
Research Article | DOI: https://doi.org/10.31579/2578-8965/149
1 Ministry of National Guard-Health Affairs, Jeddah, Saudi Arabia.
2 King Saud Bin Abdul-Aziz University for Health Sciences, Jeddah, Saudi Arabia.
*Corresponding Author: R Wali, King Saud Bin Abdul-Aziz University for Health Sciences, Jeddah, Saudi Arabia.
Citation: Wali R., Jaha A., Jamaluddin H., Shakir M., Alhumaidah R., et al, (2023), Eating Disorders Among Primary Health Care Attendees in Jeddah city, Epidemiology and Risk Factors. Saudi Arabia. J. Obstetrics Gynecology and Reproductive Sciences, 7(1) DOI: 10.31579/2578-8965/149
Copyright: © 2023 R Wali, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 January 2023 | Accepted: 13 January 2023 | Published: 25 January 2023
Keywords: eating disorder; anorexia nervosa; bulimia nervosa; primary health care; saudi arabia
Introduction: An eating disorder refers to states in which food and nourishment have a manipulative role in regulating the body's appearance. The most common forms are anorexia nervosa, bulimia nervosa, and eating disorders not otherwise specified (ED-NOS). This study aimed to estimate the prevalence and identify risk factors associated with eating disorders among Saudi attendees of PHCCs in Jeddah city during 2006.
Objectives of the research: To estimate the prevalence of eating disorders among Saudi attendees of PHCCs in Jeddah and to identify risk factors associated with eating disorders in Jeddah city.
Methodology: This was a cross-sectional analytic study among PHC attendees of the Ministry of Health in Jeddah city starting from August 2006 up to January 2007. It included Saudi males and females aged 15-45 attending the selected centers. A sample size of at least 267 individuals was estimated. Multi-stage sampling was used to ensure representativeness. (Sick, Control, One, Fat, Food) (SCOFF), and eating disorder screen for primary care questionnaires (ESP) were the tools used for data collection.
Results: The prevalence of eating disorders among the study population was 13.7Percentage using ESP and 8.9Percentage using the SCOFF questionnaire. The prevalence of eating disorders using the ESP questionnaire was 7.6Percentage among men and 19.5Percentage among women. While using the SCOFF questionnaire, the prevalence was 6.1Percentage among men and 11.6Percentage among women. There was a significant association between eating disorders and a history of abuse, eating alone, and considering oneself thin (P- value= 0.001, 0.00, and 0.008, respectively).
Conclusion: The prevalence of eating disorders in Jeddah is comparable to prevalence rates reported by studies in western societies and somewhat higher than what has been reported in the region.
MOH: Ministry of Health
PHCCs: Primary Health Care Centers
AN: Anorexia Nervosa
RAN: Restricting Anorexia Nervosa
BN: Bulimia Nervosa
ED-NOS: Eating disorder not otherwise Specified
ED: Eating disorder
An eating disorder is a state that can be used to regulate the body's appearance by manipulating food and nourishment. The most common forms of eating disorders are Anorexia nervosa (AN) and Bulimia nervosa (BN) [1].
There are variants of eating disorders that do not meet the diagnostic criteria for AN or BN. Those are still eating disorders that require necessary treatment. Individuals with Eating Disorder (ED) behaviors that resemble AN or BN but whose eating behaviors do not meet one or more essential diagnostics criteria can be diagnosed as eating disorders not otherwise specified (ED-NOS) [2].
Body weight, Shape concerns, and dieting and exercise disorders represent common sources of distress in females, with subclinical disorders affecting 10Percentage-20Percentage of women and eating disorders affecting up to 5Percentage. ED-NOS occurs in approximately 3 to 5 percent of women between the ages of 15 and 30 in western countries [3].
The lifetime prevalence of AN in women in western countries is estimated to be 0.3 to 1Percentage; rates for men tend to be only 10 percent of those for women. [3] An estimated 1 to 2 million women in the United States meet the criteria for BN as defined in the DSM-1V, whereas 50,000 women meet the diagnostic criteria for Anorexia nervosa [3].
Significant medical problems, such as the potential for significant growth retardation, pubertal delay or interruption, and peak bone mass reduction, are all associated with Anorexia nervosa. Suicide has been reported in up to 5Percentage of patients with chronic anorexia nervosa [4].
Moreover, cultural effects on eating attitudes were studied in an Israeli sub-population. Eating attitudes and body image were assessed using the eating attitudes test EAT-26. They hypothesized that the attitudes of those adolescent females most exposed to western body-shape ideas and simultaneously experiencing a conflict between traditional and modern images of the female role would resemble anorectics [5].
More males sought treatment for eating disorders in the 1990s than in the1980s. It is unclear whether this reflects prevalence or that males seek treatment more often. The psychological features of males with eating disorders appear like females when looking at co-morbid psychopathology, behaviors, and attitudes typical of patients with eating disorders. One study in the United States showed that male and female ED patients have similar family histories of relatives with eatingdisorders [3].
One study in Singapore used the Eating Attitude Test (EAT) to assess the prevalence of young females at risk of developing eating disorders (ED) and the associated sociodemographic variables. They concluded that 7.4 percent of females are at risk of developing ED. [6] AN is an important health problem to address. It has been linked to severe long-term morbidity and substantial mortality, with 10Percentage of cases ending in death and impairing normal bodily functioning in individuals [7].
Studies showed that the majority of anorexics are women who are Caucasian and from higher socioeconomic backgrounds. These demographic trends may shift towards including more ethnic minorities and people from lower social classes. [8] According to some epidemiological studies of both short and long-term treatment for anorexia and bulimia, AN and other eating disorders are reaching epidemic proportions in adolescent populations [9].
Another study regarding Disordered eating attitudes among adolescent girls in the United Arab Emirates used the eating attitude test-40. It showed that a High EAT score was associated with age, BMI, internalization of the thin ideal, drive for thinness, knowing someone on a weight loss strategy, having a family member with a weight-related or mental health problem, and watching western TV programs [10].
One study in Spain reported that solitary eating, parental marital status other than married, and a higher level of radio use were independent risk factors for developing an ED. Increased use of both mass media (listening to the radio for Greater than1 h/d and reading one girls' magazine per week) was associated with a higher risk of developing an ED [11].
A study in Riyadh showed that body mass index, speaking a western language, and having lived in a western country were the most significant personal factors associated with dieting behavior. Small family sizes, higher parental education, and better occupation were significant family factors related to dieting [12]. Moreover, obesity, dieting, and social pressure are considered risk factors for developing eating disorders in adolescent girls [13].
This is a cross-sectional analytic study among PHCC attendees of the Ministry of Health (MOH) in Jeddah city for six months, from August 2006 to January 2007.
The study included Saudi males and females aged (15-45) attending the selected PHCCs during the study period. Exclusion criteria were those aged below 15 and above 45 and patients with chronic diseases, such as malignancy or Crohn's disease, which lead to a BMI of <17>
The sample size was calculated according to the pilot study using Epi-info software statistical package 2000. A sample size of at least 267 individuals was estimated, and multi-stage sampling was used to ensure representativeness.
Sick Control, One, Fat, Food (SCOFF), and ED screen for primary care (ESP) questionnaires were the tools used for data collection. SCOFF questionnaire is a 5-question Yes or No questionnaire used for screening eating disorders. A "Yes" answer for the first question was regarded as positive, while the "No" answer was taken as positive for the remaining four. ESP is another screening test for eating disorders. It is also a Yes or No questionnaire, where each "Yes" answer was taken as positive.
If the participant scores Greater than2 in any of the screening tests (SCOFF or ESP), a full ED diagnostic interview (DSM-IV) was arranged. The DSM-IV diagnostic criteria questionnaire for AN and Bulimia nervosa: each consists of four questions. A "Yes" answer to all the criteria will diagnose AN and BN, respectively.
In the SCOFF questionnaire, a cutoff of 2 or more positive responses resulted in a sensitivity of 78Percentage (95Percentage CI, 62Percentage to 93Percentage) and a specificity of 88Percentage (95Percentage CI, 84Percentage to 93Percentage). The positive likelihood ratio was 6.6 (95Percentage CI, 4.3 to 10), and the negative likelihood ratio was 0.25 (95Percentage CI, 0.12 to 0.51).
As for the ESP questionnaire, a cutoff of 2 or more positive responses yielded a sensitivity of 100Percentage (95Percentage CI, 90Percentage to 100Percentage) and a specificity of 71Percentage (95Percentage CI, 64Percentage to 77Percentage). The positive likelihood ratio was 3.4 (95Percentage CI, 2.8 to 4.2), and the negative likelihood ratio was 0.0 (95Percentage CI, 0.0 to 0.15) [14].
The collected data were entered into a personal computer and analyzed by SPSS version 10. Continuous variables were presented as mean and standard deviation, and categorical variables as frequency and percentage. Independent t-test, chi-square test, analysis of variance (ANOVA), and multiple logistic regressions were used as indicated. A P-value of < 0>
Descriptive Data
A total of 269 participants completed the questionnaires, with a response rate of 100Percentage.
Sociodemographic Variables
Table 1 demonstrates the sociodemographic variables of the study participants. All participants were Saudi (100Percentage, n=269). While men constituted 48.69Percentage (n= 131) of respondents, women accounted for 51.3Percentage (n=138). The age distribution of the sample was between (15-45) for both genders, as indicated by the study inclusion criteria, with a mean age of (28.22 SD 9.94) for men and (29.62 SD 7.99) for women. In addition, most women were married (74.6Percentage, n= 103), while only approximately half men were married (55Percentage, n=72). Moreover, most men and women held a high school degree or a higher degree (71Percentage, n=93) and (63.8Percentage, n=88), respectively.
| Table 1. Sociodemographic Variables | ||
| Characteristics | Men (n=131) No. % | Women (n=138) No. % |
Single Marital Status Married | 59 45
72 55 | 35 25.4
103 74.6 |
< high school Level of education > high school | 38 29
93 71 | 50 36.2
88 63.8 |
Died Parental Status Single Married | 10 7.6 24 18.3 97 74 | 9 6.52 49 35.5 80 57.9 |
Table 1: Sociodemographic Variables.
As for the BMI distribution, the mean BMI was (26.4 SD of 6.73) for men and (26.3 SD of 6.71) for women, as indicated in Table 2.

Table 2: BMI Distribution Among Study Population
Behavioral Characteristics
Table 3 lists the behavioral characteristics of the studied population. While 62.6Percentage (n=82) of men were using the Internet, only 34.1Percentage (n=47) of women were. In addition, only 23.7Percentage (n=31) of men read model magazines, while 41.3Percentage (n=57) of women read the magazines. Only a minority of participants, 7.6Percentage (n=10) for men and 7.2Percentage (n=10) for women, reported a history of eating alone. In addition, only 26Percentage (n=34) of men and 42.8Percentage (n=59) of women thought they were thin. Nevertheless, only 32.1Percentage (n=42) of men and 15.2Percentage (n=21) of women exercised more than three times per week.
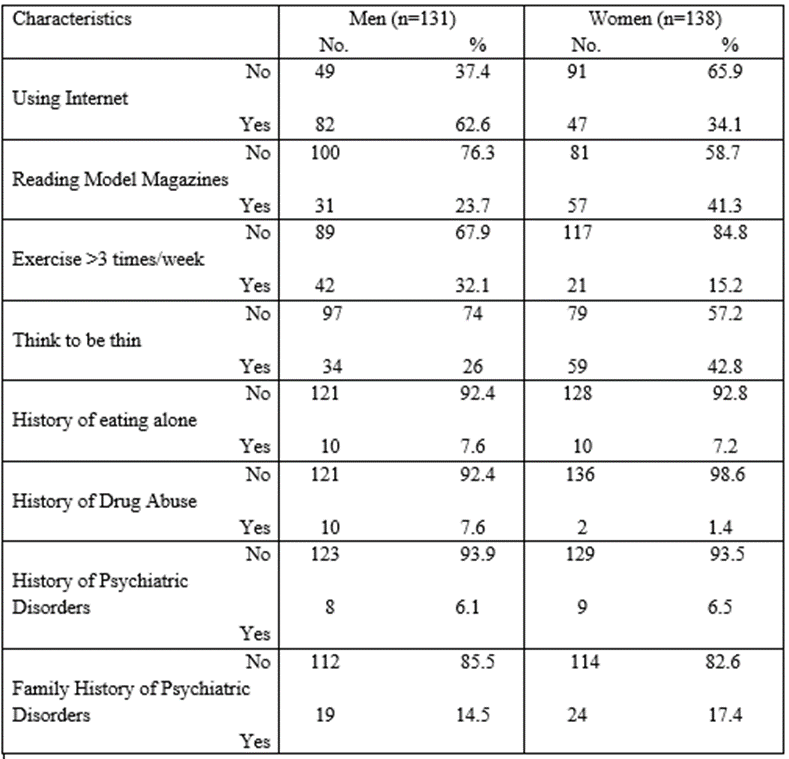
Table 3: Behavioral Characteristics
A minority of participants, 7.6Percentage (n=10) of men and 1.4Percentage (n=2) of women, reported a history of drug abuse. Additionally, 6.1Percentage (n=8) of men and 6.5Percentage (n=9) of women had a personal history of psychiatric diseases, while 14.5Percentage (n=19) of men and 17.4Percentage (n=24) had a family history of psychiatric disorders.
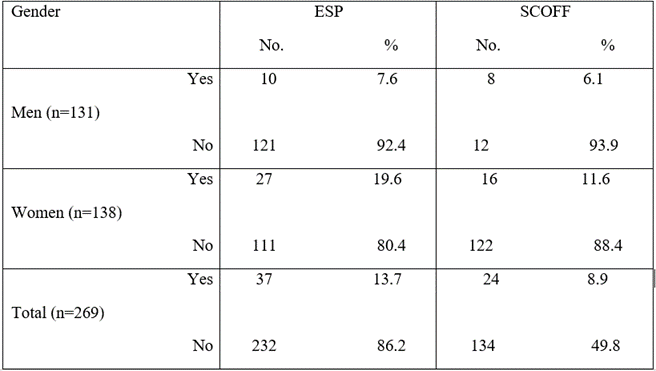
Prevalence of Eating Disorders
Table 4 shows the prevalence of eating disorders using ESP and SCOFF questionnaires. The overall prevalence of eating disorders among the participants was 13.7Percentage (n=37) using the ESP questionnaire and 8.9Percentage (n=24) using the SCOFF questionnaire. Women had a higher prevalence of eating disorders, 19.6Percentage (n=27) according to ESP and 11.6Percentage (n=16) according to SCOFF, compared to men whose prevalence of eating disorders was 7.6Percentage (n=10) according to ESP and 6.1Percentage (n=8) according to SCOFF.
Participants who scored positive on ESP and SCOFF questionnaires were introduced to the diagnostic DSM-IV criteria. This revealed that 0.4Percentage (n=1) and 1.2Percentage (n=3) of women had AN and bulimia nervosa, respectively. However, no cases of AN and BN were detected in men. Table 5 demonstrates the overall prevalence of ED not otherwise specified (ED-NOS) was 13.4Percentage (n=36). Of those, 18.8Percentage (n=26) were women. This is also demonstrated in Figure 1.
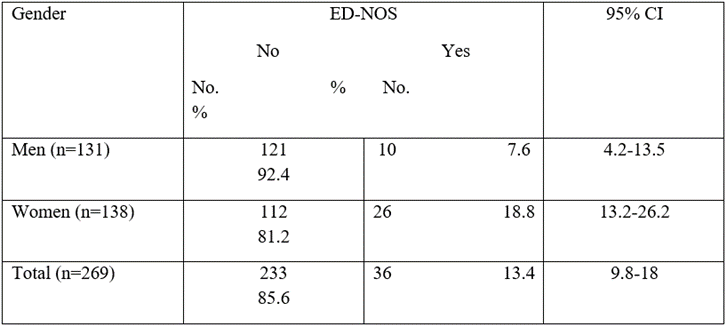
Table 5: Prevalence of Eating Disorder Not Otherwise Specified (ED-NOS)

Figure 1: Prevalence of Eating Disorder Not Otherwise Specified (ED-NOS)
Factors associated with eating disorders
Multiple logistic regression was performed to explore the association between eating disorders and other sociodemographic and behavioral characteristics. The dependent variable was eating disorders (AN, BN, and ED-NOS). The independent variables were gender, reading model magazines, family history of psychiatric disease, history of eating alone, history of abuse, and considering oneself thin. Table 6 represents the result of logistic regression, and it showed a significant association between eating disorders and a history of abuse, eating alone, and considering oneself thin (P- value= 0.001, 0.00, and 0.008, respectively).
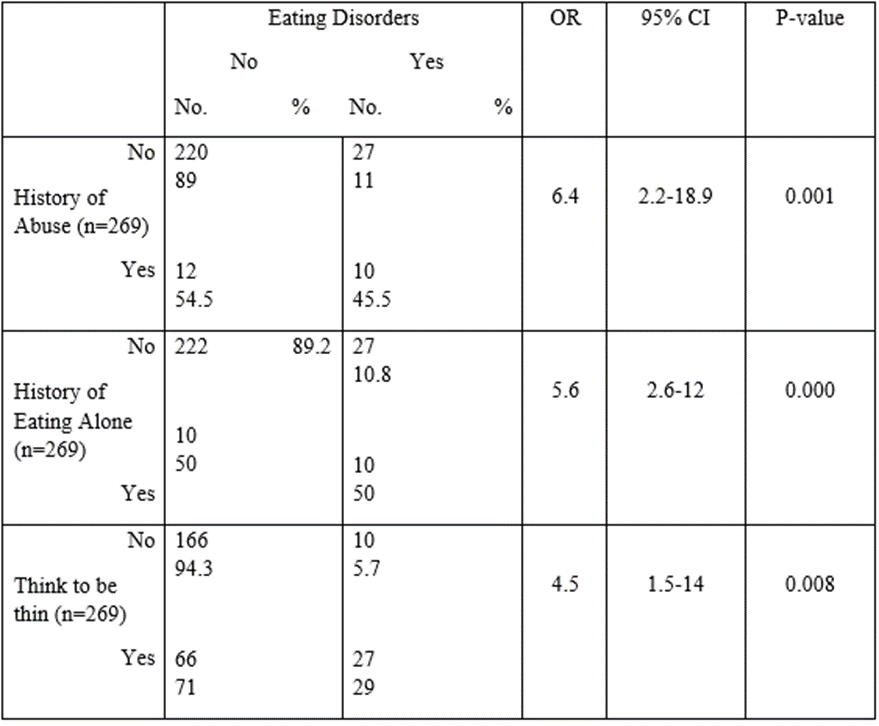
Table 6: Significant Associations with Eating Disorders
Prevalence of eating disorders
The prevalence of eating disorders was (14Percentage) compared to that reported in western literature and slightly higher than in non-western regions like Iran [15].
Gender
The prevalence of eating disorders was higher among women than men, consistent with this study's findings. This is comparable to other studies, which concluded that ED-NOS is a very common ED (12.3Percentage) and accounts for three-quarters of all community cases of eating disorders [16].
The results of this study also indicate that eating disorders are rare but not absent in Jeddah, with a higher number of ED-NOS. The high prevalence of eating disorders among women correlates with other countries. Men had lower rates of AN and BN rates, which is most likely because boys and young men tend to hide their symptoms. Therefore, they can be reluctant to ask for the help of medical professionals. In addition, this study found that an independent risk factor for developing an ED was eating alone. These results are similar to studies done in western countries [13, 17].
Among our women population, a preoccupation with having a thin body was found to be a risk factor for developing eating disorders. Several studies also suggested that having a first-degree relative with a history of drug abuse may negatively influence eating behaviors. These results were not parallel to ours since alcohol and drug abuse were not common in the study population. The latest could be due to the difficulty of admitting a history of abuse [14].
In many studies, the history of abuse of any form was related to developing an eating disorder. The results of this study resembled those among university students in Magnus. They found that sexual abuse could be considered a risk factor for the development of ED symptoms, inducing revulsion about the body in ways that may intermix with concerns about body shape, size, and weight [18].
Eating alone was found to be rare in the study population. However, it was significantly associated with the development of eating disorders in those who did. This is similar to the study done in Spain [11]. Additionally, reading model magazines more than three times per week was strongly related to eating disorders in European countries, but it was not statistically significant in our study [15].
The prevalence of eating disorders in Jeddah is comparable to prevalence rates reported by studies in western societies, and it was somewhat higher than the rates reported in other non-western cultures. Taken as a whole, this study indicates that efforts to reduce thin body preoccupation and screening for eating disorders may be necessary for reducing the prevalence in Jeddah.
From the results and conclusion gained, the following recommendations are suggested:
Further research on eating disorders in the Saudi population is needed, as this research provides a database for upcoming research in other regions. There is a need for formulating strategies to be followed by all primary care physicians to incorporate screening for behaviors of eating disorders in high-risk groups. Moreover, physicians should consider anybody with risk factors for eating disorders to be screened by SCOFF or ESP and provide health education regarding proper dieting and regular exercise programs to decrease the incidence of developing eating disorders.
The short time allocated for data collection, as well as the limited manpower were the main limitations.
Ethics approval and consent to participate:
Approval from the Joint Program of Family and Community Medicine (JPFCM) and the directorate of PHCCs in Jeddah city was obtained. (ID number 16/3239). Informed consent was obtained from all participants, and confidentiality of the data was maintained throughout the research. Those diagnosed by DSM-IV criteria were referred to King Abdul-Aziz Psychiatric Hospital for further elevation.
Guarantor: Not applicable.
Not applicable.
All data generated or analyzed during this study are included in this published article.
The author declares that they have no competing interests
This research is self-funded
Razaz Wali: intellectual idea, writing the final manuscript, and last revision.
Afnan Jaha Writing introduction, methodology, and discussion.
Huda Jamaluddin: Data collection, writing introduction, and discussion.
Murug Shakir: Writing Introduction, Methodology, Results.
Reem Alhumaidah: Data collection, Writing intro of manuscript, the conclusion of the proposal
The authors would like to acknowledge dr Rajaa Al Raddadi, consultant of community medicine, for the data analysis and Dr. Hanaa Al Hajjar, Consultant of family medicine, for the final manuscript review.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
