
Research Article | DOI: https://doi.org/10.31579/2578-8965/180
1 DNP, APRN, GNP-C, Associate Senior Faculty Benjamín León - Miami-Dade College, School of Nursing, Miami, Florida, United States.
2 Psychologist, Specialist in Organizational Communication, Master in Research Methods in Education from the University of La Rioja, Spain. PhD in Educational Sciences. Research professor at the American University Corporation, Barranquilla, Colombia.
3 Professor and researcher of the Educational and Social Synapsis Group and the Psychology Program, Faculty of Human and Social Sciences, Simón Bolívar University of Barranquilla, Colombia. Associate Researcher of Minciencias.
4 Environmental Engineer, Specialist in pedagogy and teaching. Magister in watershed management, Secondary education teacher, Ministry of Education of Colombia.
5 Professor and researcher of the Universidad Estatal a Distancia, San José, Costa Rica.
*Corresponding Author: Sara Concepción Maury-Mena, Psychologist, Specialist in Organizational Communication, Master in Research Methods in Education from the University of La Rioja, Spain. PhD in Educational Sciences. Research professor at the American University Corporation,
Citation: Antolín Maury, Maury-Mena SC, Marín-Escobar JC, Marín-Benítez AC, Olman S. Ureña (2023), Educational Intervention on Dm2in a Miami-Dade Homeless Population, J. Obstetrics Gynecology and Reproductive Sciences, 7(6) DOI:10.31579/2578-8965/180
Copyright: © 2023, Sara Concepción Maury-Mena. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 July 2023 | Accepted: 30 July 2023 | Published: 10 August 2023
Keywords: self-control; self-care; type 2 diabetes; educational intervention; food insecurity; correlational study
Objective: Homeless people have significantly more health needs and higher rates of morbidity and mortality, as well as more hospitalizations and / or rehospitalizations than the general population, caused by factors such as extreme poverty, poor access to medical care and the challenges in adherence to medications, for which the present study set out to apply an educational intervention on type 2 diabetes, aimed at homeless people living in a shelter, in order to improve self-control and self-care techniques of this chronic disease.
Materials and methods: The educational intervention was conducted in a Miami Dade homeless shelter with 250 participants and consisted of three diabetes self-management and self-care sessions and a list of community resources in the preferred language of the community. person (English or Spanish). The evaluations included a survey before and after the intervention and a pre- and post-evaluation using the Diabetes Knowledge questionnaire (DKQ-24).
Results: Demographic data: 88% male and 12% female, 40% Hispanic, 36% African American, 26% Caucasian, 64% English and 36% Spanish language. There was a significant difference in the measurement before and after two months of the educational intervention (p less than 0.001).
Conclusions: Educational intervention to improve the quality of life, self-control, and self-care of homeless patients with type 2 diabetes had a positive effect and these results may provide the basis for future interventions that help health professionals to identify needs and address them through context-specific educational interventions. Approval n. IRB 17-OR-372-ME of the Institutional Review Board (IRB).
Diabetes is a serious health problem that affects 9.3% of the general population in the United States. In Miami Dade the 8.9% of homeless adults live with diabetes (Miami Dade County, 2016). Among the adult homeless population in the United States ranges from 2% and 18%2, so uncontrolled
diabetes can have a significant effect on morbidity and mortality in this population.
According to a Miami-Dade County press release (Bernstein, 2015), the total number of homeless people was 4,235. Therefore, concern for the health of the homeless population is a matter of local and national importance, especially those that suffer from chronic diseases such as type 2 diabetes.
On the other hand, homelessness is a health problem that homeless people have higher morbidity rates and mortality, as well as more hospitalizations than the population and suffer from unmet health care needs (To, Brothers & Zoost, 2016).
According to Bernstein, et al. (2015), the prevalence of certain chronic conditions such as diabetes and high blood pressure among the homeless population is similar to that of the population general, however, by not complying with a balanced diet and when presenting inadequate adherence to medications, lack of access to medical care, as well as insecurity of get daily food, become problems that exacerbate the complications of chronic diseases among this population.
In O'Toole's studio (2017) about insecurity to get the daily diet, it was found that 19.8% of people had diabetes or prediabetes, and 43.5% reported having symptoms of hypoglycemia when they ran out of food.
As indicated by Rojas-Guyler et al. (2014) for the homeless population It is a priority to find where to take refuge and what to eat before take care of your health, even if it is a chronic illness with serious consequences such as diabetes. The above is accentuated if consider the lack of knowledge and education about the diabetes and the need to improve self-management skills and self-care of this condition in this population (Appek, Giger & Davighizar, 2005).
Wood et al. [7] also indicated that limited transportation and low income contributes to the challenges related to self-management and self-care of diabetes. About this, Abubakari et al. (2015) and Rodríguez-Burelo et al. (2019), indicate that disparities in self-management of diabetes and uncontrolled diabetes can be link with the perceptions of the disease and the beliefs of self-efficacy of this population.
As Bernstein et al. (2015), homeless people have significantly more health needs and contribute to rates of morbidity and premature mortality, which also have an impact on state-funded health agencies,
emergencies of primary care networks, providers of health care, homeless service programs and health care facilities.
Likewise, in the study to determine the prevalence of diabetes among homeless veterans (Iheanacho & Rosenheck, 2016), they were found to have an increased risk of several chronic diseases and that there were 8% higher risk of prevalence of diabetes.
The clinical guidelines of the American Diabetes Association (ADA, 2012; Ramírez García & Rodríguez León, 201; Kalinowski, 2013) published in 2012, take a care approach comprehensive that includes primary care, specialized service and social to improve health outcomes [ADA, 2012)].
There is also multiple scientific evidence about the relationship between social determinants of health and glycemic control mediated by access to health care and the multiple challenges facing the homeless population (Walker, et al. (2014).
Due to all of the above, the health promotion approach that used in the present intervention is based on the model ecological social that includes various components and is not limited to personal characteristics and attitudes (intrapersonal levels and interpersonal), but also includes social environments, as well as the institutional, community components (networks informal) and public policy (local, state and local laws and policies and national) (Mc Leroy, et al. 1998).
In this model, the individual is placed in the center of attention. producing interaction with the other elements. For the that this model illustrates the way in which the commitment of the patient, individual responsibility, access to resources in the environment and health education can be connected allowing the development of strategies for the planning of intervention programs [McCormack, Lewis & Rudd, 2017; Kyriakoulis, et al. 2016; Hur & Lee, 2020].
The present study set out to evaluate the effectiveness of an educational intervention on type 2 diabetes to facilitate that homeless people better understand and manage their chronic condition (glycemic control) based on self-monitoring and self-care. The social ecological model was used as the basis to guide educational intervention.
Design and type of study: It was a correlational descriptive study with measurement before and after the intervention educational (Hernández Sampieri, 2014). The data was analyzed to determine if the participants improved their knowledge by comparing the pre-test and post-test assessments to determine the improvement from the beginning of the intervention.
Participants: 250 participants were recruited through a convenience sampling of homeless volunteers with Type 2 diabetes during group meetings at the shelter al that these people attend daily. Each participant is assigned an identification number that was used throughout the
individual documentation to protect your privacy.
Inclusion criteria: Being male or female, of any ethnic origin, able to communicate in English or Spanish, have over the age of 18, homeless and residing in the shelter, have been diagnosed with Type 2 Diabetes and participate in the intervention, sign the informed consent, be mentally adults
competent to understand the instructions provided. For identify participants as mentally competent, the researcher assessed their ability to communicate orally coherently and their ability to read and write.
Exclusion criteria: Minors under 18 years of age, prisoners, people who do not currently reside in the people center homeless or not participating in the supportive intervention anymore established.
Context of the study: The agency where it was carried out the intervention was a clinic-refuge for people without household where the participants attended. The services and the shelter's educational initiatives include counseling on addictions, smoking cessation support and counseling on nutrition and diet to control weight and high blood pressure; however, so far there have been no educational efforts diabetic before this intervention. The intervention included individual and group meetings to discuss approaches healthiest about type 2 diabetes.
Instruments: The Knowledge Questionnaire of diabetes (DKQ-24) as a pre-post assessment for measure knowledge of diabetes (García et al., 2001) that can be managed easily to English and Spanish speakers. The DKQ 24 (reliability 0.78) measures the level of knowledge of diabetes and includes questions that answer yes, no, and no I know, use simple language and written in a way that could be easily read. Each item was scored with two points for yes, one point for no, and zero for answers unknown20. The permissions to use the DKQ-24 were obtained from the original author of the instrument prior to its use in this project.
Data Collection: Demographic indicators were collected (education, access to health care and social support for provide basic information) to verify compliance of the inclusion and exclusion criteria. the collection of data included an initial DKQ-24 questionnaire and the results from the post-intervention survey.
Data analysis: Power analysis was performed based on the calculation of a dependent sample t test where used significance level (α = 0.05), beta power level (β) of 0.80 (1-β), an effect size of 0.5 and a standard error was assumed I (α = 0.05). The results of the satisfaction survey are analyzed to determine areas that need improvement for future educational interventions. All surveys with more than 30% missing data were disqualified from the Project. Data was entered into SPSS version 22.0 for statistical analysis. The normal distribution of the data, the Kolmogorov-Smirnov tests were administered (KS test) and Shapiro-Wilk and the tests of homogeneity of variance, Levene and Brown-Forsyth, and made the Pearson correlation to measure before and after the educative intervention.
Ethical considerations: The research was carried out with the informed consent of the participants and with approval no. IRB 17-OR-372-ME from the Review Board Institutional Board (IRB) of the University of Alabama, United States Joined.
The results of the demographic survey provide information indicating that the demographic characteristics of the participants reflect those of the general population served by the agency. Gender: male 88%, Ethnicity: Hispanic 40%, African Americans 36% and Caucasians 24%; language: English 64%, Spanish 36% All demographic variables such as age, sex and ethnicity are reported in Table 1.
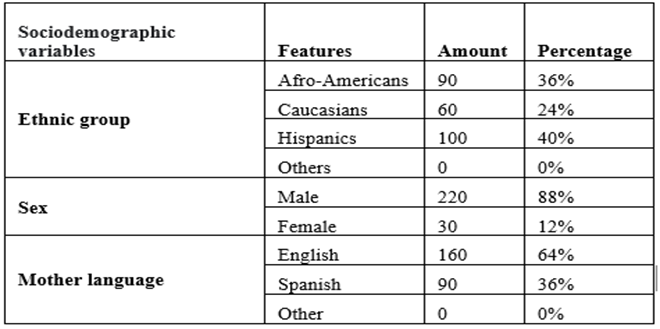
Table 1: Sociodemographic variables n=250
Results of the evaluation before and after through the Diabetes Knowledge questionnaire (DKQ-24) and the survey of satisfaction after the intervention (tables 2, 3 and 4) indicate that there was a significant increase with respect to the average of correct answers per patient between baseline (M = 8.74, SD = 2.91) and answers two months after the intervention educational (M = 14.52, SD = 2.35), t(22) = 7.54, p less than 0.000.
Tables 2, 3 and 4 illustrate the results of the evaluation before and after. There is a significant increase over to the average number of items / questions answered / answered correctly between “before” (M = 9.21, SD = 3.76) and two months “after” the educational intervention (M = 13.96, SD = 4.29), t (23) = 11.73, p less than 0.000. The power reached (1- β) was 98%.
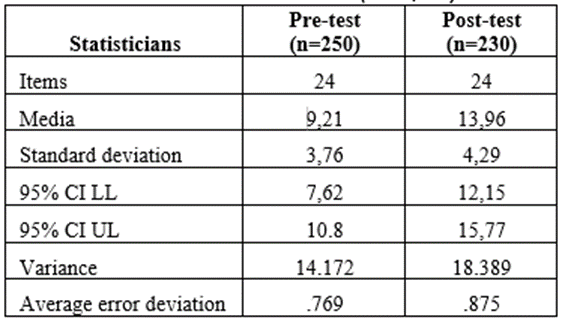
Table 2: Main statistical results (DKQ-24)

Table 3: Paired samples correlation t test

Table 4: Test paired samples
The aim of this study was to determine if the interventions educational courses for homeless people with type 2 diabetes would contribute to improve self-control and self-care of the diabetes and glycemic control.
It was found that the educational intervention had a positive effect with a significance level of p <0>
Homeless people participating in this study increased their knowledge about the causes and treatment of type diabetes 2, proper diet and exercise, learn to recognize the symptoms of hyperglycemia and hypoglycemia and received recommendations about how to treat these conditions. They also increased their knowledge about the complications of diabetes and about resources available in the community from agencies community and government.
These results are consistent with the findings of other studies (Segura Barrios & Barrera Ortíz, 2016; Salazar Estrada et al., 2012), where it was found that people in situations of chronic non communicable disease perceive their quality of life as limited and with discomfort in the physical area especially in terms of energy and mobility. In the social area they feel isolated, dependent and with alterations in their sexual function, while in the psychological order they manifested anxiety, depression, hopelessness and uncertainty, indicating the need for an intervention program in activities physical, recreational, educational and psychological.
Interventions that use programs culturally adapted can help health professionals who provide services to homeless patients to improve the health results.
In several studies (Pérez Delgado et al., 2009; Jordán Severo et al., 2007; Palacios Barahona et al., 2019; Ramón Cabot et al., 2008) where an intervention was performed education to develop knowledge and skills for the self-care and self-control of type 2 diabetes, were obtained significant changes in the development of skills and knowledge about this condition. The findings indicated that preventive, care and intervention programs people with type 2 diabetes should focus on proper management comprehensive, including the context of patients in order to Improve your quality of life. Results that agree with the found in the present study.
On the other hand, one of the complications of type 2 diabetes is obesity, which in patients with this chronic disease increases the risk of morbidity and mortality and has been related to the inadequate eating habits and lack of education in Health. Health education aims to promote the participation of patients to improve their habits and styles of life and for the modification of the Body Mass Index (BMI) in the obese type 2 diabetic.
Due to the above, Cabrera Piraval et al. (2004), carried out a quasi-experimental study with random assignment of two groups of obese diabetic patients. The control group achieved an average value of basal BMI of 33.89 ± 1.96 and at the end of 33.2 ± 2.15 (t: 22.4; p: 0.16), the experimental group obtained an initial value of 33.63 ± 2.12 and final value of 31.54 ± 1.71 (t: 11.55; p = 0.003). Therefore, it was concluded that the educational intervention participation contributes to improve the level of BMI in the obese type 2 diabetics, once again confirming the results found in the present study.
In addition, this type of intervention can raise awareness among the health community on the importance of adapting educational interventions aimed at the homeless population. In this regard, in El Guarco, Costa Rica, Arauz et al., (2001), carried out an investigation on an educational intervention community in patients with type 2 diabetes, directed to the first Level of attention. It was found that the patients do not associate the origin of the disease with family history or with being overweight, which confuse the symptoms of hyperglycemia and hypoglycemia and that there is no homogeneity in the messages of nutrition they receive. It was concluded that the primary level of attention is ideal for executing educational programs on the treatment and early detection of diabetes aimed at patients, their families and healthcare personnel.
Given that many studies have shown that glycemic control improves short and long-term outcomes term of patients with type 2 diabetes, Barceló et al. (2001), carried out a study that consisted of investigating the efficacy of an intervention that included patient education, self-monitoring of blood glucose and determination of glycosylated hemoglobin (HbA1c). It was found that, in the intervention group, compliance with recommendations diet increased from 57.5% at the beginning of the study, to 82.5%, and that in the control group the registered change did not it was significant. In addition, the mean concentration of HbA1c decreased significantly in the intervention group (–0.4 ± 1.1%; P = 0.001), but not in the control group (–0.1 ± 0.1%). It was concluded that the diabetological education of the patient managed to improve metabolic control.
Diabetes education programs should include components to increase empowerment over the diabetes and improve knowledge of diabetes treatment diabetes (Kamimura et al., 2014), especially in the homeless.
It is for this reason that Suarez Pérez et al. (2000), conducted a study with a prospective design that included doctors and nurses who educate the adult diabetic population with diabetes. It was found a significant increase (p < 0>
General improvement was found compare the mean levels of glycosylated hemoglobin at the beginning and at the end of the study and it was concluded that the appearance education is essential to deal with health problems caused by diabetes.
Likewise, Selli et al. (2005) applied a self-care program and health education for patients (n = 88 in the group of intervention n = 101 control group) with type 2 diabetes, following its evolution for five years (1996-2000) and controlling variables such as: blood glucose, weight, index of body mass, blood pressure and foot care.
The differences between the initial and final rates showed reduction for all variables in the group of adherents and for blood glucose and blood pressure for non-adherents.
All this improved in relation to diet control, medication, exercise practice and prevention of diabetic foot, demonstrating the importance of prevention in health and the use of educational interventions in this type of patients.
It is necessary to implement educational interventions more structured and adapted to culture and social contexts to educate vulnerable minority people such as homeless people who have type 2 diabetes. It was found in this study, that the services currently provided by the health agency serving the homeless do not include an educational component to address the management of conditions
chronic, information on lifestyle choices plus and a resource guide for other services available at community.
The educational intervention was directed at the homeless population with type 2 diabetes and addressed this challenge and the results indicate that the project to improve the quality of life can have a positive effect on homeless patients when approached through shelter or community agency level.
The information collected in this study will also help to improve the management of diagnosed homeless people with diabetes, their health outcomes and avoid complications developing a clear understanding of the disease, their treatment and knowledge of available resources.
Based on these results, it is recommended for future projects to continue working on education as the element most important of the promotion and prevention of attention for the homeless with type 2 diabetes. Second, funds and resources are needed to extend and replicate the initiative, providing the services and interventions educational programs that are so needed in this population. Also, the results of the project could be used to promote this type of intervention in funding agencies and health care.
Implications for practice: Use in practice educational interventions professional may have a positive effect on the way of addressing the needs of the homeless patients affected by chronic diseases such as diabetes at the shelter or community agency level. Only through culturally appropriate and tailored interventions and the context will improve health outcomes by preventing complications in developing a clear understanding of the disease, its treatment and knowledge of the resources available. In addition, this intervention can raise awareness among the health care community about the importance of culturally adapt educational interventions aimed at the homeless population.
Limitations and prospective: One of the limitations of this study was the coverage of the homeless population with type 2 diabetes because homeless people come and go, they come and do not comply with a routine that allows them to participate actively and regularly to benefit from the program. In prospective, experimental investigations should be done that allow to measure with greater consistency, reliability, and validity the size of the effect of the educational intervention in the population homeless diabetic.
The authors declare not to have any interest conflicts.
Conceptualization and design: A.M., S.C.M.M., J.C.M.E., A.C.M.B.; Methodology: S.C.M.M., J.C.M.E., A.C.M.B.; Data Acquisition and Software: J.C.M.E., A.C.M.B. Data analysis and interpretation: A.M., S.C.M.M., J.C.M.E., A.C.M.B.; Principal Investigator: A.M. Research: S.C.M.M., J.C.M.E., A.C.M.B. Manuscript writing— Original draft preparation: A.M., S.C.M.M., J.C.M.E., A.C.M.B.; Drafting, review and editing of the manuscript: A.M., S.C.M.M., J.C.M.E., A.C.M.B.; Visualization: J.C.M.E., S.C.M.M. Supervision, J.C.M.E., S.C.M.M. Acquisition of funds: A.M.
self-financed.
Availability for Miami research is appreciated Rescue Mission, Clinic and Shelter, 2015 NW, 1st Ave, Miami, Florida 33127 and Miami Dade College, School of Nursing.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
