
Research Article | DOI: https://doi.org/10.31579/2641-0419/542
1Faculty of medicine and biomedical sciences, University of Yaoundé I, Yaoundé, Cameroon.
2Department of internal medicine, Garoua general hospital, Garoua, Cameroon.
3Department of internal medicine, Yaoundé university teaching hospital, Yaoundé, Cameroon.
4Department of internal medicine, Yaoundé general hospital, Yaoundé, Cameroon.
*Corresponding Author: Hamadou Ba, Faculty of medicine and biomedical sciences, University of Yaoundé I, Cameroon.
Citation: Hamadou Ba, Chris-Nadège NG, Oummoul K. Dewa, Owona Ngabede Amalia, Danwe Dieudonné, et al, (2025), Echocardiographic Assessment and Prognostic Role of Right Ventricular Function in Chronic Heart Failure Patients in Cameroon, J Clinical Cardiology and Cardiovascular Interventions, 8(17); DOI:10.31579/2641-0419/542
Copyright: © 2025, Hamadou Ba. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 December 2025 | Accepted: 22 December 2025 | Published: 26 December 2025
Keywords: chronic heart failure; right ventricular function; echocardiography; prognosis
Aim: this study aimed to assess right ventricular (RV) function by echocardiography in chronic heart failure (CHF) patients, and its prognostic role.
Materials and methods: we conducted a 1-year longitudinal study. Participants were aged ≥21 years, with stable CHF. RV systolic and diastolic functions were assessed with bidimensional, time-motion, and Döppler modes. 6-months outcomes evaluated were all-cause death, or heart failure (HF) hospitalization.
Results: we included 82 patients with a median age of 63 years. The median left ventricular ejection fraction was 36 %. RV systolic dysfunction was observed in 64.6% of patients, while 52.4% had RV diastolic dysfunction. The 6-months mortality rate was 13.4%, and 54.9% had at least 1 HF hospitalization. RV systolic dysfunction was only significantly associated to HF hospitalizations (OR = 2.75 (1.04 – 7.28); p = 0.039).
Conclusion: RV systolic dysfunction is frequent and increases the risk of hospitalization in Cameroonian CHF patients
Chronic heart failure (CHF) is a major public health problem worldwide with an increasing prevalence [1,2]. In 2017, the estimated number of people living with CHF in the world was 64 million [3]. Despite significant improvements in the management and prevention of CHF over the past decades, its related mortality rate remains high. In a community-based study in the United States, Tsao et al reported a mortality rate of 67% for both heart failure with and without reduced ejection fraction during a follow-up period of 20 years [4]. Chronic left heart failure is a complex clinical syndrome which often leads, during its evolution, to right ventricular (RV) dysfunction, resulting from post-capillary pulmonary hypertension thus increasing afterload [5]. However, in most CHF studies, the left heart function is always assessed, while the RV function is often overlooked, although it plays an important role. Recent studies have shown that RV function was a significant predictive factor of mortality related to CHF [6–9]. Consequently, right ventricular function assessment should be an integral part of the management of CHF patients. The right ventricle has a complex anatomy and function, compared to the left ventricle, and thus is better assessed by cardiac magnetic resonance imaging, which is considered as the gold standard method, and sometimes right heart catheterization [10]. However, these tools are not readily available nor accessible in low-and-middle income countries such as Cameroon. We therefore rely on echocardiographic assessment of the right ventricle which is challenging because of the above-mentioned complex morphology, not allowing a good geometric modelization. Nevertheless, a multiparametric echocardiographic approach may help for a better characterization of the global function of the right ventricle [9,10]. This study aimed to assess right ventricular function using echocardiography and to determine its prognostic role in CHF patients in the Yaoundé and Garoua general hospitals.
Study design and setting
We conducted a longitudinal study during 12 months, spanning from August 2023 to July 2024, in the cardiology units of the Yaoundé and Garoua general hospitals, two reference hospitals in Cameroon.
Participants and sampling
We included patients aged 21 years or more, with chronic stable left heat failure, irrespective of the left ventricular ejection fraction. We excluded patient with isolated right heat failure, congenital heart failure, prosthetic heart valve, cardiac pacemaker, pericardial effusion and those with incomplete echocardiographic data.
We performed a non-probabilistic consecutive sampling.
Data collection
We collected data using a predesigned sheet. The data included:
- Sociodemographic characteristics: age, gender, revenue.
- Comorbidities: hypertension, diabetes, dyslipidemia, chronic kidney disease, hyperuricemia, human immunodeficiency syndrome, cancer, pulmonary embolism, anemia, tobacco smoking and alcohol consumption.
- Heart failure stage using the New York Heart Association (NYHA) classification
- harmacologic treatment of CHF and adherence assessed using the Morisky’s questionnaire.
- Blood pressure, heart rate, weight and height.
We used two echocardiographic machines. A General Electric Vivid T9 and a Hitachi Aloka. All the measurements were performed following the 2015 recommendations of the American Society of Echocardiography and the European Association of Cardiovascular Imaging [11].
Left ventricular ejection fraction (LVEF) was measured using the Simpson method. The left ventricular diastolic function was graded using the Appleton classification.
The RV systolic function was assessed using a combination of parameter: two-dimensional fractional area change (2D-FAC), tricuspid annular plane systolic excursion (TAPSE), DTI-derived tricuspid lateral annular systolic velocity (S’) and right ventricular index of myocardial performance (RIMP) or Tei index.
- The 2D-FAC was calculated using the formula: FAC = ((EDA – ESA)/EDA) x 100. It was considered pathological when < 35>
- The TAPSE was measured in the apical 4-chamber view by time-motion mode with the cursor aligned with the lateral tricuspid annulus. It was considered as pathological when < 17mm>
- The DTI-derived tricuspid lateral annular systolic velocity (S’) was measured in the apical 4-chamber view by DTI mode. The cursor was optimally aligned with the lateral tricuspid annulus. It was considered pathological when < 9>
- The RIMP or Tei index was calculated using the formula: RIMP = (IVCT + IVRT)/ET. Measurements were done in the apical 4-chamber view using DTI velocity at the lateral tricuspid annulus. The isovolumic contraction time (IVCT), isovolumic relaxation time (IVRT), and ejection time (ET) intervals were measured from the same heartbeat. Value of Tei index > 0.54 were considered as pathological.
RV diastolic function was assessed using the tricuspid E/A and E/E’ ratios.
- Tricuspid E/A ratio: obtained by measuring tricuspid E and A velocities in the apical 4-chamber view by pulse wave Doppler with the cursor placed at the tip of the tricuspid valve leaflets. It was considered as pathological when < 0> 1.2. The E wave deceleration (EDT) time was also measured.
- Tricuspid E/E’ ratio: the E’ wave velocity was obtained in the apical 4-chamber view by DTI mode. The cursor was aligned with the lateral tricuspid annulus. It was considered pathological when > 6
RV diastolic dysfunction stages were classified as follows:
- Altered relaxation: E/A ratio Less-than sign 0.8
- Pseudo-normal pattern: E/A ratio between 0.8 and 1.2, and E/E’ ratio > 6
- Restrictive pattern: E/A ratio > 1.2 and EDT < 120ms>
Furthermore, we made an echocardiographic estimation of pulmonary vascular resistance (PVR) by dividing the tricuspid regurgitation velocity (TRV) by the velocity-time integral in the right ventricular outflow track (RVOT): PVR = TRV/VTI (RVOT). PVR was expressed in Woods units, and considered abnormal when it was > 2 [12].
Follow-up
The participants were followed-up in office consultation on M1, M3 and M6, and by phone calls on M2, M4 and M5.
During office consultations, data collected during were the following:
- Occurrence or aggravation of signs and symptoms of heart failure, and change in vital parameters leading to the modification of heart failure treatment or hospitalization.
- Medication adherence: monitored using 8-item Morisky medication adherence scale. A score of 8 indicated a high adherence, 6 to 7 medium adherence, and Less-than sign 6 low adherence.
During phone calls, we asked the participants if they had symptoms of heart failure, and encouraged them to have good medication adherence.
Participants who did not present for office consultations, and who were unreachable on phone were considered as lost to follow-up.
Prognostic criteria were all-cause mortality, and hospitalization for heart failure.
We performed statistical analysis using Statistical Package for Social Sciences software version 23.0. We used the Chi-square test for the comparison of proportions. The Fisher exact test was used where appropriate. The Mann Whitney test was used for the comparison of medians, logistic regression for multivariate analysis. We analyzed factors associated to RV systolic and diastolic dysfunction. The first step consisted of the univariate analysis including the following variables: gender, age, heart failure duration, left ventricular ejection fraction, left ventricular diastolic dysfunction, pulmonary artery systolic pressure, pulmonary vascular resistance, basal RV diameter, and medication adherence. The second step was a logistic regression of all variables with significant p-values in univariate analysis. Data of participants lost to follow-up were not included in mortality analysis. We also did not include in the analysis of hospitalization the data of participants who had never been hospitalized before their lost to follow-up. A p-value Less-than sign 0.05 was considered as statistically significant.
This study was conducted in accordance to with the declaration of Helsinki. We obtained an ethical clearance N°1007/UY1/FMSB/VDRC/DAASR/SCD from the institutional ethical review board of the faculty of medicine and biomedical sciences of the university of Yaoundé I.
We included 82 patients (48.8% women) in the study. The median age was 63 [52 – 71] years. The baseline characteristics of the study population are presented in table I. Hypertension was the most frequent comorbidity. Hypertensive and ischemic cardiopathies as well as dilated cardiomyopathy were the most frequent etiologies of CHF. Most participants were classified NYHA II. Two third of the participants had heart failure with reduced ejection fraction (HFrEF). All classes of guideline-directed medical therapy were used in various proportions, and medication adherence was high in two third of participants.
| Variables | Categories | Number (N=82) | Percentage (%) |
| Gender | Male | 42 | 51.2 |
| Female | 40 | 48.8 | |
| Left heart failure etiologies | Hypertensive cardiopathy | 43 | 52.4 |
| Ischemic cardiopathy | 21 | 25.6 | |
| Dilated cardiomyopathy | 10 | 12.2 | |
| Valvular heart disease | 5 | 6.1 | |
| PPCM | 3 | 3.7 | |
| NYHA stage | II | 50 | 61.0 |
| III | 26 | 31.7 | |
| IV | 6 | 7.3 | |
| LVEF | < 40> | 53 | 64.6 |
| ≥ 40 | 29 | 35.4 | |
| Medications | Diuretic | 74 | 89.0 |
| Betablocker | 69 | 83.1 | |
| ACEi/ARB | 60 | 73.2 | |
| MRA | 42 | 50.6 | |
| SGLT2i | 23 | 27.7 | |
| Sacubitril-valsartan | 14 | 16.9 | |
| Medication adherence | High | 52 | 64.4 |
| Medium | 19 | 23.2 | |
| Low | 11 | 13.4 | |
| Comorbidities | Hypertension | 61 | 74.4 |
| Low physical activity | 48 | 58.5 | |
| Alcohol consumption | 20 | 24.4 | |
| Diabetes | 15 | 18.3 | |
| Obesity | 14 | 17.1 | |
| Dyslipidemia | 11 | 13.4 | |
| Tobacco smooking | 10 | 12.2 | |
| Chronic kidney disease | 8 | 9.8 |
Table I: Baseline characteristics of the study population
PPCM: peripartum cardiomyopathy NYHA: New York Heart Association LVEF: left ventricular ejection fraction ACEI: angiotensin converting enzyme inhibitor ARB: angiotensin receptor blocker MRA: mineralocorticoid receptor antagonist SGLT2I: sodium/glucose cotransporter 2 inhibitor
In table II we reported the findings of morphologic, and functional echocardiographic assessment of the right ventricle. There was no significant difference between men and women. Abnormalities of at least one parameter of RV systolic function were present in 53 participants (64.6%). The Tei index was the most frequently altered parameter followed successively by the 2D-FAC, the TAPSE and the DTI-derived tricuspid lateral annular systolic velocity (Figure 1). RV diastolic dysfunction was present in 43 participants (52.4%) with abnormal relaxation in most cases (Figure 2).
| Variables | Men | Women | p |
| RV basal diameter | 40 [31 – 47] | 35 [30 – 45] | 0.348 |
| Proximal RVOT in PSLA | 32 [29 – 40] | 32 [30 – 37] | 0.662 |
| Proximal RVOT in PSSA | 34 [28 – 37] | 33 [27 – 37] | 0.670 |
| Distal RVOT in PSSA | 26 [22 – 28] | 24 [21 – 26] | 0.373 |
| PA diameter | 24 [20 – 28] | 24 [20 – 26] | 0.659 |
| Basal RV thickness | 4 [4 – 5] | 4 [3 – 4] | 0.067 |
| RV/LV ratio | 0,76 [0,62 – 0,98] | 0,77 [0,63 – 0,92] | 0.898 |
| RA surface | 19 [16 – 25] | 19 [17 – 23] | 0.686 |
| TAPSE | 18 [13 – 21] | 17 [13 – 22] | 0.762 |
| S’ | 11,0 [8,0 – 12,9] | 10,0 [8,3 – 13,0] | 0.907 |
| 2D-FAC | 32 [21 – 43] | 34 [21 – 46] | 0.534 |
| Tei index | 59 [45 – 73] | 59 [46 – 79] | 0.926 |
| E/A ratio | 0,89 [0,69 – 1,20] | 1,07 [0,73 – 1,36] | 0.269 |
| E/Ea ratio | 5 [4 – 7] | 5 [3 – 6] | 0.722 |
| EDT | 160 [116 – 216] | 188 [119 – 276] | 0.252 |
Table II: parameters of right ventricular morphologic and functional assessment
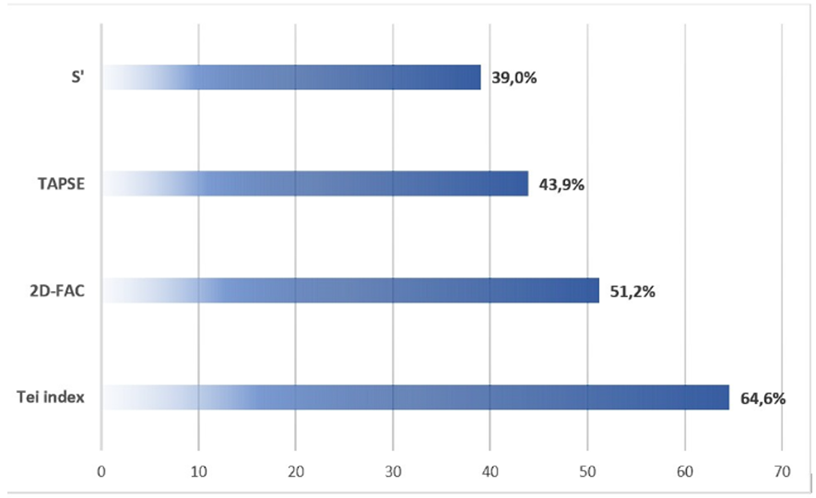
Figure 2: Proportions of abnormal right ventricular systolic function parameters
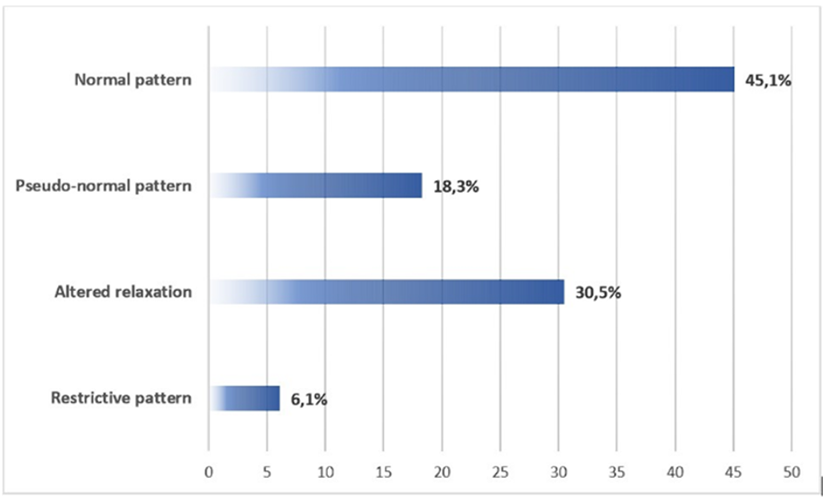
Figure 2: Proportion patterns of right ventricular diastolic function
At six months follow-up, half number of participants had presented at least one hospitalization for congestive heart failure. The triggers of depensation were infections (41.0%), poor adherence to treatment (37.0%), anemia (11.0%), and arrythmia (4.1%). The trigger of decompensation was unidentified in 6.9% of participants. The mortality rate was 13.4%. RV systolic dysfunction was significantly associated with hospitalizations for heart failure but not to all-cause mortality (Table III). There was no significant association between RV diastolic dysfunction and neither hospitalizations for heart failure nor all-cause mortality. RV systolic dysfunction was independently associated with LVEF Less-than sign 40 Percent sign (Table IV).
| All-cause mortality | Hospitalizations | |||
| No (n=62) | Yes (n=11) | No (n=30) | Yes (n=45) | |
RV systolic dysfunction Yes No |
38 (61.3) 24 (38.7) |
8 (72.7) 3 (27.3) |
15 (50.0) 15 (50.0) |
33 (73.3) 12 (26.7) |
| OR (95% CI) | 1.68 (0.41 – 6.98) | 2.75 (1.04 – 7.28) | ||
| p | 0.736 | 0.039* | ||
RV diastolic dysfunction Yes No |
36 (58.1) 26 (41.9) |
4 (36.4) 7 (63.6) |
17 (56.7) 13 (43.3) |
23 (53.5) 20 (46.5) |
| OR (95% CI) | 0.41 (0.11 – 1.56) | 0.88 (0.34 – 2.25) | ||
| p | 0.207 | 0.788 | ||
Table III: Assessment of the association between prognostic factors and right ventricular dysfunction
RV: right ventricular OR: odds ratio CI: confidence interval *significant
| All-cause mortality | Hospitalizations | |||
| No (n=62) | Yes (n=11) | No (n=30) | Yes (n=45) | |
RV systolic dysfunction Yes No |
38 (61.3) 24 (38.7) |
8 (72.7) 3 (27.3) |
15 (50.0) 15 (50.0) |
33 (73.3) 12 (26.7) |
| OR (95% CI) | 1.68 (0.41 – 6.98) | 2.75 (1.04 – 7.28) | ||
| p | 0.736 | 0.039* | ||
RV diastolic dysfunction Yes No |
36 (58.1) 26 (41.9) |
4 (36.4) 7 (63.6) |
17 (56.7) 13 (43.3) |
23 (53.5) 20 (46.5) |
| OR (95% CI) | 0.41 (0.11 – 1.56) | 0.88 (0.34 – 2.25) | ||
| p | 0.207 | 0.788 | ||
Table IV: Multivariate analysis of factors associated with right ventricular systolic dysfunction
RV: right ventricular OR: odds ratio CI: confidence interval LVEF: left ventricular ejection faction PASP: pulmonary artery systolic pressure
This study aimed to determine the prognostic value of RV function assessed by echocardiography in CHF patients in Cameroon, were other work-up such as cardiac magnetic resonance imaging, and biomarkers are not readily available, and most patients unable to afford them in the absence of universal health coverage. Our participants similarity as found by previous authors in Cameroon [13–16]; were relatively young with approximately 10 years difference as compared to CHF patients in high income countries [17,18]. This can be explained by the limited access to health services in Cameroon, which can lead to late management of risk factors, leading to early onset heart failure. Hypertension was the most frequent comorbidity. It is the predominant cardiovascular risk factor in Africa where its prevalence reaches 42% [19]. Hypertension which is asymptomatic at early stages often goes undiagnosed and undertreated in our milieu, leading inexorably to complications such as CHF. This fact can explain why hypertensive cardiopathy most prevalent in our sample, contrasting with the pattern in high income countries where ischemic heart disease is the leading cause of CHF [20]. Heart failure with reduced ejection fraction was more frequent is our study population, and corroborate the data from a large European registry reporting 60% of HFrEF phenotype [21]. Concerning RV systolic dysfunction, the prevalence we obtained is close to those reported by Meluzin et al in Czechia, and Menanga et al in Cameroon [13,22]. They reported respectively 70% and 81.6%. In contrary, Venner et al in France, and Shaker et al in Egypt found lower prevalences, respectively 25% and 48.7% [23,24]. These disparities may be explained by different study populations (only HFrEF patients included in the latter studies), and different definitions of RV systolic dysfunction. RV systolic dysfunction was based on --TAPSE, S’ and 2D-FAC in the study of Shaker et al, while it was only base on TAPSE in the Study of Venner et al. Concerning RV diastolic function, data in the literature is very scarce. However, Sumin et al in the USA also found in 2021 that approximately half of the participants with ischemic heart failure with preserved ejection fraction had RV diastolic dysfunction [25]. The multivariate analysis showed an association between RV systolic dysfunction and LVEF < 40>
This study has some limitations. First as mentioned in the discussion section, our sample size and follow-up period were respectively small and short, thus decreasing the statistical power. Secondly, we were unable to perform RV strain and magnetic resonance imaging because of unavailability for the first modality, and financial constrains for the second.
Chronic heart failure patients frequently present right ventricular dysfunction, particularly those with reduced left ventricular ejection fraction. Right ventricular systolic dysfunction was found to be independently associated with hospitalization for worsening heart failure, but not with all-cause mortality. Right ventricular function assessment should be systematically integrated in the management of heart failure patients.
Hamadou B, Nganou-Gnindjio C-N, Oummoul Koulsoumi D, and Owona Ngabede A: study design. Oummoul Koulsoumi D: data collection. Djantio Noundou H J, Oummoul Koulsoumi D, and Danwe Dieudonné: statistical analysis; Oummoul Koulsoumi D, and Danwe Dieudonné: manuscript drafting. Hamadou B, and Menanga A P: supervision.
The authors declare no conflict of interest.
No funding was received for this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
