
Research Article | DOI: https://doi.org/10.31579/2641-0419/011
1 Department of Public Health and Community Medicine/Primary Health Care Sweden.
*Corresponding Author: Nasser S. Ahmadi, Department of Public Health and Community Medicine/Primary Health Care Sweden.
Citation: Nasser S. Ahmadi, Ulf Lindblad, Jörgen Månsson, Dyspnoea Symptom Intensity And Impact On Health-Related Quality Of Life In Patients With Cardiovascular Or Pulmonary Diseases: A Longitudinal Observational Study, Clinical Cardiology and Cardiovascular Interventions. 2(1); Doi:10.31579/2641-0419/011
Copyright: © 2018 Nasser S. Ahmadi, This is an open-access article distributed under the terms of the
Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any
medium, provided the original author and source are credited
Received: 01 February 2019 | Accepted: 29 January 2019 | Published: 18 February 2019
Keywords: dyspnoea; heart failure; COPD; one-dimensional scales; SF-36; HRQoL; primary care
Introduction: Dyspnoea is a prevalent symptom associated with significantly reduced health-related quality of life (HRQoL). Accurate estimates of the severity and intensity of dyspnoea using standard tools in the clinic are important for the assessment of the severity of symptoms at later follow ups.
Objectives: The current study had two aims. First, we sought to determine one-year changes in dyspnoea and health-related quality of life in patients with cardiac or respiratory diseases. Second, we sought to analyse the long-term associations between one-dimensional measurement methods and a generic instrument reflecting the multi-dimensionality of dyspnoea using the Short-Form Health Survey (SF-36).
Methods: We prospectively recruited adult dyspnoeic patients in a rural primary health care centre. Participants were assessed for demographics, symptoms, medications, and N-terminal B-Type natriuretic pro-peptide (Nt-proBNP) level, and underwent spirometry and echocardiography. Results were analysed at baseline and one-year after enrolment. Based on the assessment results, we categorized the patients into one of three groups as the underlying disorder for dyspnoea: cardiovascular, pulmonary or psychiatric disease.
Results: The ordinal scales [New York Heart Association (NYHA), modified Medical Research Council (mMRC) and Verbal Rating Scale (VRS)] indicated a slight but not significant decrease in dyspnoea severity, whereas the VAS showed a significant reduction in dyspnoea severity (p = 0.001) overall as well as in the cardiovascular group. By contrast, patients with pulmonary disease showed no improvement. HRQoL, as determined by the eight domains of SF-36, was unchanged, and dyspnoea severity had no impact on the worsening of health status.
The correlation coefficient by test-re-test (reliability) of values at baseline and at the end of the study was highly significant.
Conclusion: As appropriate measurements for the assessment of dyspnoea using one-dimensional scales, both mMRC and VAS should be considered for measuring changes in dyspnoea severity. VAS should be considered particularly for long-term changes in dyspnoeic patients with cardiovascular disorders. Changes in the different domains of the SF-36 were not seen after one year.
Chronic dyspnoea is the most prominent symptom in cardiovascular (1, 2) and pulmonary diseases (3, 4). Anxiety, depression and even neuromuscular diseases can be associated with dyspnoea (5, 6). Therefore, the assessment of dyspnoea occurs along different clinical pathways depending on the suspected underlying aetiology. Currently, measurement of dyspnoea is a mandatory part of patient assessment (7). According to standard guidelines, both symptoms and lung function should be monitored for the management of patients with Chronic Obstructive Pulmonary Disease (COPD) and asthma (8). Monitoring dyspnoea over long-term periods (9, 10) is important to follow how patients respond to therapy due to the negative impact of dyspnoea on the health-related quality of life (HRQoL) (11). However, the lack of a gold standard for such monitoring has been previously reported (12). Despite the recommendations for using the modified Medical Research Council (mMRC) (13), its effectiveness for long-term follow up has been questioned (9).
The complexity of dyspnoea as a symptom reflects two main different clinical outcomes that are experienced by the patient. First, the symptoms have an intensity, magnitude and duration and, second, symptoms have an impact on the everyday life of the patient that affects their quality of life (14). Therefore, it is appropriate to include patient-reported dyspnoea measurements (PROs), which provide a measure of the health status as reported directly by the patients (15, 16). Several reliable scales with high validity exist that measure both outcomes. The most used scales are one-dimensional scales measuring different qualities of dyspnoea such as intensity and severity [i.e., Verbal Rating Scale (VRS), and Visual Analogue Scale (VAS)] and impact on physical activity [i.e., mMRC]. The potential of the New York Heart Association (NYHA) scale, used primarily for classifying congestive heart failure (CHF), lies in its ability to rate dyspnoea and fatigue. The Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) is a generic measure of functional health and well-being that was validated in Sweden (17) and widely used in research as a generic measure of health-related quality of life (HRQoL). The SF-36 was used in the current study to examine the impact of dyspnoea on the everyday lives of the participants.
Although worsening dyspnoea with optimal treatment is slow and difficult to detect (18), investigating the longitudinal changes associated with dyspnoea under circumstances of “conventional therapy” improves our knowledge about the follow-up, therapy adjustment and prognosis for patients with cardiopulmonary diseases. The few observational studies (9, 18-20) investigating the longitudinal changes in dyspnoea showed that dyspnoea becomes worse over time among patients with COPD. However, more studies are required, particularly in primary care, because of the existing uncertainty regarding the long-term changes of dyspnoea severity perceived by patients suffering from cardiopulmonary dyspnoea. Analysing the relationships and understanding the various perceptions and domains of dyspnoea is a clinically important matter that enables clinicians to choose accurate diagnostic pathways and effective treatment regimens for the assessment of dyspnoeic patients.
The primary aim of this paper was to compare the changes in dyspnoea and HRQoL in patients with diseases that commonly cause dyspnoea, such as cardiovascular and respiratory conditions. The secondary aim of this study was to analyse the long-term associations between one-dimensional measurement methods and a generic scale reflecting the multi-dimensionality of dyspnoea using SF-36.
We employed an observational, longitudinal design that was conducted in a single health centre in Orust, which is an island located in western Sweden and consists of 15,000 inhabitants.
The inclusion process began in December 2013 and continued for two years. The follow-up period ended in December 2015. We identified 115 patients who were seeking medical advice for dyspnoea in our health centre during the two years of data collection for this study. A total of 89 participants were enrolled in our study (2013 to 2014; Fig. 1).
Participants were required to meet all of the following criteria: Adults (aged ≥ 18 years), duration of perceived dyspnoea ≥ six weeks and no previous investigation of the symptoms. Exclusion criteria were dementia or psychotic disorders. Assessments of the participants were conducted by trained personnel within three weeks after first contact. In this study we focused primarily on patients with cardiac or respiratory illnesses. Patients with no cardiopulmonary disease or participants with unknown aetiologies (8 patients) were excluded during the follow-up period, which was predetermined as one year after the enrolment date.
An experienced nurse collected peripheral blood samples for routine biochemical tests, including N-terminal B-Type natriuretic pro-peptide (Nt-proBNP). A medical history was taken and a clinical examination performed at baseline by a physician specializing in cardiology and family medicine (NSA). All participants were examined again one month later and were informed about the results of the blood samples and physical examinations.
All participants were referred to spirometry and echocardiography, and all were subjected to an electrocardiography (ECG) exam. When a diagnostic process was required, patients were examined by X-ray, CT scan or sonography. CHF was diagnosed by an Nt-proBNP value > 400 pmol/L and an Left Ventricular Ejection Fraction (LVEF) value less than 45. A diagnosis of COPD was based on the maximal FEV1/forced vital capacity ratio of less than 0.7 and a post-bronchodilator FEV1 of less than 80% of the predicted normal value. Restrictive respiratory problems included extra pulmonary causes, such as obesity, and intrinsic pulmonary pathology, such as interstitial fibrosis. The intervention administered was the conventional treatment given by each caregiver according to national and international guidelines. The follow-up period ended 12 months after the initial clinical contact. Both baseline and one-year data were obtained by sending a booklet containing the measurement scales and questionnaires described below to the participants.
The patient-reported clinical outcomes gathered at baseline were obtained using a booklet sent to the patients prior to the first meeting. The patients read the 5-point mMRC scale and circled the grade (0–4) that most closely matched his/her degree of breathlessness. Higher scores represent more severe breathlessness. NYHA was included in the same booklet, and participants marked the severity of their perceived dyspnoea at that point in time. For the VAS, the participant marked on a line (0-100 mm) the value corresponding to their extent of breathlessness. A similar procedure was performed for the Verbal Rating Scale (VRS), but this scale was ordinal in nature defined by four different severity grades from no dyspnoea to severe dyspnoea.
All participants were asked to evaluate their HRQoL by answering questions in the SF-36 at baseline and one year after baseline measurements. The scores (0 to 100) were summed, and higher scores represented better patient condition.
Data were analysed using SPSS Version 21software for Windows 8.1 (SPSS, Inc., Gothenburg, Sweden). The following factors were considered in the current study: the number of participants, baseline characteristics, method of analysis and study duration.
The patient characteristics and demographics were calculated using descriptive statistics. The main comparison of interest was the difference in symptom scores at baseline and one year after baseline in each disease category and between the categories. Comparisons in this case were conducted using a pair-sampled t-test. The difference between the various measurement scales was estimated using an independent sample t-test. We considered a difference of 10% in symptom score (for any of the four measurement scales mMRC, NYHA, VAS or VRS) or domains of SF-36 over the course of the study to be clinically significant. A sample size of 30 per group for those with dyspnoea of various aetiologies provided 80% power to detect a 10% difference using p < 0.05 in the VAS, which was calculated prior to the study. Ordinal data were analysed by cross tabs, and p-values were calculated using a Chi-squared test. Within-subject Spearman correlation coefficients and corresponding p-values as well as a t-test for mean comparisons were calculated for all participants. The internal consistency and reliability were calculated using Cronbach’s Alfa. For all statistical tests, alpha was set at 0.05.
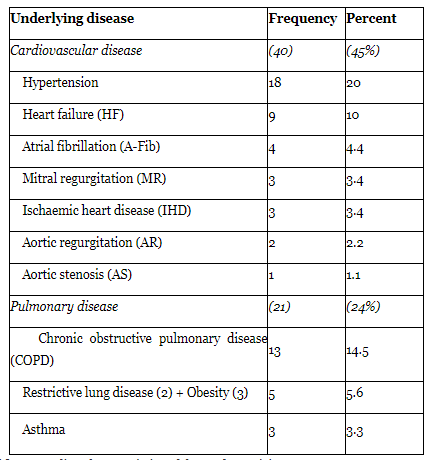
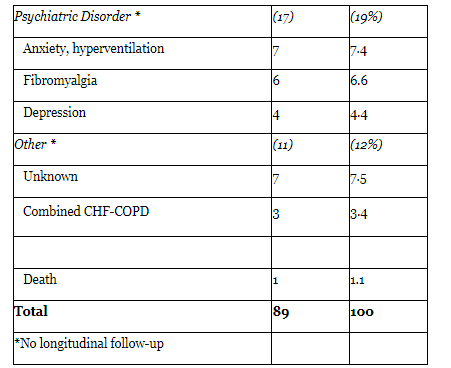
A total of 89 patients seeking treatment for dyspnoea were included for the baseline analysis. The selection process is displayed in Figure 1. After the initial assessment, we categorized the patients into one of three categories according to their underlying disease. The first category included all patients with cardiovascular disease (40 patients, 15 females) and the two remaining groups included patients with pulmonary (21 patients, 12 females) and psychiatric diseases (17 patients, 9 females). The diagnosis was based on findings at the baseline examination related to patient history and echocardiography, spirometry and other laboratory findings. The baseline characteristics of the three categories are displayed in Table 1. Eight patients presented with an unknown diagnosis even after assessment, two patients presented with neurological disorders, and one patient died during the follow-up period (Table 2). The patients with unknown diagnoses (seven subjects) or with combined HF and COPD (Three individuals) were not included in the one-year follow up visit. One patient died of a thoracic aortic aneurysm during the study period.
The mean age for the entire study population with dyspnoea was 68 ± 10 years, whereas the mean age for participants with cardiovascular disease was 71.5 ± 9.5 years (p < 0.02). Nt-proBNP, a marker for heart failure, was significantly higher in patients with cardiovascular disease compared with the other groups (p < 0.001). There were no significant differences in smoking habits or comorbidities, such as hypertension or diabetes mellitus type 2, among the groups. The majority of patients with CHF were treated with angiotensin-converting enzyme (ACE) inhibitors, mainly enalapril, angiotensin II receptor blockers, such as losartan, beta blockers, such as metoprolol, carvedilol, and diuretics. The treatment for patients with COPD or asthma was mainly bronchodilators such as tiotropium, salmeterol in combination with the inhaled steroids fluticasone and budesonide or combination inhalers. We observed a significantly higher frequency of medication with only a beta-blocker among patients with

The frequencies of underlying aetiologies for dyspnoea are presented in detail in Table 2.
The intensity and severity of dyspnoea measured by each one-dimensional scale for patients in both categories of disease at baseline and one year after baseline are presented in
Table 3. The ordinal scales (NYHA, mMRC and VRS) indicated a slightly but not significant decrease in dyspnoea intensity at the end of the study compared with baseline. By contrast, VAS showed a significant overall reduction in dyspnoea (p = 0.001) in the cardiovascular group. However, the patients with pulmonary disease did not show any change.
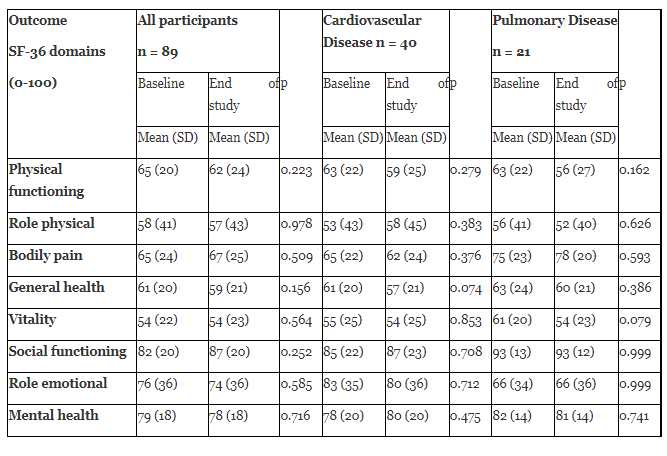
HRQoL, which was determined by the eight domains of the SF-36, did not show any significant change in any disease category, as changes were not observed in the physical or psychosocial domains of the SF-36. However, patients with cardiovascular disease who rated their health status better than at baseline mostly showed differences in the domain about general health, which is a measure of self-rated health. By contrast, patients with pulmonary disease displayed better vitality, but this improvement did not meet our significance criteria
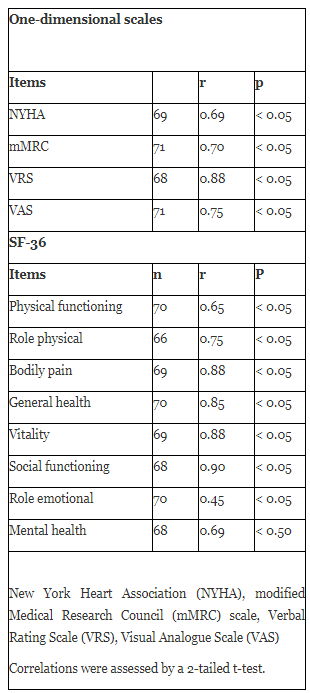
The correlation coefficient by test-re-test (reliability) of values at baseline and at the end of the study was greater than 0.65 for almost all parameters included in the study, which reached significance and suggests good reliability for the tests
In our study, patient-reported outcomes rated by one-dimensional scales and a multi-dimensional scale (SF-36) were measured among patients with perceived dyspnoea in two different disease categories (cardiovascular and pulmonary disease). Regarding our first research question, we found that the one-dimensional scales (mMRC, VAS and VRS) did not show worsening of dyspnoea after one year of follow-up. By contrast, the VAS scale showed a significant improvement in dyspnoea severity in the cardiac disease group, which could lead to better standardization of dyspnoea outcome measures for more precise comparisons in the future (21). This result is consistent with those of previous studies (9, 20). A corresponding improvement was not observed in patients with pulmonary dyspnoea (18).
Despite the few observational studies describing longitudinal changes in dyspnoea patients, more knowledge is needed in this important area. In a study conducted by Mahler et al. (9), in 70 patients with COPD assessed with the mMRC criteria, the authors found that the Transition Dyspnoea Index (TDI) indicated significant deterioration of dyspnoea patients, whereas the mMRC could not detect a difference. We found weak improvement in the general health and vitality of patients with cardiac and pulmonary diseases one year after conventional treatment. In a recent study, an affective/emotional dimension was linked to dyspnoea (22), but the mental health domain showed no changes over time in our study.
The second objective of our study was to analyse the long-term associations between one-dimensional measurement methods and different domains of the SF-36. Based on these observations, we found a significant association and acceptable test-re-test reliability of all included parameters. Additionally, the most obvious finding to emerge from our analyses was the role of Nt-proBNP, which is not only a marker of heart failure but is also a good discriminator of dyspnoea based on cardiac or pulmonary aetiologies, a finding that is consistent with previous studies (23).
One strength of our study is that we focused on a representative population in a rural area from a primary care perspective. Using different one-dimensional measurement scales and the SF-36 in such a setting gave us new insight into how theses scales relate to each other and how the obtained information can be compared more accurately. Nonetheless, further studies are necessary to determine the pros and cons for each assessment scale.
To obtain better and more reliable results, a study designed as a clinical trial with a control group, a larger initial sample size, longer duration and a multi-centre nature should be performed. Another limitation of our study is that we did not assess lung function. However, previous studies did not demonstrate a correlation between lung function tests and dyspnoea severity over long-term periods (20). Dyspnoea is associated with many chronic diseases, and it is important to assess the intensity and severity perceived by individual patients. This measure could help with obtaining a better understanding and estimation of the symptoms of dyspnoea. Moreover, we believe that novel ways to understand symptoms, such as fatigue, pain or breathlessness, can be useful methods for the early detection of chronic diseases and can serve as an important part of the successful treatment of dyspnoeic patients (24).
Since dyspnea shows tendency to worsen over time, it is important to have a reliable measuring scale than can be used effectively in a short time during the consultation. We suggest that one-dimensional scales such as mMRC and VAS, particularly VAS, are appropriate measurements for the long-term assessment of dyspnoea. The latter one reflects the effect of treatment better among patients suffering from cardiovascular diseases.
ATS, American Thoracic Society; BMI, Body Mass Index; COPD, Chronic Obstructive Pulmonary Disease ; HRQoL, Health-Related Quality of Life; mMRC, modified Medical Research Council; NYHA, New York Heart Association; PROs, Patient-Reported Outcomes; QoL, Quality of Life; SF-36, Short Form 36; VAS, Visual Analogue Scale; VRS, Verbal Rating Scale.
The authors are grateful to the participants in the study, the study assistants RN Johanna Henriksson, Ann-Britt Nyström and especially administrators and the staff at the Capio Orust Health Centre. We also want to thank the Capio research aid, Sahlgrenska Academy and the Fyrbodal Research and Development Council (R&D Fyrbodal), supporting this study.
The study was conceived by NSA, UL, and JM. NSA performed the clinical examinations, data collections, data analyses and drafted the paper. All the authors provided their intellectual inputs; All the authors read, edited, and approved the final manuscript.
The authors declare that they have no competing interests.
SF-36 is a licensed product and license was obtained by payment from optum tm (license no. QM026775)
The study was approved by the Regional Ethical Review Board (registration nr. 786-11) at the University of Gothenburg and was conducted in accordance with the Declaration of Helsinki. Patients provided written, informed consent to participate in the study and all patients agreed at enrolment to participate in the study? Participants were informed about their freedom for refusal and regardless of which decision they may take, would not affect their right for healthcare services. Anonymity and confidentiality were maintained throughout the research process.
Figure 1. Flowchart of eligibility and participants included i
Adult participants with chronic dyspnea n=115
Initially included
n=107
Participation confirmed
n=93
A cross sectional previous study n=89
Current study Included
n=65
Eight participants excluded because they did not meet the inclusion criteria (-8)
Seventeen participants with no cardiovascular or pulmonary diseases and seven undiagnosed cases excluded (-24)
Four drop outs after first contact (-4)
Fourteen drop outs before initial assessments (-14)
Three participants with combined CHF-COPD and one death (-4)
21 patients with Respiratory disease
40 patients with Cardiovascular disease
Figure 1. Flowchart of eligibility and participants included in the study III and IV
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
