
Research Article | DOI: https://doi.org/10.31579/2578-8868/373
1Assistant Professor, Neuroanesthesia, Indira Gandhi Medical College, Shimla, India.
2Associate Professor, Pediatric Surgery, Indira Gandhi Medical College, Shimla, India.
3Associate Professor, Anaesthesiology & Critical care, Indira Gandhi Medical College, Shimla, India.
4Assistant Professor, Pediatric Surgery, Indira Gandhi Medical College, Shimla, India.
5Resident, Anaesthesiology & Critical care, Indira Gandhi Medical College, Shimla, India.
*Corresponding Author: Kunal Kumar Sharma, Assistant Professor, Neuroanesthesia, Indira Gandhi Medical College, Shimla, India
Citation: Kunal K. Sharma, Raj Kumar, Rajesh K. Verma, Kamalkant Khidtta and Parveen Kumar (2025), Effect of Anesthesia on Intracranial third Ventricular Diameter in Infants and Toddlers- A Case Series, J. Neuroscience and Neurological Surgery, 17(5); DOI:10.31579/2578-8868/373
Copyright: © 2025, Kunal Kumar Sharma. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 18 April 2025 | Accepted: 02 May 2025 | Published: 19 May 2025
Keywords: infants; third ventricular diameter; nitrous oxide; intracranial pressure; anesthesia
Background and Objective: This case series investigates the effect of anesthetic technique—specifically nitrous oxide use—on the third ventricular diameter (TVD) in infants and toddlers undergoing pediatric surgical procedures under general anesthesia. Methods: Transcranial sonography was used to assess TVD at multiple intraoperative time points in a cohort of pediatric patients. Comparative analysis was conducted between patients receiving O₂:N₂O and O₂:Air anesthetic mixtures alongwith sevoflurane and caudal / epidural analgesia. Results: The study cohort of 15 patients was analyzed. A statistically significant change in TVD was observed across time points, particularly between post-skin incision and skin closure. The O₂:Air group demonstrated greater ventricular dilation compared to the O₂:N₂O group. Eleven patients received caudal block, whereas one patient received epidural catheter insertion for perioperative analgesia.Conclusion: Nitrous oxide usage in 50:50 ratio with oxygen and sevoflurane exerts minimal effect on intraoperative third ventricular dilation. However, confounding factors such as caudal / epidural analgesia efficacy warrant further investigation in form of randomized trials to generate level 1 evidence in this regard.
The third ventricle can be visualized using transcranial ultrasound through the trans-temporal bone window—a method primarily described for assessing brain structures and ventricles in patients with hydrocephalus,[1,2] psychiatric disorders3 and neurodegenerative pathologies.[4-6]
In pediatric populations, particularly infants and toddlers, the temporal bone is generally more penetrable, making ultrasound-based measurement of the third ventricle a promising, non-invasive, and radiation-free method for assessing the ventricular system in children with hydrocephalus. However, anesthetic agents such as nitrous oxide (N2O) —commonly used for maintenance during pediatric surgery—can influence craniometrics by altering cerebral blood flow and, subsequently, intracranial pressure.
N2O is a colorless, non-inflammable gas used as a carrier gas for sevoflurane. It has a minimum alveolar concentration of 105% and a blood/gas partition coefficient of 0.46. It acts by partial blockade of acetylcholine, gamma-aminobutyric acid, N-methyl-d-aspartate and histamine receptors. It also partially potentiates GABA and glycine receptors. Because of its poor blood solubility, alveolar and brain concentrations are achieved very rapidly. When administered with sevoflurane it causes increase in cerebral blood flow, however this effect gets decreased when administered with propofol. Increase in intracranial pressure and impairment of cerebral autoregulation have been reported with its use.[7]
Although there is a renaissance in recent studies that are exploring the impact of anesthetic induction on cerebral oxygenation,8 electroencephalography trends[9] and cerebral blood flow.[10] There still remains a gap in published literature regarding effect of N2O on infants and toddlers. Therefore we decided to investigate this potential confounding factor, by conducting an observational study on a cohort of children of this age group. They underwent complex pediatric surgical procedures under general anesthesia. Therefore we assessed the impact of anesthetic maintenance with nitrous oxide on the third ventricle diameter assessed sonographically using the phased array probe of Sonosite TM machine (Figure 1)

This case series adheres to the EQUATOR network guidelines. As the observational analysis was being done on the existing anesthetic practice of the institute, the ethical clearance was not required. After valid informed consent from the parent of the child, the patient was brought into the operation theatre after premedication.
Anesthetic induction was done as per conventional protocol of balanced anesthesia technique. The muscle relaxant used to facilitate jaw relaxation was recorded in the excel chart. Endotracheal tube was inserted as per the age appropriate formula. Cuffed endotracheal tubes were inserted as per the size predicted by Motoyama formula, whereas the uncuffed endotracheal tubes were inserted as per the size predicted by Cole's formula.
Although the ETT was inserted as per the formula for depth of the tube i.e. (age in years / 2) + 12 cm, we mandatorily auscultated bilateral air entry after insertion of the ETT. The first assessment of third ventricular diameter (TVD) was done at this time using phased array transducer of Sonosite TM machine. Thereafter the child was placed in lateral position for caudal block or epidural catheter insertion as per the requirement cited by the pediatric surgeon (Figure 2). After this procedure, the child was placed in the operative position and TVD was assessed at skin incision, skin closure and prior to extubation.

Figure 2: Child positioned for caudal block in lateral position after endotracheal intubation
The demographic analysis of 13 male and 2 females children revealed an age {mean + standard deviation} of 24.7 + 12.8 months; inter-quartile range (IQR) of 12.5 - 36 months. Uncuffed Oral Endotracheal Tube (UCETT) was used in 7 children, while rest of them were intubated with Cuffed Oral Endotracheal Tube (COETT) (Figure 3).
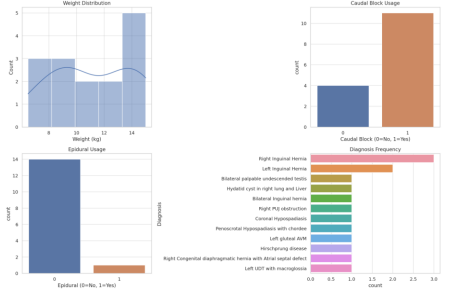
Figure 3: The trend of demographic data
Third ventricle diameter trend across the four intraoperative time points of measurement, depicted a trend toward increase in the TVD after intubation (D1) till skin closure (D3). The largest mean TVD was seen at the skin closure (D3), this suggested transient dilation of the third ventricle during surgery. By the time of extubation (D4), TVD stabilized or decreased slightly but often did not return completely to the initial values observed soon after intubation (D1) (Figure 4).

Figure 4: Boxplot illustrating the trend of third ventricular diameter across the observed time points
Non-parametric test for repeated measures (Friedman test) revealed a statistically significant difference in third ventricle diameters across the four intraoperative time points, (p-value= 0.0062). Post-Hoc pair-wise comparisons using the Wilcoxon Signed-Rank Test showed a statistically significant change in the third ventricle diameter over the course of surgery i.e. between skin incision (D2) and skin closure (D3) (p < 0>
| Comparison of TVD between observed time points | p-value | Interpretation |
| D1 vs D2 | 1.000 | Not significant |
| D1 vs D3 | 0.382 | Not significant |
| D1 vs D4 | 0.723 | Not significant |
| D2 vs D3 | 0.004 | Significant |
| D2 vs D4 | 0.108 | Not significant |
| D3 vs D4 | 1.000 | Not significant |
Table 1: Comparison of TVD between the observed time points using Wilcoxon Signed-Rank Test
Analysis between patients who received O2:N2O and O2: Air: was done by using the numerical encoding of 0 for O₂: N₂O group and 1 for O₂: Air group. The O₂: N₂O group exhibited a increase in diameter till the culmination of anesthesia protocol (D1 to D4). However, the overall trend appeared to be more stable in comparison to the O₂: Air group. This group showed a steeper rise, between the time points from D1 to D3, and thereafter it exhibited a modest decrease in TVD at the time of culmination of anesthesia, just prior to extubation (D4) (Figure 5). Interestingly the O₂: Air: group demonstrated greater fluctuation in ventricular size, with a notably larger increase at the time of skin closure (D3).
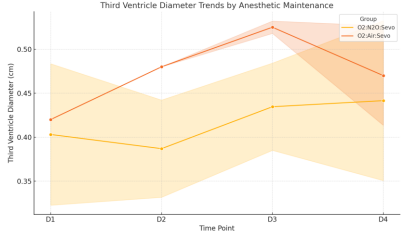
Figure 5: Comparison of third ventricular diameter between the O2:N2O group and O2:Air group
The comparison between the observed time points of TVD assessment was done using Mann-Whitney U test. It revealed significant differences at D2 (post skin incision) and D3 (skin closure). At these time points, the O₂: Air group had significantly larger third ventricle diameters compared to the O₂: N₂O group. There was no significant differences at baseline (D1) or pre-extubation (D4). (Table 2)
| Observed time point for TVD assessment | U statistic | p-value | Interpretation |
| D1 | 9.0 | 0.55 | Not significant |
| D2 | 0.0 | 0.033 | significant |
| D3 | 0.0 | 0.033 | significant |
| D4 | 12.0 | 0.93 | Not significant |
Table 2: Comparison of observed time points for TVD assessment using Mann-Whitney U test
Mechanical ventilation and ETT positioning can directly influence intracranial pressure. While formulas such as Motoyama’s and Cole’s provide population-based ETT size estimation, optimal depth of insertion of endotracheal tube is required for avoiding mainstem bronchus intubation. That is why we inserted the ETT as per the PALS estimation formula for this purpose {[Age (in years) / 2] + 12}
Nevertheless, there are other formulas also but their performance is variable for each individual patient, because age-based or height-based formulas are based on population statistics and the current patient may be outside the mean of that population.12 Internal diameter estimation of ETT can be done by simply following the equation: 3 x ID of ETT. However, it can only be used for ETT 3.0 or greater, and it has ~ 59
As per the data obtained from this study cohort, the usage of nitrous oxide in 50-50 % with oxygen does not result in increase in ICP in comparison to using oxygen Air mixture in same ratio. However, adequately powered level 1 evidence is mandated for further research in this regard.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
