
Research article | DOI: https://doi.org/10.31579/2641-0419/234
1Cardiothoracic Centre, All India Institute of Medical Sciences, New Delhi, India.
2Department of Cardiothoracic Surgery, All India Institute of Medical Sciences, Himachal Pradesh, India.
*Corresponding Author: Ujjwal Kumar Chowdhury, MCh, Diplomate NB ProfessorDepartment of Cardiothoracic and Vascular Surgery All India Institute of Medical Sciences Ansari Nagar, New Delhi-110029, INDIA.
Citation: Shikha Goja, Lakshmi Kumari Sankhyan, Ujjwal K. Chowdhury, Niraj N. Pandey., Sudheer Arava., et all (2022). Echocardiographic and Computed-tomographic Evaluation of the Fate of Bovine Pericardial Patch as a Pericardial Substitute in Bentall’s Procedure: Twenty-year’ Results. J. Clinical Cardiology and Cardiovascular Interventions, 5(1); DOI:10.31579/2641-0419/234
Copyright: © 2022 Ujjwal Kumar Chowdhury, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 November 2021 | Accepted: 30 December 2021 | Published: 06 January 2022
Keywords: annuloaortic ectasia; aortic dissection; bentall’s procedure; bovine pericardial patch; pericardial calcification
Objective: The study was designed to ascertain the influence of usage of bovine pericardial patch in patients undergoing Bentall’s procedure with respect to reexploration for bleeding, mediastinal infection, avoidance of conduit adhesions, late development of pericardial constriction and calcification.
Materials and Methods: We reviewed 150 patients (79 males) aged between 22 to 68 years (mean±SD 49.25±12.9 years) receiving a composite aortic conduit between January 1998 to December 2020 for annuloaortic ectasia (n=100), aortic dissection (n=49), and dilated aortic root in repaired tetralogy of Fallot (n=1). Twenty-five patients had Marfan’s syndrome. Modified “button technique” was performed by interposing a glutaraldehyde treated pericardial strip at the graft coronary anastomoses, and proximal aortic conduit suturing using interlocking interrupted, pledgeted mattress suture. On completion, the pericardial cavity was reconstructed using St. Jude Medical Biocor pericardial patch. To detect evidence of pericardial constriction, survivors underwent echocardiography and computed tomography. The Kaplan-Meier curve was drawn to show the probability of survival over a period of follow-up time.
Results: Seven (4.7%) patients died of cardiac-related cause, 45% had transient hemodynamic instability, 55% had low cardiac output, and 87.1% had spontaneous return of sinus rhythm. The average 12-hour postoperative drainage was 245±70 ml and there was no mediastinal infection. At a mean follow-up of 172.4 (SD± 58.9) months, the actuarial survival was 94.2±0.04% (95% CI: 88.5-96.8), and there was no pericardial constriction or calcification.
Conclusion: Reconstruction of pericardial cavity using Biocor bovine pericardial patch minimizes diffuse oozing of blood, graft infection, and is not associated with later development of pericardial constriction, or calcification.
Since the introduction of glutaraldehyde by Alain Carpentier, bovine pericardium and other biological tissues have been used in clinical practice for the past 50 years. The biological tissues when subjected to low concentration of glutaraldehyde loses its antigenicity, does not induce the formation of antibodies, and produces the disruption of intra- and intermolecular protein, enhancing its structural stability, and maintaining sterility. [1-4]
The glutaraldehyde-treated bovine pericardium is one of the biological materials widely used in cardiovascular surgery as a patch material for aorta, pulmonary arteries, medium sized vessels, bioprosthesis valve leaflets, for repair of intracardiac defects, small vascular substitutes, and neoaortic reconstruction. The non-cardiac usage has been during tracheal reconstructive surgery, repair of diaphragmatic defects, and suture line reinforcement during lung volume reduction procedures, cholangioplasty, and inguinal hernia repair. [2,3,5-21]
Literature documents isolated case reports on successful use of bovine pericardium in infected surgical field, namely, patch arterioplasty, and patch reconstruction of the mitral annulus following infective endocarditis.[22] However, larger case series as well as long-term results of use of this biomaterial in presence of infection is not available.[13,21,23-28]
The original Bentall’s procedure employed an in situ circumferential suture line around the coronary ostia, then complete aortic wrap around to control bleeding. Tension developing at the suture line of the side-to-side coronary anastomosis and/or blood accumulation within the perigraft space conveyed significant risk of coronary artery dehiscence, pseudoaneurysm formation and reoperation.[29,30] Hematoma in the space may additionally compress the graft or cause prosthetic valve dysfunction.[31-33]
To avoid this complication, Cabrol used a fistula to the right atrial appendage and subsequently adopted interposition Dacron conduits to the coronary ostia with the new risk of graft thrombosis and persistent aorto-right atrial fistula.32 For these reasons, a modified open technique was developed by Kouchoukos and associates in 1986 that eliminated the prosthetic wrap and allowed reattachment of adequately mobilized coronary buttons to the graft with tension free sutures. [29]
Despite technical improvements in coronary arterial reconstruction by the “open button technique”, graft-coronary anastomotic bleeding, bleeding from proximal and distal aortic conduit suture line, pseudoaneurysms of the coronary ostia anastomoses, pseudoaneurysms of the proximal and distal suture lines continue to occur because of fragility and reduced tissue quality of the ascending aortic wall and connective tissue abnormality. [20,31,34-41]
To address these concerns, we interposed a glutaraldehyde-treated autologous pericardial strip between the graft and native coronary ostia during coronary ostial implantation and placed interlocking, interrupted, pledgeted mattress sutures to ensure perfect hemostatic proximal aortic suture lines. The technical details and long-term results of coronary ostial and distal aortic anastomoses following modified Bentall’s procedure have been addressed in our previous publications. [42-46]
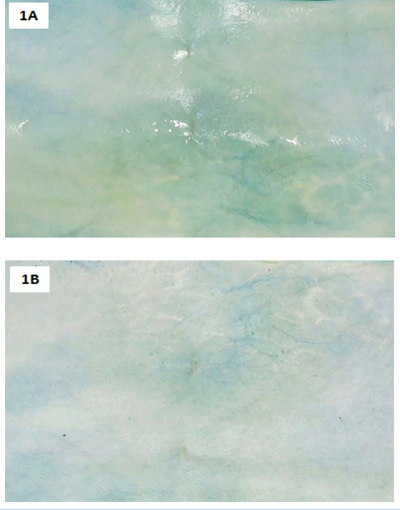
Since the native pericardium was harvested for creating coronary buttons, bovine pericardium was used to cover the cardiac chambers and great vessels, including the conduit. From 1998 onwards, we reconstructed the pericardial cavity using a bovine pericardial patch to reduce/eliminate diffuse oozing from multiple needle holes and graft interstices, prevent the formation of postsurgical adhesions between the conduit and sternum, and as a protective material against graft inoculation (Figures 1A, 1B).
Bovine pericardium is preferred because it’s biocompatible, less antigenic, resistant to infection and acellular comprising essentially of pure collagen which may provide a natural microenvironment for host cell migration and proliferation, accelerating endothelization and tissue regeneration. [5-21]
Bovine pericardium is thoroughly washed and sutured with the rough surface facing intrapericardial side. Experimental data have demonstrated formation of covering layers with more plasticity, producing greater tension resistance and expansion when the rough face was placed intraluminally towards the vessel lumen, thus preventing aneurysmal dilation. [47]
The technical details of coronary button implantation, the long-term fate of coronary ostial and distal aortic anastomoses, and the myocardial preservation strategies of this group of patients have already been addressed in our previous publications. The same is not repeated here. [42-46] In this retrospective study, we present the very late-term (20 years) results evaluating: i) any reduction of diffuse bleeding and perioperative prosthetic graft infection, ii) the stability of newly reconstructed pericardial cavity over time, and iii) the fate of bovine pericardial patch in terms of thickening, constriction, and calcification assessed using echocardiography and computed tomography.
This study conforms to the principles outlined in the declaration of Helsinki of 1975, as revised in 2008. Between January 1998 to June 2021, 150 consecutive patients (79 males), aged 22-68 years (mean 49.25±12.9 years) underwent modified Bentall’s operation using the surgical techniques described after obtaining informed consent and institutional ethics committee approval. This is the total number of Bentall’s procedure done by the corresponding author in the last 23 years, and all patients are included in this study. Literature does not document any other studies citing the use of bovine pericardium as a pericardial substitute in patients undergoing Bentall’s procedure. Therefore, the total number of operated patients in this study is totally based on subjective assessment by the corresponding author. Indication for surgery included annuloaortic ectasia (n=100), type A aortic dissection (n=49) and dilated aortic root following intracardiac repair of tetralogy of Fallot (n=1). Moderate to severe aortic regurgitation was seen in 144 (96%) patients, 6 (4%) patients had grade II mitral regurgitation, and 105 (70%) patients had left ventricular ejection fraction <0>Table 1.
Echocardiography
Transthoracic two-dimensional, color-flow Doppler echocardiography (Philips iE33 echo machine; Philips X7-2T probe, Bothell, WA, USA) was performed to measure mitral, tricuspid, superior vena cava, hepatic vein, pulmonary venous flow velocities, prosthetic valve motion, and transprosthetic gradients. Mitral or tricuspid regurgitation was assessed semiquantitatively as grade 1+ to 4+. Ejection fraction was calculated with a modification of the method of Quinones and colleagues. [48] A constrictive pattern was defined as pericardial thickening >4mm, 25% or greater increase in mitral E-velocity with respiration, and an augmented (25% or more) diastolic flow reversal in the hepatic vein after the onset of expiration compared with the inspiration phase.[49,50]
Techniques of computed tomography
Non contrast high pitch spiral acquisition was performed using a dual source computed tomography scanner (Somatom flash/ force, Siemens Healthcare, Forchheim, Germany). The scan was acquired in a craniocaudal direction, from above the level of carina upto the diaphragm.
Thin axial sections (1.0 mm, increment 0.6 mm) were reconstructed using a medium-soft convolution kernel (B26). All reconstructed images were transferred to an external dedicated workstation (syngo.via, Siemens Healthcare, Forchheim, Germany) where multiplanar reformations, and volume rendered images were evaluated alongside axial images.
Surgical techniques
Intraoperative transesophageal echocardiography was performed with a Hewlett-Packard Sonos 1500 or 5500 ultrasound system on all patients. Standard anaesthetic and operative techniques were used throughout the study period. The operations were performed under moderately hypothermic cardiopulmonary bypass through arterial cannulation (axillary artery n=28; femoral artery n=122) and bicaval venous cannulation of femoral vein and superior caval vein.
A retrograde coronary sinus cannulation with self-inflatable balloon (RCO 14, Edwards Lifesciences, Irvine, CA, USA) was done using transatrial blind cannulation in 100 patients. In cases of difficult cannulation (n=50), the coronary sinus was cannulated through a short right atriotomy under direct vision. Proper placement was confirmed by observing distension of posterior interventricular vein, maintenance of coronary sinus pressure, palpation of coronary sinus cannula posteriorly at the base of heart and transesophageal echocardiography.[51] No coronary sinus anomalies or coronary sinus injuries were confronted.
Ultrafiltration was used in all patients during and after cardiopulmonary bypass to reduce the total body water, potassium overload and to remove the inflammatory mediators from the circulation, maintaining hematocrit more than 25% on cardiopulmonary bypass.
All patients were subjected to the “integrated myocardial preservation management” strategy using intermittent antegrade direct ostial cardioplegia and retrograde coronary sinus cardioplegia infusion.[52] Cardioplegic infusions by both routes were never given simultaneously.
A dacron composite graft with a mechanical heart valve [(St. Jude Medical Inc.; Minn); (Conduit 25 mm (n=60); 27 mm (n=55); 29 mm (n=35)) was used in all patients. While creating the coronary buttons, the pericoronary diseased aortic tissue was excised leaving behind a cuff of 10-12 mm.
All patients in the study underwent “modified button technique” for reconstruction of the coronary arteries and proximal conduit suturing for perfect hemostasis (Figures 2A-2I).
The technical details of the composite aortic graft replacement, the fate of the coronary ostial, and distal aortic anastomoses, and the myocardial preservation strategies have been enumerated in detail in our previous publications.42-46 The composite graft was sutured to the annulus using everted, interrupted 2-0 sutures over polytetrafluoro-ethylene pledgets. Each interrupted aortic supra-annular sutures were placed in such a fashion that successive sutures were made to pass through the previous pledget; thus ensuring perfect aortic annular hemostasis (Figures 2A, 2B). Using graft cautery, two side holes were created on the composite graft measuring around 10mm in diameter in the proposed area of coronary ostial implantation. The left and right coronary buttons were anastomosed in an end-to- side fashion with continuous 5-0 polypropylene suture to openings on the composite graft. While suturing, a long strip of glutaraldehyde treated pericardium, about 1 cm wide was interposed circumferentially around each graft-coronary button anastomosis (Figures 2C-2H). During construction of the inferior portion of the ostial anastomoses, the continuous retrograde perfusion was transiently lowered to avoid flooding and performing perfect hemostatic suturing under vision.
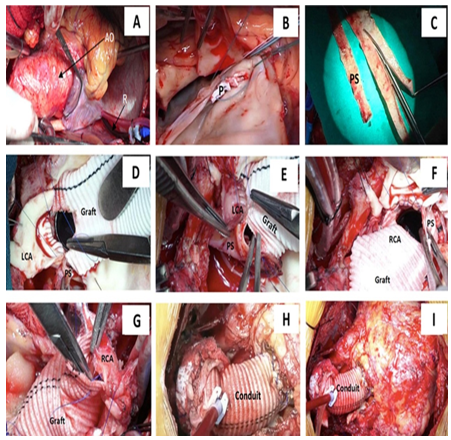
The right coronary button was anastomosed at a relatively high position of the composite graft taking into consideration the collapsed state of the right ventricle during cardioplegic arrest. We used topical thrombin (Tisseel, Baxter AG, Vienna) as an additional topical hemostatic agent on all patients.
Mean cross-clamp time was 114.6±28.4 min (range, 90-187 minutes) and mean cardiopulmonary bypass time was 156.0±29.6 min (range, 136-220 min).
Following removal of aortic cross-clamp, majority of the patients (n=132, 87.2%) returned to normal sinus rhythm. Only 18 (12.8%) patients required antegrade administration of injection adenosine and 200-250ml warm hotshot blood cardioplegia for spontaneous defibrillation. Direct current cardioversion was not used on any patient. We used atrioventricular sequential pacing for 24-48 hours in patients with low heart rate.
On completion of the Bentall’s procedure a segment (15 x 10 cm) of bovine pericardium (SJM BiocorTM Pericardial Patch, St. Jude Medical, St. Paul, MN, USA) was used to cover the cardiac chambers and great vessels including the valve conduit (Figures 1A, 1B).
Statistical Analysis
Statistical analysis was performed using Intercooled STATA 14.0 Software (College Station, Texas, USA). Interval related data were expressed as mean ± standard deviation (SD) or median (minimum-maximum) and categorical variables were expressed as percentages. The Kaplan-Meier curve was drawn to show the probability of survival over a period of follow-up time. The results were expressed as probability of survival (95% confidence interval) at various time intervals. Statistical significance was set at p<0>
Short-term outcomes
There were 7 (4.7%) early deaths due to low cardiac output syndrome with multiorgan failure and superimposed sepsis between 10th to 18th postoperative days. These patients had acute type A aortic dissection and were in congestive cardiac failure preoperatively (Table 1).

Patients who needed moderate amount of inotropes (usually dopamine and/or dobutamine hydrochloride, 5 µg/kg/min) for less than 24 hours postoperatively were considered as having transient postbypass hemodynamic instability (n=72). In contrast, patients who required inotropic agents, vasopressors and/or intra-aortic balloon counterpulsation for more than 24 hours postoperatively were categorized as having a true low cardiac output syndrome (n=78).
Five patients required intraoartic balloon counterpulsation as an additional support of which three patients survived. The incidence of low cardiac output syndrome remained fairly constant over the course of the study.
Morbidity
Hospital morbidity included re-exploration for excessive bleeding from non-anastomotic sites within 12 hours in 8 patients with acute type A aortic dissection. The average 12-hour postoperative drainage was 245±70 ml. Twelve (9.2%) patients required tracheostomy and long-term ventilator support. Hospital stay ranged from 7 to 54 days (median, 9 days; mean, 20±7 days). Three patients were readmitted on 18th, 21st and 22nd days postoperatively had deranged prothrombin time and required pericardiocentesis.
Long-term outcomes
There were 3 (2%) late deaths at 15 and 69 months after surgery due to intractable ventricular arrhythmias and anticoagulant-related intracranial bleed respectively. Follow-up was 100% complete (1-226 months) and yielded 1218 patient-years of data. At a mean follow-up of 172.4 (sd± 58.9) months, the actuarial survival was 94.2±0.04% (95% CI: 88.5-96.8). All survivors were in New York Heart Association I or II at their last follow-up. Two patients required thoraco-abdominal aortic graft replacement with re-implantation of celiac, superior mesenteric and right renal arteries 3 years following Bentall’s procedure. No survivors had structural deteriorations, pseudoaneurysm formations or thromboembolic complications.
Peri-operative myocardial infarction and arrhythmias
No patients sustained a perioperative myocardial infarction. Postoperatively, 16 (10.7%) patients had supraventricular arrhythmias, 8 (5.4%) had premature ventricular contraction, 2 (1.3%) had ventricular tachycardia, 14 (9.3%) had left bundle branch block, and 10 (6.7%) had junctional rhythm. No patient had complete heart block.
Postoperative studies and results
Cohort of survivors
All survivors (n=140) were examined and studied between December 2019 and June 2021, which was the closing interval of the study. Postoperative evaluation consisted of clinical examination, electrocardiogram, chest radiograph, cine fluoroscopy, echocardiography and computed-tomographic angiography. The functional class at follow-up was noted. All patients received warfarin and aspirin (100 mg/day) for anticoagulation to maintain INR between 2.5 to 3.5. Digoxin and diuretics were weaned at varying time intervals. Amiodarone was used for intractable atrial fibrillation.
Postoperatively, the left ventricular ejection fraction increased from 50%±9.2% (range 15% to 62%) to 58%±6.2% (range 15%-70%). Thirty-nine (26%) patients had left ventricular ejection fraction ranging between 15% and 25%.
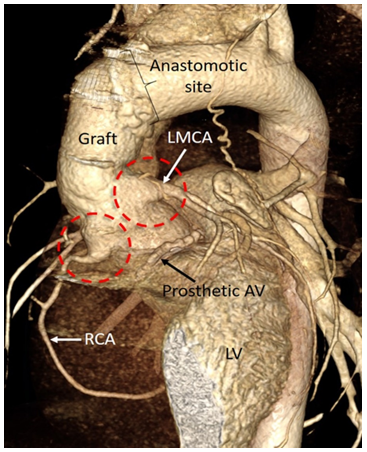
At a mean follow-up of 172.4±58.9 months, none of the survivors demonstrated anastomotic complications involving the coronary ostia or the distal aortic arch. All patients demonstrated patent coronary ostia and with no coronary aneurysm, kinking or pseudoaneurysm formation of the newly implanted coronary arteries (Figure 3). None of the survivors had either constrictive pericarditis or pericardial calcification.
The present study is the first to our knowledge to determine the very late-term (20 years) results of bovine pericardium as a pericardial substitute in the setting of Bentall’s operation. The study provided several interesting findings: i) no patient exhibited clinical or echocardiographic features of constrictive pericarditis, ii) computed-tomography did not reveal any instances of pericardial thickening or calcification and iii) the average postoperative drainage volume was 249±65 ml in the first 12 hours following surgery, with no instance of graft/mediastinal infection on any patient.
The quest to establish a pericardial substitute that is durable for 20-25 years without causing any pericardial adhesions, and adverse hemodynamics continues. Various biologic or synthetic sheets such as absorbable polymer patches, three-layered synthetic pericardial substitutes, and expanded polytetrafluoroethylene have been used as a pericardial substitute.[52-54] However, there have been no documented adequate substitutes that reduces postsurgical adhesions.[53] Prevention of adhesions through pericardial substitution has therefore become a matter of investigation.[55]
Bovine pericardium has come into common clinical use during the past 50 years, especially when used as a patch for arterial closure during vascular and cardiac surgery. Technical merits that have led to widespread adoption of bovine pericardial patches in the operating room, include easy handling, less suture bleeding and the ability to immediately perform arterial duplex examination at the site of angioplasty.[5-21] However, long-term results of this biomaterial are poorly documented and need cautious interpretation as to whether its long-term performance is related to the material itself or to the operation in which it is used.[1,13,14]
Experimental basis and clinical applications of bovine pericardium as a biomaterial
The advantages of bovine pericardium as a cardiovascular patch can be divided into clearly observed and documented advantages, and benefits that are not well documented so far. The clearly documented advantages are: i) biocompatibility; ii) minimized antigenicity, increased strength and stability due to pretreatment using glutaraldehyde; iii) dependable suture retention due to consistent processing with 0.5 mm thickness pericardium; iv) reduced potential infections; v) increased long-term durability; vi) similarity of compliance of bovine pericardium and native artery/prosthetic conduit; and vii) feasibility of insonation with ultrasound immediately after implantation due to lack of air spaces and solidity.[3,21,25,26,57-59]
Although being used in clinical practice, there are instances where benefits of bovine pericardium not as well documented, for example: i) use of bovine pericardium as a vascular patch of medium sized arteries namely, carotid, femoral, and popliteal arteries following embolectomy or endarterectomy, ii) closure of intracardiac defects like atrial and ventricular septal defects,[5,7,17] iii) repair of arteriotomy in the presence of infected field despite lack of evidence of it being bacteriostatic or bactericidal,11,12 and iv) claim of some manufacturers that bovine pericardium possess anticalcification technology that can significantly reduce calcification, and support endothelization.[8,9,27,6-65]
Bovine pericardium being an acellular material of essentially pure collagen, may provide a natural microenvironment for host cell migration, and proliferation, accelerating endothelization, and tissue regeneration.[66,67] Since primary closure of a longitudinal arteriotomy may result in restenosis due to neointimal hyperplasia, patch arterioplasty is advocated to prevent this complication. Most commonly, patch angioplasty is performed after carotid endarterectomy and in femoral and popliteal arteries following thrombectomy or embolectomy. Meta-analysis provides strong evidence that carotid patching provides both perioperative and long-term benefits after carotid endarterectomy.[8,9,11,27,61-63,65,68-74]
Published literature is divided on the selection of patch material for carotid endarterectomy. Vein patch angioplasty ideally should have the lowest incidence of postoperative thrombosis due to an intact endothelium, an inherent suppleness and natural compliance. Several investigators have reported equally encouraging results using bovine pericardial patch and synthetic patches.[61,69-72]
Although there are morphological similarities, the molecular and cellular pathways that stimulate intimal hyperplasia in these clinical circumstances may be different. The biological signaling pathways that activate vascular healing after patch angioplasty depend on cells that infiltrate the patch and different patches may have different biological responses and therefore may need different types of treatment.[8,9,11,27,61-63,65,68-74]
Although scientific evidence of bovine pericardium as bacteriostatic and bacteriocidal is scanty, it has been used to repair arteriotomy in the presence of infected field.[11-14,21,25-27,74,75] Prosthetic patch infection after carotid endarterectomy has been estimated to be around 0.4%.26,75 Investigators have demonstrated similar risk of postoperative infection comparing bovine pericardium, autologous vein patches, and synthetic patches.[6,11,12,74,75] However, until an underlying mechanism of resistance to infection e.g. contact cytotoxicity is demonstrated, one cannot convincingly state that bovine pericardium is immune from becoming infected. The fundamental strength of glutaraldehyde fixed bovine pericardial patch may be responsible for low rate of degeneration and resistance to infection.
Fibrosis of patches is unusual and reports of bovine pericardium patch fibrosis are distinctly rare.[77,78]. It is likely that the mechanisms that induce patch calcification may be similar to those that induce patch fibrosis, although with subtle differences. Further research may help identify fibrocyte-specific signaling pathways as potential therapeutic targets to prevent bovine pericardium fibrosis.[79]
Since the primary problem of xenografts is structural deterioration at long-term, mainly due to calcification, several improvments in the processing of xenografts and placement of the pericardial patches have been implemented to prevent structural deterioration and dystrophic calcification.[8,9,46,80-83]
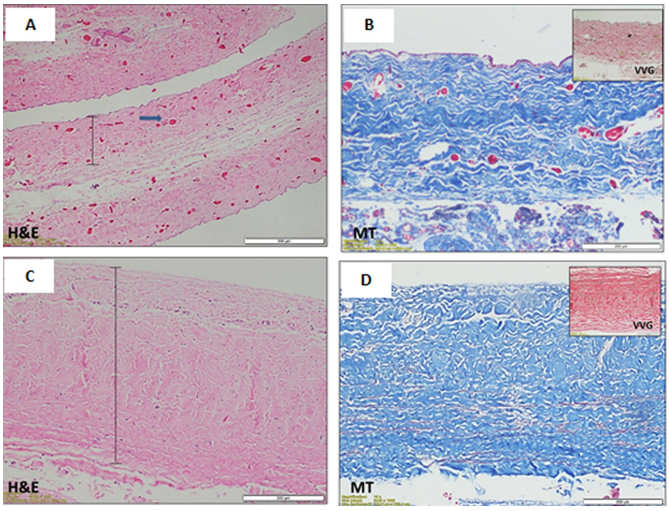
The native structure of bovine pericardium has three layers: i) the thin inner serosal layer consisting of mesothelial cells; ii) the thicker fibrosal layer formed by diversely oriented, wavy bundles of collagen and elastin; and iii) the outer epipericardial connective tissue layer that is partly continuous with the pericardiosternal ligaments (Figure 4A-4D).
Commercially available patches are processed to be acellular, preventing transplantation of bovine proteins or DNA into the host. Gluteraldehyde is a typical processing agent, crosslinking −NH2 groups of lysine, hydroxylysine, or the N-terminus of amino acids, to form amine linkages with the elimination of water; these amine linkages form covalent bonds between adjacent proteins that are stable at physiological temperature and pH. The resultant cross-linkage of xenograft tissue with glutaraldehyde increases tissue strength to inhibit biodegradation, stabilizes collagen, and reduces antigenicity.[1,57,66,67,80-92]
However, glutaraldehyde fixation promotes dystrophic calcification because of the chemical process between free aldehyde groups, phospholipids, and residual antigenicity of the bioprosthetic tissue.[1,80-85] Series of experimentation over several years through basic research have been directed toward developing a tissue treatment process to prevent calcification in glutaraldehyde fixed xenograft tissue. The aim of the anticalcification strategies is to extract lipid or to neutralize toxic residual aldehyde.[92-95]
Residual free aldehyde groups or polymerized forms of glutaraldehyde create a locally cytotoxic environment and result in tissue calcification. Amino acid post fixation improves protein cross-linking to increase the mechanical performance of bioprostheses or to neutralize these free aldehyde groups because the amino groups of these compounds can react with the free aldehyde groups of glutaraldehyde, forming Schiff base.[86,87,94,95] In 2009, Zhou et al demonstrated utiliy of sodium bisulfite, a classic reductive agent which reacts with aldehyde to form -hydroxyl sodium sulfonate, and would react with any free glutaraldehyde in fixed pericardial tissue, thus minimizing in vivo calcification.[96]
Short-chain alcohols, such as octanol at high concentration (>50% in aquous buffers) reduce calcification potential of aldehyde-fixed tissues by removing phospholipids or conformational changes in collagen.[87,92,93] The alcohols may also be preferentially bound to hydrophobic residues within collagen and elastin which may undergo independent calcification.[88,97]
Long-chain alcohols such as oetanol 1, 2-octanediol along with short-chains, and isopropanalol have been used along with a buffered ethanol solution to remove phospholipids more efficiently.[90,92,93,98]
The key common feature for the pathophysiology of calcification is involvement of devitalized cells and cellular debris.[80-83] There is a debate in the literature as to whether there is an immune response to bioprosthetic tissue.[80-83] Recently, it has been found that the mammal cell surface xenoantigen called -Gal epitopes are still present on the commercially available glutaraldehyde fixed tissues.[84] Patients undergoing bioprosthetic valve implantation have exhibited a significant rise in anti--Gal antibodies.[99-104] Decellularization suppresses the rise anti--Gal antibodies titre. However, the pathogenesis of dystrophic pericardial calcification remains conjectural.
Other investigators have introduced genipin, derived from the fruits of Gardenia Jasminoides as a novel cross-linking agent because this naturally occurring cross-linker is less cytotoxic and better in vivo biocompatible than glutaraldehyde.[66,67,89] Park and associates have used recombinant human alpha galactosidase A to remove alpha-gal epitopes from porcine aortic valve.[105-107]
Despite good results of bovine pericardium in several clinical trials, degeneration of biological tissue including calcification is frequently observed.[80-83] Piers and colleagues suggested a possible correlation between calcification and contact of the rough face of the pericardium with the blood stream.[8,9] In 2011, Saporito and colleagues demonstrated experimentally that the bovine pericardium preserved in glutaraldehyde did not show alterations in its structure when implanted with different faces turned to the inner portion of vessels.[46] There was aneurysmal dilation of the implant site when the smooth face was turned to the intraluminal side. When the rough face was turned intraluminally, there was formation of a covering layer with more plasticity, modeling elastic tendon and bone formation which produced greater tension resistance, preventing its expansion. Piers and colleagues demonstrated the formation of internal apposition fibrosis on the surface of the retail. The wrinkled surface of the retail facilitates capture and adhesion of blood components and subsequent assemblage by the release of platelet factors and secondary released thromboplastin.[8,9,108] In this study, all patients underwent reconstruction of the pericardial cavity using bovine pericardium with the rough surface facing the cardiac chambers, and great vessels.
Some investigators have reported that if smooth muscle cells and/or fibroblasts migrate into the bovine pericardium patch, the patch may provide an environment that promotes subsequent calcification and degradation.[94,95] Hruska and associates summarized the currently accepted major theories regarding the mechanism and regulation of vascular calcification: i) abnormal calcium and phosphate homeostasis, ii) failure of anticalcific mediators, iii) induction of osteochondrogenesis, iv) apoptosis, v) circulating nucleatic complexes/paracrine factors derived from bone, and vi) matrix degradation.[109-113]
As these etiologies become more understood, it is possible that preventive strategies may be able to be incorporated into future generations of patches, i.e. incorporation of anticalcific mediators, remesothelialization on the surfaces of the implanted patch. [97,98,101-104,109-113,119,120] These next generation patches might be particularly useful for patients with chronic kidney disease, type 2 diabetes mellitus, and elderly, who might be at increased risk of patch calcification and degradation.[114]
When bovine pericardium is used as a vascular patch, the collagen surface of the bovine pericardial patch may be a nidus of thrombus formation. However, thrombosis of bovine pericardium patches has not been reported to be a major problem, either acutely or chronically. In clinical practice, most institutions routinely administer Dextran-40 for 24 hours post endarterectomy to prevent thrombus formation and propogation at the site of thromboendarterectomy.
Exploring the unknown: Future Directions
This communication is not meant in any way to convince those surgeons satisfied with their own methods of performing a Bentall’s procedure. Rather it hopes to pointout that reconstructed pericardial cavity is beneficial preventing inoculation with infected mediastinal wound, minimizes diffuse oozing, and avoids postsurgical periconduit adhesions.
Can intimal hyperplasia be avoided by seeding mesenchymal stromal cells on bovine pericardium? Investigators have used bovine pericardium as the scaffold for the seeded multilayered mesenchymal stromal cells to provide a base for uniform cardiac tissue regeneration.115 They have demonstrated that this novel bioengineered tissue graft can serve as a useful cardiac patch to restore the dilated ventricle and stabilize cardiac functions after myocardial infarction.115 Interestingly, the authors reported increased density of neomicrovessels in the tissue engineered patches compared to control patches, suggesting that tissue regeneration occurs within the porous bovine pericardium through a process involving cell recruitment and tissue-specific differentiation.
Investigators have demonstrated that acellular bovine pericardial tissues fixed with genipin could provide a natural microenvironment for host cell migration, and may be used as a tissue engineering extracellular matrix to accelerate tissue regeneration.115 In an attempt to reduce postsurgical pericardial adhesions, researchers are experimenting on mesothelial regeneration on acellular bovine pericardia loaded with an angiogenic agent (ginsenoside Rg1).[66,67,105-107,115-120] This exciting research shows the prospect for delivering cell therapy, in a site-specific manner, with bovine pericardial patches.
Conclusions
Reconstruction of the pericardial cavity using bovine pericardial patch minimizes diffuse oozing of blood, mediastinal infection, and is not associated with late development of pericardial constriction and calcification. Understanding the mechanisms by which bovine pericardium heals after patch angioplasty may lead to next generation tissue engineered patches. Process of decellularization, use of alcohol, newer preservatives like genipin and mechanism of healing of bovine pericardial patches may improve the long-term durability of bovine pericardial patch.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
