infarction, valvular heart disease, atrial dysrhythmias, end stage renal failure and abnormal liver function. Patients were divided into 3 groups according to coronary dominance: Right coronary dominant group, (RCD), left coronary dominant group, (LCD) and balanced coronary dominant group, (BCD).
Transthoracic echocardiogram
2-dimensional echocardiography was performed within 48 hours of admission and at 3-month follow-up. Routine Images were obtained at rest. M-mode, 2-dimensional, and Doppler images acquired. Systolic LV function was assessed. LV ejection fraction (LVEF) was calculated (226). Subsequently, the LV was divided into 16 segments to calculate the wall motion score index (WMSI). Every segment was individually assessed and scored based on its motion and systolic thickening as the following: Normokinesis or hyperkinesis =1, Hypokinesis =2, Akinesis =3, Dyskinesis =4 and Aneurysm = 5. WMSI was calculated as the sum of the segment scores divided by the number of segments visualized (226). WMSI classified as the following: 1 is norma1, 1-1.49 is mild impairment, 1.5-1.99 is moderate impairment and ≥ 2 is severe impairment.
Coronary angiography and Primary percutaneous coronary intervention
The images of the coronary angiography and PCI were obtained according to standardized angiographic projections [11]. During the analysis coronary vessel dominance, the culprit vessel and culprit lesion and severity of CAD were recorded. The extent of CAD was expressed as the presence of one-, two- or three-vessel disease (stenosis causing ≥ 70 % luminal narrowing). Complete revascularization were defined as treating all present significant coronary artery stenosis (≥ 70 % luminal narrowing) during primary PCI or during secondary revascularization before discharge. Angiographic success of PCI was defined as TIMI III flow with residual stenosis below 0%.
Angiographic assessment of Coronary arterial dominance [12]
Coronary arterial dominance was defined according to the following definition: Right coronary dominant if the PDA and at least one posterolateral branches originating from the right coronary artery (RCA). Left coronary dominant if the PDA and the posterolateral branches originating from the LCx. Balanced coronary dominant if the PDA originating from the RCA in combination with posterolateral branches originating from the LCx artery [12].
The Brain Natriuretic Peptide
Test used: We used Alere Triage® BNP Test is a rapid, point of care fluorescence immunoassay designed to be used with the Alere Triage® Meters for the quantitative measurement of B-type natriuretic peptide (BNP) in EDTA anticoagulated whole blood or plasma specimens. The test procedure involves the addition of several drops of an EDTA
Statistical Analysis
All variables were expressed as mean ± standard deviation. The Chi-square test was used to analyse categorical variables. Student's t test and analysis of variance were used for continuous variables. Univariate and multivariate analyses were performed to identify independent predictors of no-premature atherosclerosis. Statistical analysis were made using SPSS 19.0. A P value <0>
All patient’s characteristics, ECG STEMI were insignificantly different among the studied groups. There was insignificant difference in approach of catheterization (femoral or radial) between the three groups. [Error! Not a valid bookmark self-reference.]
Table 1: Patient’s characteristics, ECG STEMI and approach to catheterization among three groups
| LCX (n = 29) | RCA (n = 70) | LCX & RCA (n = 11) | P value | ||
Age (years) | Mean ± SD | 54.45 ± 10.54 | 54.70 ± 9.71 | 61.36 ± 7.68 | 0.099 | |
Range | 37 - 76 | 28 - 75 | 47 - 73 | |||
Gender | Male | 22 (75.86%) | 58 (82.86%) | 9 (81.82%) | 0.720 | |
Female | 7 (24.14%) | 12 (17.14%) | 2 (18.18%) | |||
Hypertension | 23 (79.31%) | 56 (80.00%) | 8 (72.73%) | 0.859 | ||
DM | 16 (55.17%) | 47 (67.14%) | 7 (63.64%) | 0.530 | ||
Smoker | 11 (37.93%) | 36 (51.43%) | 7 (63.64%) | 0.282 | ||
ECG STEMI | ||||||
Inferior | 22 (75.86%) | 52 (74.29%) | 8 (72.73%) | 0.976 | ||
Posterior | 9 (31.03%) | 16 (22.86%) | 2 (18.18%) | 0.604 | ||
| Approach to catheterization | ||||||
Femoral | 24 (82.76%) | 64 (91.43%) | 9 (81.82%) | 0.376 | ||
Radial | 5 (17.24%) | 6 (8.57%) | 2 (18.18%) | 0.376 | ||
LCX: Left Circumflex coronary artery, RCA: Right coronary artery, DM: Diabetes mellites
There is insignificant difference in CKMB, serum creatinine andtype of stent and wire (soft and DES) and its diameter, length, and number of stents used among the three groups [Error! Reference source not found.]
Table 2: CKMB, Serum creatine, troponin T and Type of stent and wire used in PCI among three groups
| LCX (n = 29) | RCA (n = 70) | BCD (n = 11) | P value | ||
CKMB |
Mean ± SD |
78.17 ± 17.01 |
82.39 ± 13.03 |
89.64 ± 11.29 |
0.070 | |
Range | 110 - 80 | 120 - 85 | 105 - 90 | |||
Serum Creatine |
Mean ± SD |
|
1.03 ± 0.16 |
1.13 ± 0.20 |
0.204 | |
Range | 0.8 - 1.3 | 0.7 - 1.3 | 0.8 - 1.4 | |||
Positive serum troponin T | 29 (100%) | 70 (100%) | 11 (100%) | --- | ||
Type of stent and wire used in PCI | ||||||
Soft | 3 (10.34%) | 10 (14.29%) | 2 (18.18%) | 0.785 | ||
DES | 26 (89.66%) | 60 (85.71%) | 9 (81.82%) | 0.785 | ||
Diameter |
Mean ± SD |
3.18 ± 0.49 |
3.20 ± 0.41 |
3.27 ± 0.45 |
0.666 | |
Range |
2 - 4 |
2.25 - 4 |
2.5 - 4 | |||
Length |
Mean ± SD |
45.66 ± 24.36 |
38.41 ± 16.28 |
41.82 ± 18.57 |
0.223 | |
Range | 15 - 96 | 15 - 86 | 18 - 78 | |||
Number of Stents |
Mean ± SD |
1.45 ± 0.57 |
1.26 ± 0.44 |
1.45 ± 0.52 |
0.17 | |
Range | 1 - 3 | 1 - 2 | 1 - 2 | |||
LCX: Left Circumflex coronary artery, RCA: Right coronary artery, CKMB: Creatine kinase-MB
Low-density lipoprotein was significantly higher in LCX & RCA group than RCA group and LCX group and was significantly higher in RCA group than LCX group (p <0>
High-density lipoprotein was significantly lower in LCX group than RCA group (p =0.021), but there was insignificant difference between LCX group and LCX & RCA group, and between RCA group and LCX & RCA group. [Table 3
EF was significantly higher in RCA group than LCX group and LCX & RCA group, and was significantly higher in LCX & RCA group than LCX group.
EF after 3 months was significantly different among the three groups (P =0.007). It was significantly higher in RCA group than LCX group and LCX & RCA group, and was significantly higher in LCX group than LCX & RCA group. [Table 3
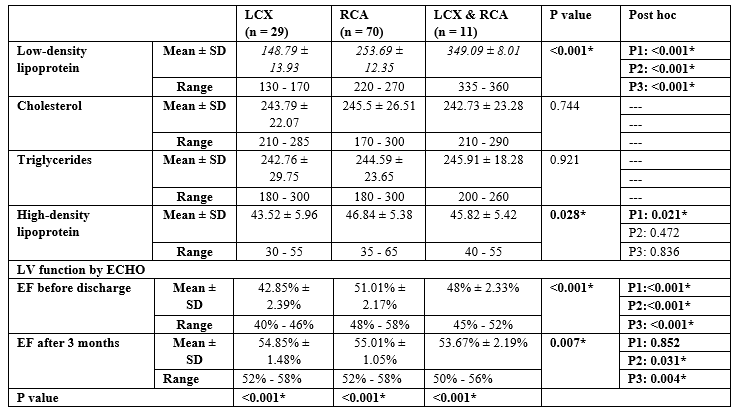
LCX: Left Circumflex coronary artery, RCA: Right coronary artery, P1: Significance between LCX and RCA, P2: Significance between LCX and LCX & RCA, P3: Significance between RCA and LCX & RCA
BNP before discharge was significantly different among the three groups (P <0>[Table 4
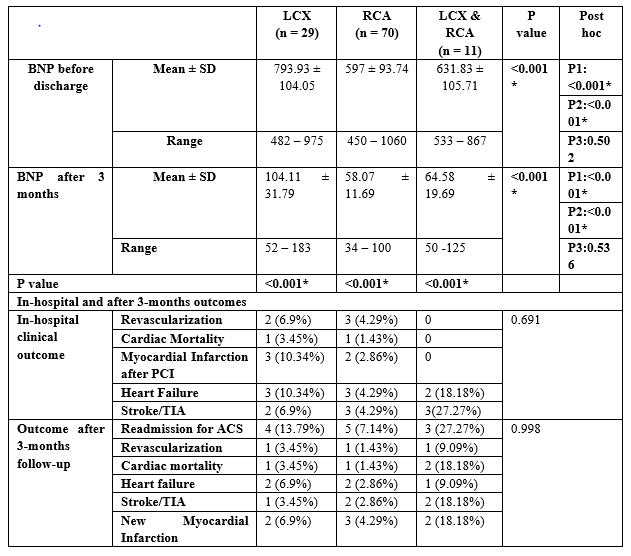
LCX: Left Circumflex coronary artery, RCA: Right coronary artery, BNP: B-type natriuretic peptide, *Significant as p value <0>P1: between LCX and RCA P2: between LCX and LCX and RCA P3: between RCA and LCX and RCA
Ticagrelor and clopidogrel during hospital stay and on hospital discharge were significantly more used with RCA group than LCX group and LCX & RCA group( (P=0.021, 0.012), (P=0.018, 0.014) respectively). GPIIB/IIIA was significantly more used during hospital stay with RCA group than LCX group and LCX & RCA group(P=0.014). Nitrates was significantly more used on hospital discharge with RCA group than LCX group and LCX & RCA group (P<0>].
Table 5: Drugs received during hospital stay and on hospital discharge among the three groups
| LCX (n = 29) | RCA (n = 70) | LCX & RCA (n = 11) | P value | |
Nitrates | 29 (100%) | 70 (100%) | 11 (100%) | --- | |
BB | 29 (100%) | 70 (100%) | 11 (100%) | --- | |
ACI | 29 (100%) | 70 (100%) | 11 (100%) | --- | |
Ticagrelor | 25 (86.21%) | 43 (61.43%) | 5 (45.45%) | 0.021* | |
STAIN | 29 (100%) | 70 (100%) | 11 (100%) | --- | |
GPIIB/IIIA | 8 (27.59%) | 16 (22.86%) | 7 (63.64%) | 0.014* | |
Clopidogrel | 3 (10.34%) | 27 (38.57%) | 6 (54.55%) | 0.018* | |
| LCX (n = 29) | RCA (n = 70) | LCX & RCA (n = 11) | P value | |
BB
| 29 (100%)
| 70 (100%)
| 11 (100%)
| --- | |
ACEI
| 29 (100%)
| 70 (100%)
| 11 (100%)
| --- | |
Aspirin
| 29 (100%)
| 70 (100%)
| 11 (100%)
| --- | |
Ticagrelor
| 25 (86.21%) | 43 (61.43%) | 5 (45.45%) | 0.012* | |
STATIN
| 29 (100%)
| 70 (100%)
| 11 (100%)
| --- | |
Diuretics
| 7 (24.14%) | 30 (42.86%) | 7 (63.64%) | --- | |
Nitrates | 6 (20.69%) | 43 (61.43%) | 11 (100.00%) | <0>
| |
Clopidogrel | 4 (13.79%) | 31 (44.29%) | 6 (54.55%) | 0.014* |
LCX: Left Circumflex coronary artery, RCA: Right coronary artery, BB: Beta-blocker, ACEI: Angiotensin converting enzyme inhibitor, *Significant as p value <0>
Coronary artery dominance is associated with the extent of CAD with incidence and all‑cause mortality of AMI but not with atherosclerotic involvement. Research has suggested difference in post‑PCI outcome and mortality of patients with acute coronary syndrome (ACS) undergoing PCI based on their coronary artery dominance. Coronary artery dominance is also associated with 30‑day mortality and early reinfarction after STEMI [13-15].
In our study, there was an insignificant difference CKMB between the three groups.
Our results were not in consistent with [16]. They observed that median CK‑MB were significantly different, and the highest values were observed in LD group (195.79 U/L, respectively). Larger included sample size and ethnic consideration can explain this contradiction. However, [17] found that the peak level of CK-MB was significantly higher in LCX group than in RCA group. This difference could be justified by the large recruited sample size and excluding patients with codominant LCX & RCA.
In our study, there was insignificant difference in approach of catheterization (femoral or radial) between the three groups. Our findings were in agreement with [18] who observed no significant difference in catheterization (femoral or radial artery) between the right- or co-dominant anatomy (RD group) and those with left dominant anatomy (LD group).
In our study, there is insignificant difference in type of stent and wire (soft and DES) and its diameter, length, and number of stents used among the three groups.
In consistent with our results, [19] assessed two-year follow-up data of 1,387 patients from the randomized TWENTE trial. Based on the origin of the posterior descending coronary artery, coronary circulation was categorised into left and non-left dominance (i.e., right and balanced). This was in line with [16] results; as no significant difference was detected in terms of stent type, size, and number among right, left and Co‑dominant groups.
Moreover, [20] reported no significant difference between all studied group in stent length, number and diameter.
In the present study, EF before discharge was significantly different among the three groups (P <0>
Comparable to our findings, [17] found that EF was higher in RCA group than LCX group.
In our results, EF after 3 months was significantly different among the three groups (P =0.007). It was significantly higher in RCA group than LCX group and LCX & RCA group and was significantly higher in LCX group than LCX & RCA group.
Similarly, [21] conducted a study to compare the outcome of patients with CX versus right coronary artery (RCA) related STEMI. A total of 1683 consecutive patients with STEMI were studied. Patients who lacked STEMI were also included if they had persistent chest pain with signs of ischaemia or regional wall motion abnormalities on echocardiography. Coronary angioplasty was performed according to standard procedures. After the intervention, all patients received aspirin and clopidogrel or ticlopidine. The results showed that LVEF was significantly higher in patients with RCA- related MI treated by primary percutaneous intervention (PCI) when compared to LCX- related MI. Further, [17] results demonstrated that the left ventricular ejection fraction was notably lower in LCX group than RCA group after 30-Day. This difference could be related to the variety in duration of follow up.
In contrast, [20] found no significant difference in lower left ventricular ejection fraction after 3 months by both 2D and 3D echocardiography in patients with left dominant, right coronary dominant, and balanced coronary dominant groups.
Our findings were in line with [22] study which included one hundred fifty consecutive patients with acute inferior wall STEMI. Patients were divided into two groups according to the infarct related artery (LCX vs. RCA). All patients underwent routine adjunctive angioplasty after TLT during the index hospitalization and clinical characteristics and outcomes were compared. There was lower left ventricular ejection fraction (LVEF) (p= 0.01) in patients with LCX occlusion compared with RCA.
In the present study, EF after 3 months was significantly higher than before discharge in the groups (p <0>, [20] found that after 3 months follow-up a significantly lower left ventricular ejection fraction at admission was observed by both 2D and 3D echocardiography in patients with a left dominant system.
In our study, regarding in-hospital clinical outcome, the most common outcomes in the LCX group were myocardial Infarction after PCI and heart failure each occurred in 3 (10.34%) patients, the most common outcomes in the RCA group were revascularization, heart failure, and stroke/TIA each occurred in 3 (4.29%) patients, the most common outcome in the LCX & RCA group was Stroke/TIA occurred in 3 (27%) patients.
In consistent with our results, [17] study results demonstrated that the frequency of advanced congestive heart failure was remarkably higher in group LCX than in RCA group (all P < 0>
Furthermore, [23] conducted a prospective, observational, nonrandomized study and enrolled 200 consecutive patients with inferior wall STEMI. All patients were treated with emergency percutaneous coronary intervention during hospitalization and clinical characteristics and outcomes were compared. Group 1 included 100 patients presented with acute inferior wall STEMI caused by RCA occlusion and Group 2 included 100 patients presented with acute inferior wall STEMI caused by LCX occlusion. Total primary outcome in their study was higher in LCX group (p=0.048) that may be related to heart failure, stroke and bleeding which were more than RCA group.
Limitations: The study population was of limited size and the number of sites included in our registry. We only included patients with acute STEMI who were treated with primary PCI, which may have influenced the prevalence of CD pattern. Our findings must be interpreted in the context of acute STEMI treated with primary PCI, and they do not necessarily apply to all patients with acute STEMI.
Coronary arterial dominance showed significant prognostic value in cases of myocardial Infarction after PCI, heart failure in LCX cases and in revascularization, heart failure, and stroke/TIA cases in RCA. Further, readmission for ACS was the most common outcome in all groups after 3-months follow-up.
Nil
Conflict of Interest: Nil
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
