
Case Report | DOI: https://doi.org/10.31579/2690-4861/014.
1 Internal Medicine, Memorial Healthcare, Sunrise, USA.
2 Internal Medicine, Memorial Hospital West Healthcare System, Pembroke Pines, USA.
3 Cardiology, Memorial Hospital West Healthcare System, Pembroke Pines, USA.
4 Malignant Hematology & Cellular Therapy, Moffitt Cancer Center at Memorial Healthcare System, Pembroke Pines, USA.
*Corresponding Author: Rosas D MD, 1Internal Medicine, Memorial Healthcare, Sunrise, USA.
Citation: Rosas D, Yepes I, Tschanz J, Wariboko M, Sandoval-Sus J. (2020) EBV: From Kissing Disease to Broken Heart. International Journal of Clinical Case Reports and Reviews. 2(3); DOI:10.31579/2690-4861/014
Copyright: ©2020 Daniel Rosas, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 February 2020 | Accepted: 29 May 2020 | Published: 05 June 2020
Keywords: NHL;BL; kissing disease; pulmonary embolism
The prevalence of non-Hodgkin lymphomas (NHL) involving the heart ranges between 9-24% [1]. and very rarely cases of primary cardiac Burkitt Lymphoma (BL) have been reported.
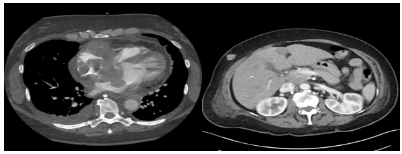
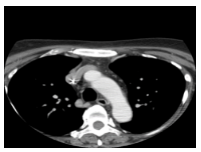
We present a case of a 59 year old female patient that presented with exertional chest pain and palpitations. On admission she was noticed to be tachycardic. An EKG showed right axis deviation with signs of right ventricular hypertrophy. Pro-BNP came out 665 pg/ml and 3 sets of troponin levels were negative. A CT scan of the chest was negative for pulmonary embolism (PE) but revealed a nodular thickening of the atrial septum with right atrial extension encasing the right coronary artery. A CT scan of the abdomen and pelvis with IV contrast (figure 1) revealed several nodular foci scattered in the subcutaneous fat of the abdominal wall bilaterally including a 2.0 x 1.4 cm nodular focus involving the anterolateral right abdominal wall. An initial transthoracic echocardiogram (TTE) (figure 2) revealed thickening of the interatrial septum with a 3.6 cm x 2.6 cm mass protruding from the interatrial septum into the left atrium and a 3.1cm x 5.3 cm pedunculated mass protruding from the interatrial septum into the right atrium with significant obstruction within the right atrium identified by color flow Doppler.
The prevalence of non-Hodgkin lymphomas (NHL) involving the heart ranges between 9-24% [1]. and very rarely cases of primary cardiac Burkitt Lymphoma (BL) have been reported.
We present a case of a 59 year old female patient that presented with exertional chest pain and palpitations. On admission she was noticed to be tachycardic. An EKG showed right axis deviation with signs of right ventricular hypertrophy. Pro-BNP came out 665 pg/ml and 3 sets of troponin levels were negative. A CT scan of the chest was negative for pulmonary embolism (PE) but revealed a nodular thickening of the atrial septum with right atrial extension encasing the right coronary artery. A CT scan of the abdomen and pelvis with IV contrast (figure 1) revealed several nodular foci scattered in the subcutaneous fat of the abdominal wall bilaterally including a 2.0 x 1.4 cm nodular focus involving the anterolateral right abdominal wall. An initial transthoracic echocardiogram (TTE) (figure 2) revealed thickening of the interatrial septum with a 3.6 cm x 2.6 cm mass protruding from the interatrial septum into the left atrium and a 3.1cm x 5.3 cm pedunculated mass protruding from the interatrial septum into the right atrium with significant obstruction within the right atrium identified by color flow Doppler.

An ultrasound-guided biopsy of the soft tissue nodule in the right anterior abdominal wall and subcutaneous tissue was obtained. Histologic sections revealed a dense atypical lymphoid infiltrate mainly consisting of intermediate sized lymphocytes with high nuclear to cytoplasmic ratio with one to several small nucleoli with frequent apoptotic bodies imparting a starry sky appearance (figure 3)

Immunohistochemical stains and immunofluorescence in situ hybridization studies (FISH) confirmed a diagnosis of Burkitt lymphoma. The patient received 4 cycles of DA EPOCH-R and follow up CT of the abdomen and pelvis (figure 4) reported resolution of the soft tissue density involving the partially visualized portions of the heart, pericardium and abdominal wall as well as smaller atrial septal nodularity seen on follow up TTE.
Although rare, cardiac lymphomas should be considered in the differential diagnosis of patients with identified cardiac masses. As the initial presentation is usually composed by non-specific symptoms, a detailed clinical history can identify certain constitutional symptoms and a thorough physical exam can lead to the suspicion of cardiac structural pathology prompting the need for the appropriate chest imaging. Most of the cardiac masses are incidentally identified in imaging studies. Further characterization may need TTE or TEE which are more sensitive and specific due to the tridimensional and temporal quality of the imaging. Appropriate biopsy with pathology and molecular studies are of utmost importance in making an accurate diagnosis in order to select the best management for this highly aggressive malignancy.
Background:
The prevalence of non-Hodgkin lymphomas (NHL) involving the heart ranges between 9-24% [1]. Among these, diffuse large B cell lymphoma (DLBCL) is the most common and only in extremely rare cases Burkitt Lymphoma (BL) has been reported. BL by itself represents just 1% of all non-Hodgkin lymphomas (NHL) and has a prevalence in the general population of 0.30 per 100,000 people [2]. In patients with Human Immunodeficiency virus (HIV) this percentage can reach almost 30% [3, 4]. In the current literature most of the reported cases of lymphoma involving the heart presented in immunocompromised patients with HIV. We report a case in a middle age woman without a diagnosis of HIV and otherwise immunocompetent.
Case Report:
A 59 year old hispanic patient presented with palpitations and pressure like retrosternal chest pain which was more pronounced with exertion, lying flat and while coughing. She also mentioned that she had some bilateral calf pain and dry cough for the last 3 weeks. She was admitted to the hospital 2 years ago with similar symptoms and was found to have paroxysmal tachycardia. Physical examination was remarkable for tachycardia and both heart sounds and pulse were markedly irregular. She had mild wheezing as well. Laboratory work-up was negative for HIV, Pro-BNP was 665 pg/ml, three sets of troponin were negative and she had mild normocytic normochromic anemia. EKG on admission showed sinus tachycardia with right axis deviation and signs of right ventricular hypertrophy.
A computed tomography (CT) of the chest was ordered to rule out pulmonary embolism and revealed a nodular thickening of the interatrial septum extending to the right and left atria as well as a nodular soft tissue density encasing the right coronary artery (RCA) and a small pericardial effusion. Mediastinal, internal mammary and right hilar lymphadenopathy were also noticed (Figure 1A). A CT scan of the abdomen and pelvis with IV contrast revealed several nodular foci scattered in the subcutaneous fat of the abdominal wall bilaterally including a 2.0 x 1.4 cm nodular focus involving the anterolateral right abdominal wall (Figure 1B). An initial transthoracic echocardiogram (TTE) revealed thickening of the interatrial septum with a 3.6 cm x 2.6 cm mass protruding from the interatrial septum into the left atrium and a 3.1cm x 5.3 cm pedunculated mass protruding from the interatrial septum into the right atrium with significant obstruction within the right atrium identified by color flow Doppler. The left ventricle (LV) function was hyperdynamic and no valvular abnormalities were found.
Initially a myocardial biopsy was intended but due to safety concerns it was deferred and an ultrasound-guided biopsy of the soft tissue nodule in the right anterior abdominal wall and subcutaneous tissue was obtained. Histologic sections revealed a dense atypical lymphoid infiltrate mainly consisting of intermediate sized lymphocytes with high nuclear to cytoplasmic ratio with one to several small nucleoli with frequent apoptotic bodies imparting a starry sky appearance to the lymphoid infiltrate and mitotic figures. On Immunohistochemical stains and immunofluorescence in situ hybridization studies (FISH), the neoplastic lymphoid cells were positive for CD45, CD20, PAX5, CD10, BCL6, CD43, and EBER, predominantly positive for c-MYC, and were negative for BCL2, MUM1, CD5, TdT, CD34, cyclin D1, CD30, and HHV8. The Ki-67 proliferation fraction was 100%. CD3 and CD5 highlight scattered T cells. CD21 did not show any follicular dendritic cell meshworks. Few scattered CD138+, MUM1+ plasma cells appeared to show a mixture of kappa and lambda positive cells by in situ hybridization. The FISH analysis of the specimen from part B (F19-785) revealed a kappa clonal B-cell population with co-expression of CD10.
A diagnosis of high risk Burkitt's lymphoma stage IV (extra nodal involvement). Testing for EBV DNA was positive with qualitative analysis revealing 165,163 copies/mL. The patient was transferred to our Hematology-Oncology unit for initiation of chemotherapy due to the aggressive nature of the lymphoma. The patient was started on chemotherapy regimen of DA EPOCH-R(Etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab). The patient was discharged 3 weeks later and a new TTE reported smaller size of the nodular masses involving the interatrial septum in the left atrium. He patient received 4 cycles of DA EPOCH-R and follow up CT of the abdomen and pelvis performed reported resolution of the soft tissue density involving the partially visualized portions of the heart, pericardium and abdominal wall.
Discussion
Burkitt lymphomas encompass only 1% of all the non-Hodgkin lymphomas and by themselves NHL involving the heart are rare with a maximal prevalence reaching 24%. Among patients presenting with NHL involving the heart, DLBCL is the most common. Very rarely there have been other cases of primary cardiac Burkitt lymphoma reported in the literature with a review of the literature reporting only 13 manuscripts [1,3]. Most of the cases presenting with primary cardiac lymphoma (PCL) were patients with a diagnosis of HIV with the immunocompromised state making them more susceptible to this aggressive malignancy. In our patient, a diagnosis of HIV was excluded on admission. Burkitt lymphomas have a mutation in the MYC gene. This mutation is associated with EBV activation of B-cells. EBV infection is found in 5-10% of sporadic Burkitt lymphoma and 30% of HIV associated Burkitt lymphoma [8].
Although a typical presentation of Burkitt lymphoma comes with abdominal pain and constitutional symptoms, a patient presenting with initial cardiac signs and symptoms like chest pain, orthopnea or signs of heart failure may warrant chest imaging and echocardiography. Most of the cases of cardiac lymphomas are found incidentally during imaging studies performed to rule out another differential diagnosis. In this case, a chest CT was performed to rule out a pulmonary embolism. Incidental cardiac masses are often benign in nature with most cases being a thrombus or vegetation. Even when malignancy is indeed suggested by imaging, cardiac metastasis from a known breast, lung or malignant melanoma are more common than primary cardiac tumors. From those being primary cardiac tumors, 90% are benign with atrial myxomas making up 50% of the cases and papillary fibroelastomas are the second most common. Primary malignant cardiac tumors are even more infrequent and represent only 25% of all primary cardiac tumors. Most of those being sarcomas [5,6]. With that being said, finding a primary cardiac Burkitt lymphoma is case reportable. Onyee Chan, et al did a review of the literature and found only 22 cases reported in the English literature including their case. Only 7 of these were in patients with confirmed negative HIV status [1].
Mortality is high as reported back in 2008 by Onyee, et al. In their review of the literature almost 50% of the 22 cases and with the longest surviving patient reported to be alive at 36 months after the diagnosis [1]. With new chemotherapy regimens, better imaging modalities, and multidisciplinary management of these patients, early diagnosis and more effective treatment prevent these patients from getting locally advanced cardiac involvement. This includes its inherent mechanical complications due to right heart involvement.
Petrich A, et al, found that immune status, left ventricular involvement, the presence of extra-cardiac disease and arrhythmia were 4 factors that markedly impact survival [5]. This may correlate with how locally advanced is the cardiac involvement from the lymphoma.
The correct pathologic diagnosis is essential in order to select the appropriate systemic chemotherapy regimen which as per the available literature is the only effective therapy for this kind of malignancy [7]. In our case we able to avoid endomyocarial biopsy as there was a more suitable abdominal wall lesion that confirmed diagnosis. There are potential serious complications of systemic chemotherapy on the heart, including cardiac toxicity and the mechanical complications due to regression of the lesions and alteration of the surrounding cardiac structures. All these can end in cardiac free wall rupture, atrial septal defect (ASD), ventricular septal defect (VSD) or valvular apparatus alterations with ensuing valvular insufficiency. Follow up imaging with TTE or TEE allows identification of these potential complications as well as assess for response to chemotherapy. In our case this follow up imaging found complete resolution of the interatrial septal nodular masses. The interdisciplinary approach with management and follow up by Hematology-Oncology in conjunction with Cardiology allows for better outcomes in the management of this aggressive and rare subset of lymphoma.
Conclusion
Although rare, cardiac lymphomas should be considered in the differential diagnosis of patients with identified cardiac masses. Although the initial presentation is usually composed by random symptoms, a detailed clinical history can identify certain constitutional symptoms and a thorough physical exam can lead to the suspicion of cardiac structural pathology. These might lead to findings prompting the need for the appropriate chest imaging. Most of the cardiac masses are incidentally identified in imaging studies. Further characterization may need TTE or TEE which are more sensitive and specific due to the tridimensional and temporal quality of the imaging. Appropriate biopsy with pathology and molecular studies are of utmost importance in making an accurate diagnosis in order to select the best management for this highly aggressive malignancy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
