
Research Article | DOI: https://doi.org/10.31579/2578-8965/166
1 Yalgado Ouedraogo teaching hospital (YOTH), Ouagadougou, Burkina Faso.
2 Higher Institute of Health Sciences of Nazi Boni University, 01 BP 1091, Bobo-Dioulasso, Burkina Faso.
3 Sourô Sanou University Hospital Center, Bobo-Dioulasso, Burkina Faso.
4 Health Science Training and Research Unit of Joseph Ki-Zerbo University.
*Corresponding Author: KOMBOIGO BE, Higher Institute of Health Sciences of Nazi Boni University, 01 BP 1091, Bobo-Dioulasso, Burkina Faso.
Citation: Some Wc, Komboigo Be, Simpore A, Some Da, Thieba B, (2023) Early Post-Cesarean Rehabilitation in A Tertiary Hospital in Burkina Faso, 2021, J. Obstetrics Gynecology and Reproductive Sciences, 7(6) DOI:10.31579/2578-8965/166
Copyright: © 2023, KOMBOIGO BE. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 May 2023 | Accepted: 16 June 2023 | Published: 22 August 2023
Keywords: early; rehabilitation; caesarean section; yoth; burkina faso
Introduction: early post-caesarean rehabilitation could be an ideal alternative in terms of direct health savings for the parturient and indirect for the community.
Objective: Studying the effects of early rehabilitation after caesarean section in women at Yalgado Ouedraogo teaching hospital (YOTH)
Methodology: This was a cohort study comparing two groups of patients who underwent a scheduled caesarean section from 7th May to 4th September, 2020 in the obstetrics department of YOTH. Group 1 consisted of women benefiting from the early rehabilitation protocol (n=124) and group 2 consisted of non-rehabilitated women (n=124).
Results: The times of first getting up (p=0.01), walking (p<0.05), first drink (p=0.0001), removal of the urinary catheter (p<0.05), and urination (p<0.05) were significantly reduced in group 1. There was no statistically significant difference in postoperative pain. The mean time to first urination after removal of the urinary catheter was 18.8 ± 4.3 hours in the rehabilitated operated group versus 28 ± 10.5 hours in the non-rehabilitated group (p < 0.05). The first rise took place on average 7.2 ± 1.5 hours after the cesarean section in the rehabilitated group versus 8.1 ± 3.7 hours in the non-rehabilitated group (p=0.01). There was a significant reduction in length of stay (p < 0.05) and cost of treatment (p=0.)
Conclusion: The early rehabilitation protocol after caesarean allows a significant improvement in terms of functional recovery, length of stay and cost of treatment.
Any surgical procedure generates stress which can be responsible for profound modifications in the homeostasis of the human organism. Following this, comes convalescence, which is defined as a complex process specific to each patient [1].
The purpose of conventional perioperative care is to deal with the stress associated with the surgical act and to promote a smooth convalescence. The concept of "Fast track Surgery" or "enhanced recovery after surgery" which means "early, accelerated or improved rehabilitation" makes it possible to reduce the duration of hospitalization for patients while improving postoperative recovery, through a multidisciplinary approach. and multimodality of the perioperative period [2]. This early rehabilitation is also applicable after cesarean section. Indeed, caesarean section is increasingly considered a non-major intervention since nowadays it is possible for patients to return to normal physical activity after this intervention within a short to medium period of time [3].
The use of maternity services by women has increased significantly since the introduction of free maternal and child care by the government of Burkina Faso in 2016 [4]. This could explain the increase in the cesarean rate observed in hospitals. But the duration of hospitalization in most of these hospitals can reach three days or more. The number of hospital beds being limited in these hospitals, there is inevitably a problem of availability of beds. At the Yalgado Ouedraogo teaching hospital (YOTH), the occupancy rate of maternity beds was 120.5%, 114.2%, 116% respectively in 2016, 2017 and 2018 [5]. The overcrowding of hospital rooms leads some women to lie on the floor with negative consequences on the quality of care offered and an increase in the rate of morbidity and maternal and neonatal mortality. Early post-caesarean rehabilitation at the YOTH could therefore be an ideal alternative in terms of direct health savings for the parturient and indirect for the community. The aim of the work was to study the effects of early rehabilitation after caesarean section in women at the Yalgado Ouedraogo teaching hospital (YOTH).
The study took place in the obstetrics department of the Yalgado Ouedraogo teaching hospital (YOTH)). This was a cohort comparing two groups of patients who underwent a cesarean section between 7th May and 4th September, 2020. Group 1 had received the early postoperative rehabilitation protocol instituted during this study and group 2 the usual care protocol after caesarean section. We included in the study all the women who had undergone a planned caesarean section during which no pre- and intra-operative complication had occurred. We did not include women who underwent emergency caesarean section or those who presented a contraindication to one of the molecules of the postoperative management protocol or those who had an ASA (American Society of Anesthesiologists) score higher than 2. We carried out an exhaustive sampling of all the women admitted for scheduled caesarean section and who met the study criteria. The choice of patients from the two groups was made randomly without a matching criterion. We collected 248 patients including 124 from group 1 and 124 from group 2. The data were collected by semi-structured direct individual interviews and by a documentary review using a questionnaire including the variables of the study. The judgment criteria related to the postoperative length of stay, functional recovery (motor, sensory and cognitive), the occurrence of postoperative adverse effects, the overall cost of treatment and the management of postoperative pain operative. The data were collected by direct semi-structured individual interviews and by a documentary review using a questionnaire including the variables of the study. The judgment criteria related to the postoperative length of stay, functional recovery (motor, sensory and cognitive), the occurrence of postoperative adverse effects, the overall cost of treatment and the management of postoperative pain operative. The data were collected by direct semi-structured individual interviews and by a documentary review using a questionnaire including the variables of the study. The judgment criteria related to the postoperative length of stay, functional recovery (motor, sensory and cognitive), the occurrence of postoperative adverse effects, the overall cost of treatment and the management of postoperative pain operative.

Box 1: Joint care administered to the two study

Box 2: Usual post-operative care administered to group 2 (usual department protocol)

Box 3: Application of early postoperative rehabilitation to group 1
Microsoft Word and Excel 2019 computer software were used for word processing, tables, graphs and Epi info version 7.2.2 for data analysis. The central tendencies (mean) and dispersion (standard deviation, minimum, maximum, quantiles) parameters were calculated for the quantitative variables. For qualitative variables proportions were used. Tests (Chi², Fischer's and Student's exact test) were used to assess the association between the different variables at the 5% significance level. For ethical considerations, we obtained authorization from the national ethics committee in Burkina Faso under deliberation number 68 of 22th April, 2020. Also, patients were asked to give their free and informed consent to participate in the study.
Socio-demographic characteristics
The average age of the rehabilitated patients was 28.7 ± 6.7 years versus 27.6 ± 6.5 years for the non-rehabilitated patients (p= 0.15). Table 1 includes the distribution of patients according to Socio-demographic characteristics.

Table 1: Distribution of patients according to Socio-Demographic characteristics
Rehabilitation data
The average time taken to absorb the first drink was 6.9 hours ± 1.4 hours in the rehabilitated group versus 8.3 hours ± 3.7 hours in the non-rehabilitated group (p= 0.0001). The average time for removal of the urinary catheter was 7.7 ± 2.1 hours in the operated group. rehabilitated versus 10.5 hours ± 4.9 in that of the non-rehabilitated rehabilitated (p less than0.05). The mean time to ablation of the peripheral venous line was 24.3 hours ± 2.4 in the rehabilitated group versus 22.3 hours ± 5.6 in the non-rehabilitated group (p=0.0003). Table 2 includes the distribution of patients according to data from early rehabilitation.
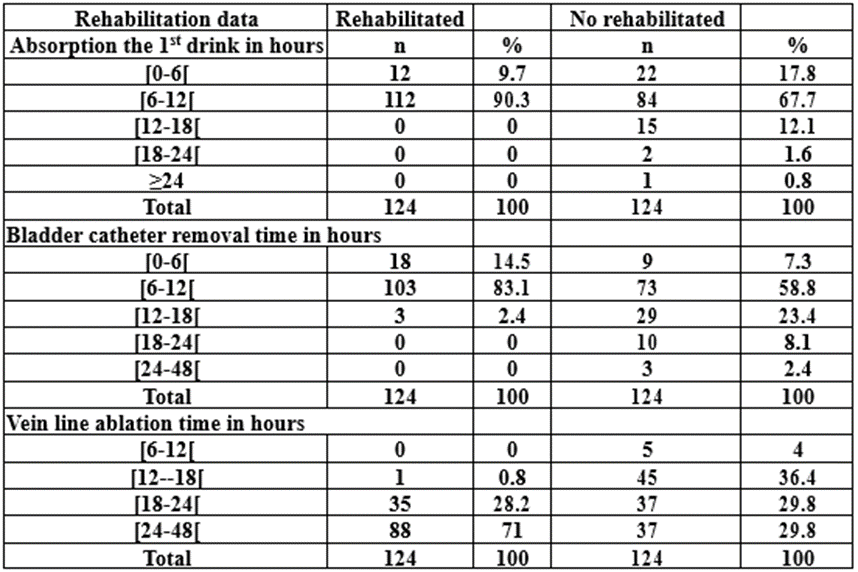
Table 2: Distribution of patients according to data on early rehabilitation
Functional recovery
The mean time to first urination after removal of the urinary catheter was 18.8 ± 4.3 hours in the rehabilitated operated group versus 28 ± 10.5 hours in the non-rehabilitated group (p less than 0.05). Figure 1 illustrates the distribution of patients according to the time to occurrence of the first spontaneous micturition after removal of the urinary catheter.

Figure 1: Distribution of rehabilitated patients (n1=124) and not rehabilitated(n2=124) according to the delay of the first micturition after removal of the urinary catheter.
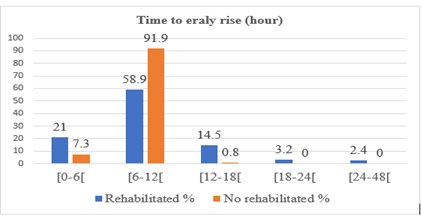
Figure 2: Distribution of rehabilitated patients (n1=124) and not rehabilitated (n2=124) according to the time to first get up after the caesarean section.
The first rise took place on average 7.2 ± 1.5 hours after the cesarean in the rehabilitated group versus 8.1 ± 3.7 hours in the non-rehabilitated group (p=0.01). Figure 2 illustrate the distribution of patients according to the time to first get up after caesarean section.
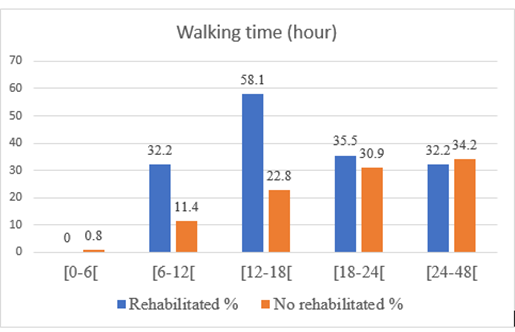
Figure 3: Distribution of rehabilitated (n=124) and non-rehabilitated (n=124) patients according to ambulation time after caesarean section.
The average time to return to walking was 16.4 ± 3.6 hours in the rehabilitated group vs.20.9 ± 8.5 hours in the non-rehabilitated group (p less than 0.05).
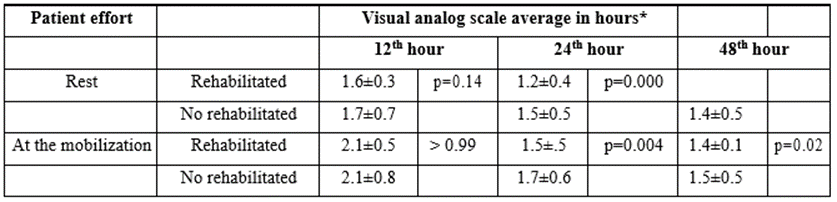
Table 3: Distribution of patients according to the mean of the visual analogue scales according to the effort of the patient at the 12th, 24th and 48th hour.
Postoperative pain
In Table 3 are presented the means of the visual analog scales at rest and during mobilization at the 12th, 24thand 48thhour.

Table 4: Distribution of rehabilitated and non-rehabilitated patients according to side effects
Scalable data
The usual protocol was significantly associated with discomfort on first rising (p less than 0.05). Table 4 presents the adverse effects occurring in the postoperative period according to the treatment groups. The average duration of hospitalization after the cesarean section was 2.9 days ± 0.2 in the rehabilitated group versus 3.5 days ± 0.9 days in the non-rehabilitated group (p less than 0.05). The average cost of care for patients in the early rehabilitation group was 89516.1 CFA money± 9699.1 vs 97612.9 CFA money ± 29070.1 in the non-rehabilitated group (i.e., respectively 179 USD±19.4 versus 195.23 USD±58.4). The difference was statistically significant with p=0.003.
Early rehabilitation data
The average time taken to absorb the first drink was 6.9 hours ± 1.4 in the group of rehabilitated patients versus 8.3 hours ± 3.7 in the group of non-rehabilitated women. The difference was statistically significant with p value equal to 0.0001. Huang and al. in 2016, reported that early oral rehydration would allow rapid resumption of intestinal transit and early ambulation. It would also reduce the risk of infection, the delay in breast-feeding and the duration of hospitalization [6]. Our results contrast with those of Mangesi and al who, in 2002, found no significant difference in the resumption of intestinal transit between early and late resumption of oral feeding [7].
In our study, on average, early rehabilitation reduced the time to removal of the urinary catheter by 3 hours. Indeed, the ablation of the probe was made within 24 hours after caesarean section in 95.2% of patients benefiting from early rehabilitation. This rate is close to that of Laronch and al in France which was 93% [8]. Ghoreishi and al found in 2003, in a study of indwelling urinary catheters in cesarean delivery, that the use of an indwelling urinary catheter is an unnecessary part of the cesarean delivery process. In addition, urinary retention was very rare [9]. Nevertheless, Pavlin and al found that it would be important to combine this strategy with a monitoring protocol for voiding [10].
The mean time to ablation of the peripheral venous line was 24.3 hours ± 2.4 in the group of rehabilitated women versus 22.3 hours ± 5.6 in the non-rehabilitated group (p=0.0003). The venous line was removed in all patients within 24 hours after surgery. This rate is similar to that found by Laronche and al in Paris in 2017, which was 98% [8]. However, it is superior to that found by Jacques and al in France which was 49% [11]. A practice survey of maternity wards in the Provence-Alpes-Côte d'Azur and Île-de-France regions in 2013 revealed that the venous line was maintained for 24 hours after the procedure in 70% of patients who received planned caesarean section [12]. Although maintaining the venous line is a brake on regaining autonomy, the need to administer oxytocics and intravenous analgesics would lead practitioners to keep the venous line for 24 hours. In our study, the absence of complications in the immediate postpartum in early rehabilitated patients justified the removal of the venous line within 24 hours after cesarean section.
Functional recovery
Early rehabilitation significantly reduced first rise time by nearly one hour (7.2 hours vs. 8.1). The difference was significant with p=0.01. Mazard and al in France in 2015 found an average delay close to 9 hours ± 4.2 [13]. Randriambololona in Antananarivo in 2018 was higher than ours (16.4 hours) [14]. Getting up early is a fundamental point of early rehabilitation. It allows patient autonomy and prevention of thromboembolic risk. The results of our study are much better since the first sunrise took place at the 12th hour in 99.2% in rehabilitated women compared to 78.9% in non-rehabilitated ones (p = 0.05). In fact, James and al in France had only 53.3% of women having their first birth the day after the cesarean section [11].
The mean walking time was 16.4 ± 3.6 hours in the group of rehabilitated women vs. 20.9 ± 8.5 hours in the group of non-rehabilitated ones (p less than 0.05).
Our study showed an increase in the rate of early ambulation in patients who had benefited from early rehabilitation. In fact, all the patients who had benefited from early rehabilitation had ambulated within 24 hours after the cesarean compared to 68.5% in patients who had benefited from the usual protocol. These figures corroborate those found by Lee and al who reported a significant increase (p=0.001) in early ambulation from 33 to 51
Postoperative pain
This study revealed to us that at the 12thhour there was no statistically significant difference in the pain experienced by the two groups of patients, both at rest (p=0.14) and during mobilization (p greater than0.99). This could be explained by the fact that the two groups of patients benefited from the same analgesia made of paracetamol 1gram associated with nefopam 20 micrograms until the 6th postoperative time.
In patients undergoing early rehabilitation at 24th hour the early rehabilitation protocol significantly reduced postoperative pain by 0.3 at rest (p=0.0000) and by 0.2 at mobilization (p=0.004). Similarly, at the 48th hour, there was a significant decrease in pain intensity of 0.3 at rest (p=0.00002) and 0.1 on mobilization (p=0.02). This difference could be explained by the fact that the diclofenac suppository had been systematically combined every 12 hours for 48 hours in the early rehabilitation protocol, which was not the case for the usual protocol.
In the literature, several authors have conducted comparative studies of the level of pain felt between two groups of patients benefiting from early postoperative rehabilitation and not. Elgohary and al in 2017 compared the intensity of pain between a group of patients benefiting from early rehabilitation and another from conventional rehabilitation as part of scheduled colorectal surgery and found a statistically significant difference (p less than 0.001) (16). As for Meyer and al. in 2018, they found no statistically significant difference for the same type of study conducted on two groups of patients who had undergone obstetric surgery (P= 0.80) [17]
Scalable data
Nausea/vomiting was at the forefront with 16.1% in the group of rehabilitated women and 14.5% in the group of those not rehabilitated. There was no statistically significant difference between the two groups with p=0.7.
Our results are higher than the 6.6 and 8.7 found by Moris B and al in 2019 in Uganda respectively in the rehabilitated and non-rehabilitated groups [18]. On the other hand, in his series, Randriambololona in 2018 at the University Hospital of Befelatanana reported a higher rate with a percentage of nausea/vomiting complications of 21.43% [14]. As for infectious complications, he found no significant difference between the two groups p=0.3. During the first lift, 24.2% of patients rehabilitated in our study compared to 58.8% of those not rehabilitated had presented with discomfort. The difference was statistically significant between the two groups with p less than0.05 Moris B and al also found a statistically significant difference between the groups of rehabilitated (6.6%) and non-rehabilitated (30.4%) patients [18].
The patients who had benefited from the early rehabilitation protocol were authorized to leave the maternity ward earlier than the other patients (2.9 days versus 3.5 days, p less than0.05). The rehabilitation protocol had significantly (p less than 0.05) reduced the duration of hospitalization by an average of 12 hours. This reduction in hospital stay is similar to that reported by Rousseau et al in France in 2017 which was 10 hours [19]. The main fear of early discharge remains the risk of rehospitalization. But Wrench and al in England found that patients who were discharged on the first day after caesarean section using an early rehabilitation protocol were no more rehospitalized than those discharged on the second day after caesarean section [20]. Of course, the early discharge of patients implies a good city–hospital relay. A discharge on the third day after the caesarean section requires that the medical team has ensured that returning home is possible on the basis of the acquisition of various prerequisites by the mother (mother-child relationship,18
breastfeeding, newborn care). These prerequisites are achieved more quickly with the application of early rehabilitation since the mother can get up on her own, without being bothered by a urinary catheter or an infusion. As a result, the mother can be autonomous with her child before the 12th post cesarean hour. In our study, 99.2% of patients benefiting from early rehabilitation had made their first rise before the 12th hour, which would explain this reduction in hospital stay.
The average cost of care for patients in the early rehabilitation group was 89516.1 CFA money ± 9699.1 versus 97612.9 CFA money ± 29070.1 (i.e. respectively 179 USD±19.4 vs 195.23 USD±58, 14) in the group of unrehabilitated women (p= 0.003). The earlier authorization for patients to leave the hospital, made possible thanks to the application of this protocol, seems to have contributed to significant savings for the health system. Orji and al in Nigeria found that women in the rehabilitated group required less intravenous fluid than those in the non-rehabilitated group [21], which may explain the lower cost of treatment. Also our results are similar to those of Fay and al in the United States of America in 2019 who found that total postoperative direct costs decreased [22].
This study revealed to us that patients who benefit from early rehabilitation had faster empowerment. This empowerment was favored by adequate management of postoperative pain, faster removal of medical devices, early oral nutrition and early mobilization. The study also allowed us to observe a reduction in the duration of hospitalization and a significant drop in the cost of caesarean section management. Maternal satisfaction and the mother-child relationship were not addressed in the study. Further studies integrating these aspects should make it possible to refine the benefits of early rehabilitation in obstetrics at the Yalgado Ouedraogo teaching hospital or even beyond.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the authorization of the ethics committee. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
SWCL and KBE prepared the manuscript, SWCL collected the data, SA analyzed the data, SDA, BT and DB provided a useful review of this manuscript. All authors contributed to the article and approved the submitted version.
The authors would like to thank all patients for their consent obtained. The authors also thank all the staff who contributed to the care of the patients. They would also like to thank Meighan Mary for her contributions to the writing in English.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
