
Review Article | DOI: https://doi.org/10.31579/2642-9756/195
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
2 Obstetrics Gynecological Nursing, Faculty of Nursing Benha University
*Corresponding Author: 1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt 2 Obstetrics Gynecological Nursing, Faculty of Nursing Benha University
Citation: Abdelazim Mohamed AS, Hassan Omran AA, Elham A. Ramadan, Hanan E. Hassan, (2024), Effect of Body Mass Index on Urinary Incontinence Among Menopausal Women, J. Women Health Care and Issues, 7(3); DOI:10.31579/2642-9756/195
Copyright: © 2024, Hanan Elzeblawy Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 January 2024 | Accepted: 15 March 2024 | Published: 25 March 2024
Keywords: body mass index; urinary incontinence
Background: World Health Organization (WHO) mentioned that around 200 million people worldwide experience urinary incontinence. Aim of the study: The study was conducted to assess level of obesity and its relation with urinary incontinence among elderly women. Design: A descriptive study design was utilized in this study. Sample: A purposive sample was selected and this study was performed on 100 Menopausal women diagnosed with stress urinary incontinence. Setting: gynecological and urological outpatient clinics Beni-Suef university hospital. Tools: Data was collected using a structure interviewing questionnaire schedule. Results: About two-thirds (72%) of the studied women were obese while one-quarter (24%) of them was overweight. Around one-third (32%) of the studied women began to suffer from stress urinary incontinence from 3-4 years. As well as, more than a half (52%) of them suffered from daily stress urinary incontinence. Conclusion: A statistical significant association between BMI and frequency of urinary incontinence among the studied sample was found. Recommendations: Application of an education program regarding healthful nutrition and optimal body weight to avoid urinary incontinence among elderly women
Urinary incontinence is a major global health problem. The prevalence of UI increases with age, though the prevalence rate in women between 15 and 64 is from 10% to 30% and only a quarter of all women with this problem seek help. It is estimated that 20% to 40% of the elder women present involuntary loss of urine [1-8]. Also, World Health Organization (WHO) mentioned that around 200 million people worldwide experience urinary incontinence [9].
Menopause is divided into three periods as premenopausal, perimenopausal, and post-menopausal. Premenopausal period: Covers the 2-6-year period before menopause. In this period ovaries gradually lose their power of function. The order of menstrual cycle is lost and the chance of fertility decreases. Irregular cycles can take a few months or a few years [10-17].
Perimenopausal period: Covers menopause and the first year after menopause. In this period, the decrease of estrogen results in cycle disorders, vasomotor changes and mental disorders. Postmenopausal period: Covers the period from menopause until old age, which is approximately 6-8 years after menopause. As a result of the decrease of ovarian hormones, old age-related organic diseases such as vaginal atrophy, osteoporosis, cardiovascular disorders and skin problems are seen. Vulva, vagina, urethra and bladder contain estrogen receptors [18-25].
The decrease of estrogen effects results in distinct dysfunctions in the urogenital system. After the menopause, the lower part of urethra contracts and loses its flexibility. In this period, urethral syndrome associated with findings of burning sensation during urination, difficulty in holding urine, interrupted urinating and nocturia is seen [26-30].
As a result of estrogen deficiency, vagina is unable to collect sufficient glycogen in the epithelium cells and the acid reaction of vagina regresses, which causes the development of an alkali environment in vagina. This condition forms a basis for infections. Cervix shrinks with the decrease of estrogen and mucus secretion reduces, which results in the increase of vaginal dryness. Majority of women in the postmenopausal period face vaginal dryness. They may also complain about dyspareunia because vagina loses its elasticity [31-34]. During the menopausal period, estrogen deficiency results in losing the tonus of pelvic floor. Weakness in pelvic floor increases the complaint of stress urinary incontinence (SUI). It is one of the most prevalent bladder control problems encountered during the menopausal period; however, it does not typically worsen due to menopause [35]. Also, during the menopausal period, bladder dysfunctions develop with increasing age, which results in the decrease of bladder capacity and urinating speed and the increase of urinating time. Depending on the decrease in estrogen level; the decrease of the tonus of sphincters, impairment of the closing capacity of urethral lumen, decrease of urethra length and hypermobility in case of stress are seen [26].
Urodynamic changes associated with age include smaller voided volume, increased residual volume, smaller bladder capacity, and increased involuntary detrusor contractions. Among older women, large cystoceles may also contribute to elevated post- void residual urine. Incomplete bladder emptying from all causes can reduce functional bladder capacity, and thereby contribute to the urinary frequency and nocturia common in older people [36]. Elder people may have a combination of detrusor over activity on filling and poor contractility during voiding, a condition termed detrusor hyperactivity with impaired contractility (DHIC). In such cases, the bladder contraction does not empty. The bladder fully, leaving a large post-void residual (which otherwise is not explained by bladder outlet obstruction). Symptoms include leakage with urgency, leakage with increases in abdominal pressure, dribbling, frequency, and nocturnal similar to other LUT conditions such as stress UI and obstruction, for which DHIC easily can be mistaken people [36-38].
To assess level of obesity and its relation with urinary incontinence among elderly women through:
Research questions
Subject and methods
Study Setting and Sampling:
A Purposive sample was used from the above mentioned setting. Total sample was 100 women.
Tool of data collection:
A structured interviewing questionnaire sheet was developed by the researcher in the Arabic language based on a review of recent literatures, under guidance of supervisors. It was consist of two parts:
The first part: included personal characteristics data of the study women such as (age, height, weight, body mass index "BMI" education level, occupation, residence, marital status).
Second part: urinary incontinence history included duration of illness, frequency, amount of leakage of urine, timing (day and night), and predisposing factors as coughing, sneezing, laughing, using sanitary towels for urine leakage, frequency of change the towels.
Administrative Design:
An official written approval letter for data collection to conduct this study clarifying the purpose of the study was obtained from dean of faculty of nursing, Benha University to the director of Beni-Suef university hospital.
Statistical Design:
The collected data was revised, coded, tabulated and introduced to a computer using statistical package for social sciences (IBM SPSS .25.0). Data was presented and suitable analysis was done according to the type of data obtained for each parameter.
Table (1): Illustrates the mean and standard deviation of studied sample according to their age, weight, height and Body Mass Index. It reveals that the minimum age of the studied women was 50 years old and the maximum age was 66 years old. Moreover, the minimum weight of the studied women was 55 kg and the maximum one was 120 kg. However, the minimum height of the studied women was 150 cm and the maximum one was 167 cm. In addition, the minimum body mass index of the studied women was 21.76 and the maximum one was 45.17.
Figure (1): Portrays the distribution of studied sample according to their obesity level; It revealed that about two-thirds (72%) of the studied women were obese while one-quarter (24%) of them was overweight.
Figure (2): Indicates that around one-third (32%) of the studied women began to suffer from stress urinary incontinence from 3-4 years. As well as, more than a half (52%) of them suffered from daily stress urinary incontinence. In addition, the majority (97%) of them did not lose urine during sleep. Regarding the amount of urine leakage per once, the same figure illustrates that 38% lost splashes amount of urine, while 27% lost large amount of urine per once.
Figure (3): Demonstrated the distribution of studied sample according to the severity of urinary incontinence. It reveals that 75% among the studied women has severe urinary incontinence, 13% of them have mild level, and 12% of them have moderate level.
Table (2): Demonstrates the relationship between body mass index and frequency of urinary incontinence. It reveals that there was statistical significant association between BMI and frequency of urinary incontinence among the studied sample (p<0> Minimum Maximum Mean Std. Deviation Age (in years) 50 66 54.23 2.87 Weight 55.0 120.0 82.680 11.8815 Height 150.0 167.0 160.420 2.8610 BMI 21.76 45.17 32.1224 4.47973
Table 1: Mean and standard deviation of studied sample according to age, weight, height and Body Mass Index
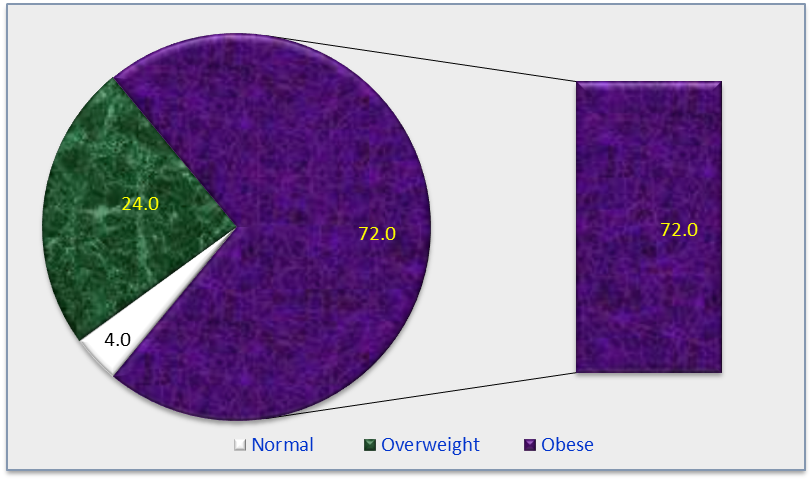
Figure 1: Distribution of studied sample according to their obesity level (n=100)
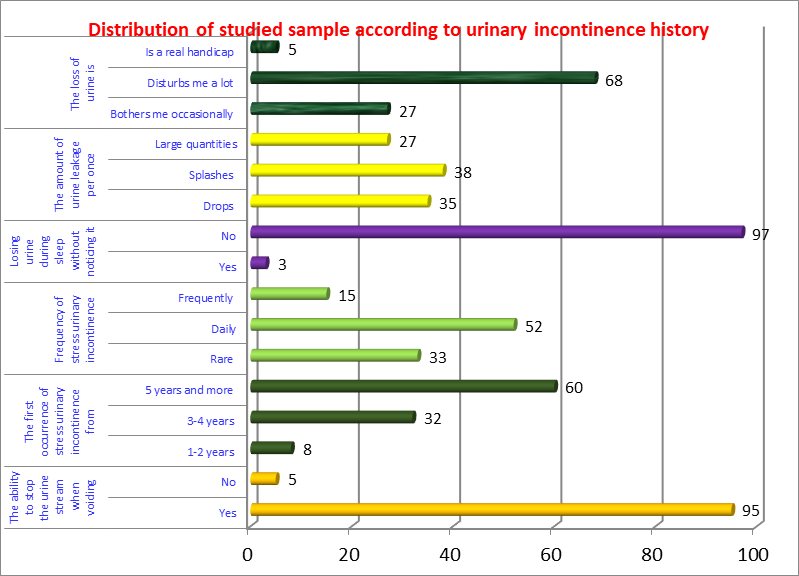
Figure 2: Distribution of studied sample according to urinary incontinence history (n=100)
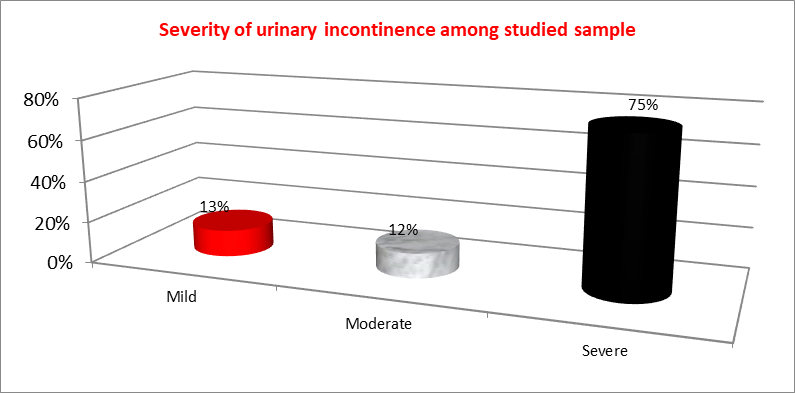
Figure 3: Distribution of studied sample according to the severity of urinary incontinence (n=100)
| Frequency of urinary incontinence | Body mass index | |||||||
| Normal | Overweight | Obese | X2 | p-value | ||||
| No | % | No | % | No | % | |||
| About once a week or less often | 4 | 100.0 | 6 | 25.0 | 10 | 13.8 | 19.75 | 0.003* |
| Two or three times a week | 0 | 0.0 | 8 | 33.3 | 22 | 30.6 | ||
| About once a day | 0 | 0.0 | 2 | 8.4 | 3 | 4.2 | ||
| Several times a day | 0 | 0.0 | 8 | 33.3 | 37 | 51.4 | ||
*significant at p≤ 0.05 **highly significant at p≤0.01
Table 2: Relationship between body mass index and frequency of urinary incontinence (n=100)
Elder women refer to women age 50 and older. Ageing women refers to the same chronological group but emphasizes that ageing is a process that occurs at very different rates among various individuals and groups. Privileged women may remain free of the health concerns that often accompany ageing until well into their 70s and 80s. Others who endure a lifetime of poverty, malnutrition and heavy labour may be chronologically young but functionally “old” at age 40 (WHO, 2007). The more traditional Africans definitions of an elderly person correlate with chronological age of 50 to 65 years, depending on the setting, the region and the country [39].
Regarding correlation between Body Mass Index and the frequency of urinary incontinence, the current study demonstrated that there was statistical difference in the frequency of urinary incontinence in relation to Body Mass Index among the studied women after practicing deep breathing and kegel exercises. This was agreed with Jayachandran(2019) who assessed the Prevalence of Stress, Urge, and Mixed Urinary Incontinence in Women and mentioned that body mass index has been associated with urinary incontinence as the greatest number of women in the overweight and obese categories had stress urinary incontinence [40]. This result disagreed with Nygaard C et al (2019) who assessed the Impact of menopausal status on the outcome of pelvic floor physiotherapy in women with urinary incontinence and found no statistically significant association between BMI and frequency of urinary incontinence [41]. From the researcher point of view, higher Body Mass Index causes increased pressure on the abdomen with strenuous activity, accounting for increased occurrence of Stress Urinary Incontinence in obese women. The excess weight weakens the pelvic floor muscles that support the bladder and urethra, causing urine to leak. Women with higher Body Mass Indices tend to have a higher incidence of comorbidities such as diabetes and high blood pressure, which might also play a contributing role in prevalence of urinary incontinence.
A statistical significant association between BMI and frequency of urinary incontinence among the studied sample was found.
Application of an education program regarding healthful nutrition and optimal body weight to avoid urinary incontinence among elderly women
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
