
Case Report | DOI: https://doi.org/10.31579/2640-1053/126
1 Cancer Center of Southern California/Sarcoma Oncology Research Center, Santa Monica, CA, USA.
2 Aveni Foundation, Santa Monica CA, USA.
3 Terasaki Institute, Los Angeles, CA, USA.
4 NKGen Biotech, Inc., Santa Ana, CA, USA.
*Corresponding Author: Erlinda M. Gordon, Cancer Center of Southern California/Sarcoma Oncology Research Center 2811 Wilshire Boulevard, Suite 414 Santa Monica, CA 90403, USA.
Citation: Erlinda M. Gordon, Sant P. Chawla, Victoria S Chua-Alcala, Don A Brigham, Amir Ahari, et al. (2022). Durable Responses Using SNK01 Autologous Enhanced Natural Killer Cells and Pembrolizumab for Chemotherapy-Resistant Advanced Sarcoma: Case Reports, Literature Review and Future Perspectives. J. Cancer Research and Cellular Therapeutics. 6(5); DOI:10.31579/2640-1053/126
Copyright: © 2022 Erlinda M. Gordon, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 July 2022 | Accepted: 13 July 2022 | Published: 05 September 2022
Keywords: SNK01; autologous natural killer cells; immune checkpoint inhibitor; program death ligand-1; PD-1; PD-L1; pembrolizumab; sarcoma; immunotherapy; cell therapy
Advanced or metastatic sarcoma is associated with an invariably fatal outcome. Two noteworthy cases of chemotherapy-resistant metastatic sarcoma with durable responses to SNK01 autologous enhanced natural killer cell therapy and pembrolizumab, an immune checkpoint inhibitor, are reported here. Single patient use of SNK01 and pembrolizumab was authorized by the United States Food and Drug Administration and a Central Institutional Review Board. After informed consent was obtained, Patient #1 with desmoplastic small round cell tumor and Patient #2 with radiation-induced chondrosarcoma received SNK01 2x109 cells i.v. and 200 mg pembrolizumab i.v. every 3 weeks. Patient #1’s tumors gradually decreased in size, achieving a 47% partial response after which the patient underwent two surgical resections and achieved a sustained remission. Patient #2’s tumors gradually decreased in size, achieving a 38% partial response. Albeit a very small case study, the data suggest that SNK01 plus pembrolizumab may be a viable therapeutic option for patients with chemotherapy-resistant advanced sarcoma with manageable toxicity, and supports existing evidence that natural killer cells mediate a favorable response to immune checkpoint inhibitor therapy while reducing immune-related adverse events.
Immunotherapy for sarcoma has not, hitherto, shown impressive clinical benefit as in other solid tumors. However, in principle, natural killer cell function within the tumor may be revived with the use of immune checkpoint inhibitors [1]. Recent evidence has implicated a profound role of natural killer cells in the immune checkpoint inhibitor pathway and suggests that natural killer cells can improve program death ligand 1 (PD-L1) - negative tumor response to immune checkpoint inhibitor therapy [2]. Given that natural killer cells have also been found to target and eliminate autoreactive T-cells, natural killer cells could possibly reduce autoimmune-like side effects associated with immune checkpoint inhibitor therapy as well [3].
SNK01 is a first-in-kind, autologous non-genetically modified natural killer cell therapy with highly enhanced cytotoxicity and over 90
Two single patient investigational new drug applications using SNK01 and pembrolizumab for advanced sarcoma were authorized by the United States Food and Drug Administration/Center of Biologic Evaluation and Research (USFDA/CBER), Bethesda, MD, USA, and approved by Western Institutional Review Board, Olympia, WA, USA. The treatment protocol consisted of autologous enhanced natural killer (SNK01) cells at a dose of 2 x 109 cells i.v. and pembrolizumab 200 mg i.v. every 3 weeks, followed by surgical debulking of residual disease if possible. Treatment outcome parameters included best overall response and progression-free survival using RECIST v1.1 [6], overall survival and incidence of treatment related adverse events using NCI NIH Common
toxicity Criteria for Adverse Events version 5.0 [7]. Stopping rules included serious treatment-related adverse events that did not improve to Grade 1 or less severity after 3 weeks.
Patient # 1: A 32-year-old hispanic male was diagnosed to have metastatic desmoplastic small round cell tumor in December 2016 for which the patient received multiple chemotherapy regimens including vincristine sulfate, doxorubicin, cyclophosphamide + ifosfamide, and etoposide phosphate followed by aldoxorubicin, irinotecan, vincristine and temozolomide. The patient then received trabectedin and pembrolizumab until disease progression in October 2019. In November 2019, the patient was enrolled in Cohort 1 of SNK01 Phase 1 study, wherein he received five weekly doses of SNK01 at a dose of 1 x 109 cells/dose. After five treatments, a follow-up CT scan revealed stable disease, although at that time, he still had extensive liver metastases with massive abdominal and pelvic disease. Because intra-patient dose escalation was not allowed in the Phase 1 study, and to improve tumor response, a single patient investigational new drug application using SNK01 and pembrolizumab was authorized by the USFDA based on a publication demonstrating how natural killer cells could play a significant role in responses of patients with PD-L1 negative tumors [2]. The patient’s tumors decreased in size over one year of treatment to a 47% partial response by RECIST v1.1 [6]. In March 2021, he underwent a surgical debulking procedure followed by whole abdominal radiation and intraperitoneal chemotherapy, after which he resumed SNK01 and pembrolizumab regimen in May 2021. His last scan in January 2022 showed sustained remission with no evidence of disease (Figure 1).
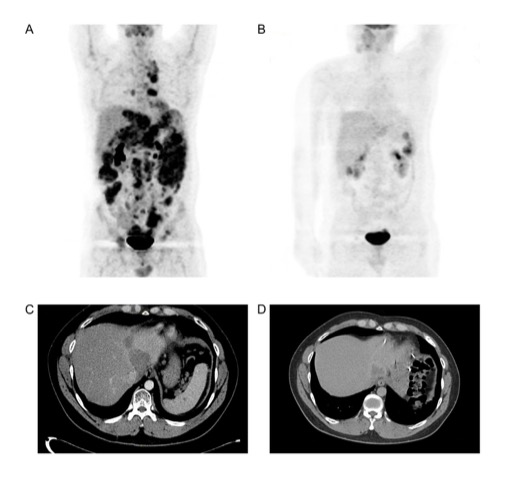
(A) PET scan before treatment; (B) PET scan after SNK01 plus pembrolizumab treatment
followed by debulking procedure; (C) Abdominal CT scan before treatment; (D) Abdominal
CT scan after SNK01 plus pembrolizumab treatment followed by debulking procedure. FDG
PET: Fluorodeoxyglucose Positron Emission Tomography; CT: Computerized Tomography.
He has now received 32 cycles of SNK01 + pembrolizumab over 28 months and has an Eastern Cooperative Oncology Group score of 0 (fully active, able to carry on all pre-disease performance without restriction). Grade 2 treatment-related adverse events included hypothyroidism, fatigue, rash, and pruritus. There were no > Grade 3 treatment-related adverse events reported.
Patient #2: A 57-year-old white male was diagnosed to have a high-grade pleomorphic liposarcoma of the right pelvis in 2004. The patient underwent pre-operative doxorubicin, ifosfamide, mesna, and radiotherapy. He then received adjuvant interferon for 2 years. In January 2019, a biopsy of the right iliac crest revealed PD-L1 positive radiation-induced chondrosarcoma. The patient underwent a two-stage surgical procedure including right hemipelvectomy and proximal femoral replacement in March 2019. The patient then received nivolumab in August 2019 until disease progression. Other targeted therapies included palbociclib and pazopanib until disease progression in June 2020. The USFDA then authorized a single patient use investigational new drug application using SNK01 2 x 109 cells and pembrolizumab 200 mg every 3 weeks and the patient had a 38% partial response by RECIST v1.1 [6] after four months of treatment (Figure 2).
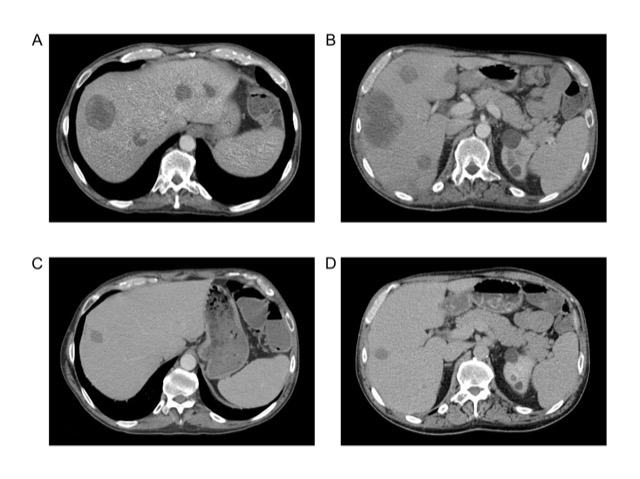
(A, B) Before treatment; (C, D) Four months after treatment.
CT: Computerized Tomography.
He then undertook a surgical debulking procedure, but unfortunately, developed post-operative sepsis and died. The patient had received 18 cycles of SNK01 + pembrolizumab and survived 12 additional months. Grade 3 treatment-related adverse events included increased AST; Grade 2 treatment-related adverse events included hypothyroidism, increased ALT, increased alkaline phosphatase and increased GGT.
In recent years, the efficacy and safety of immune checkpoint inhibitors in advanced sarcoma have been reported. The pioneering SARC028 multicenter phase 2 study investigating the safety and efficacy of pembrolizumab in advanced soft tissue sarcoma and bone sarcoma showed promising activity in certain histologic subtypes [8]. Of 80 patients evaluable for response at 12 center members of the Sarcoma Alliance for Research through Collaboration, seven (18%) of 40 patients with soft tissue sarcoma had an objective response: four (40%) of ten patients with undifferentiated pleomorphic sarcoma, two (20%) of ten patients with liposarcoma, and one (10%) of ten patients with synovial sarcoma. Only 5% of 40 patients with bone sarcoma had an objective response. Nine (11%) patients had serious treatment-related adverse events, five of which were immune-related including adrenal insufficiency, pneumonitis, and nephritis.
In 2018, Chawla et al. reported on their clinical experience with combination chemo-/immunotherapy using trabectedin and nivolumab for advanced soft tissue sarcoma [9]. Twenty-eight heavily treated patients received trabectedin (1.5 mg/m2 via continuous intravenous infusion for 24 hours) every 3 weeks, and nivolumab (3 mg/kg intravenously over 30 minutes) every 2 weeks. Tumor responses were assessed by RECIST v1.1 [6]. All patients had metastatic disease and a median of 4 lines of prior chemotherapy. Best overall response rate was 18.2%, median progression-free survival was 45.4 weeks (range: 10-95 weeks), median overall survival was 66.5 weeks (10-95 weeks), 6-month progression-free survival rate was 68.2%, and 6-month overall survival was rate 95.4%. Safety analysis in 28 patients showed > Grade 3 treatment-related adverse events including anemia (7%), fatigue (3.6%), thrombocytopenia (3.6%), neutropenia (3.6%) and increased creatine kinase (3.6%). Taken together, the data suggested that paired administration of trabectedin and nivolumab is safe, and that this chemo-/immuno-therapy approach may have synergistic activity that could lead to improved clinical outcomes.
In 2021, Chawla et al. (10) reported on the results of the TNT study, a Phase 2 study using Talimogene Laherparepvec, Nivolumab and Trabectedin for previously treated advanced soft tissue sarcoma (NCT03886311). Best overall response (complete and partial responses) was 11% and disease control rate was 80.6%. Safety analysis in 47 patients showed the following > Grade 3 treatment-related adverse events: anemia (25.5%), increased ALT (17%), fatigue (8.5%), thrombocytopenia (8.5%), and neutropenia (8.5%). There was no > Grade 3 injection site reaction with talimogene laherparepvec intratumoral injections. Further, there was one conversion of an unresectable to resectable tumor, showing 100% tumor necrosis on histopathologic examination. Taken together, the data indicated that the TNT protocol may be effective as second/third line therapy for advanced soft tissue sarcoma, with no new safety signals seen.
Recently, Gordon et al. reported on the results of a five-year study using the SAINT protocol: A Phase 2 study using Safe Amounts of Ipilimumab, Nivolumab and Trabectedin as first-line therapy for previously untreated patients with advanced soft tissue sarcoma [11]. The guiding hypothesis was that sarcoma cells are more immunogenic earlier in the course of the disease [12] and that immune checkpoint inhibitors that promote sustained T cell activation would be most effective when given as first-line therapy, together with a tumoricidal agent, trabectedin, that depletes the tumor microenvironment of growth-promoting macrophages. In this article, best overall response was 21.6% with 87.5% disease control rate in 88 patients. Median progression-free survival was 7 (range:1-44) months, median overall survival was 14 (range: 1-46) months. Grade 3 or greater treatment-related adverse events included increased ALT (29.5%), anemia (11.4%), increased AST (11.4%), fatigue (9.1%), neutropenia (6.8%), thrombocytopenia (4.5%), hyponatremia (2.3%), increased ALP (2.3%), port site infection (2.3%), increased CK (2.3%), psoriasis exacerbation (1.1%), adrenal insufficiency (1.1%), dehydration (1.1%), and rhabdomyolysis (1.1%). There was no incidence of alopecia nor cardiac toxicity reported. Taken together, by indirect comparison, these data indicate that first-line combinatorial therapy with the SAINT protocol (1) may be more effective than standard first line therapy (doxorubicin/ifosfamide/mesna), and (2) may be safer than standard first line therapy for advanced soft tissue sarcoma.
Natural killer cells of the innate immune system play a key role as the main effector cells against cancer. In recent years, there has been increasing evidence of natural killer cell-mediated immunosurveillance of sarcoma cells, highlighting the potential of using natural killer cells as a therapeutic tool against sarcoma [13]. Hence, a rational approach would be to boost innate natural killer cell-mediated anti-tumor activity with ex vivo activated natural killer cells. Autologous natural killer cells have always been challenging to grow ex vivo, especially when derived from chemotherapy-treated patients. Thus, universal allogeneic donor-derived products have been mostly used [14]. SNK01 is the first-in-kind, autologous, non-genetically modified natural killer cell product with significant anti-tumor cytotoxicity and over 90% expression of cell determinants CD16, NKG2D, NKp46, and DNAM-1, that can be consistently produced even from chemotherapy-treated cancer patients [4]. While most, if not all, natural killer cell therapies have focused on hematologic malignancies, SNK01 has been shown to exhibit strong activity against both hematologic malignancies and solid tumors in preclinical studies. For patients with advanced sarcomas in the relapsed/refractory setting, there are few, if any, effective salvage treatment options. Monotherapy with PD-L1 inhibitors have shown only modest activity in most sarcomas, especially in tumors that have little to no PD-L1 expression [2,8]. In our experience, SNK01 can be safely administered without the need for lymphodepletion [4]. Interim results of Cohort 4 of a Phase 1 study using SNK01 cell therapy and avelumab, a PD-L1 immune checkpoint inhibitor for chemotherapy-resistant sarcoma have been reported [15]. These patients were treated with 4 x 109 SNK01 cells and 800 mg of avelumab intravenously every two weeks. Best overall response rate was 13.3% and disease control rate was 33.3%. Response was independent of PD-L1 status. Three of 15 patients had a grade 2/3 adverse event which was related to avelumab. There were no adverse events related to SNK01. The authors concluded that combinatorial therapy with SNK01 and avelumab may be safe with antitumor activity in advanced sarcoma that is independent of PD-L1 status.
Albeit these are very small studies that require confirmation in a larger randomized Phase 2 study, the interim results of the on-going Phase 1 study using SNK01 and avelumab for previously treated advanced sarcoma and the promising results of these two case studies suggest that combination therapy using SNK01 and an immune checkpoint inhibitor may improve treatment outcome of patients with advanced chemotherapy-resistant sarcoma.
Future perspectives: An interesting concept is that improved efficacy may be achieved by combining SNK01, an immune checkpoint inhibitor and a targeted cell cycle checkpoint inhibitor, e.g., DeltaRex-G, a tumor-targeted retroviral vector (1) that uniquely targets/hunts down tumors, and (2) that kills not only cancer cells/ cancer stem cells, but also proliferative neovasculature, tumor- associated growth-promoting macrophages and tumor associated fibroblasts [16]. Extracellular matrix deposition by tumor-associated fibroblasts down-regulate ligands of natural killer cell- activating receptors [14] and prevent immune cell trafficking in the tumor microenvironment. Reducing extracellular matrix production by DeltaRex-G therapy may enable SNK01 cell entry in the tumor microenvironment, favor natural killer cell-ligand interactions and improve tumor control and treatment outcome.
Taken together, the data (1) suggests that SNK01 plus pembrolizumab may be a viable salvage therapy regimen for chemotherapy-resistant advanced sarcoma with manageable toxicity, and (2) supports existing evidence that natural killer cells mediate a favorable response to immune checkpoint inhibitor therapy while reducing immune-related adverse events. Randomized Phase 2 studies are planned to confirm these encouraging results and biologic insights.
Ethics approval and consent to participate
The clinical protocol was approved by the USFDA/CBER and the Western Institutional Review Board. Written informed consent was obtained from each patient prior to treatment.
Consent for publication was obtained from Patient #1 and from the family of Patient #2.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
EMG, SPC, VSC, AA, CV, EY and DAB have no competing interests. PYC and PYS are employees of and have equity in NKGen Biotech, Inc.
Funded in parts by the Cancer Center of Southern California/Sarcoma Oncology Research Center and the Aveni Foundation. The SNK01 product was provided by NKGen Biotech, Inc. and pembrolizumab was prescribed.
EMG and SPC are the clinical investigators of the clinical trial, conducted the study and evaluated the patients' tumor responses, survival and safety, wrote parts of the manuscript, as well as reviewed and edited the final manuscript. VSC, AA, CV, EY and DAB analyzed the data, reviewed the literature and reviewed and edited the final manuscript. PYC and PYS reviewed the literature, wrote parts of the manuscript, reviewed and edited the final manuscript. All authors have read and approved the final manuscript.
The authors are grateful to Dr. Sandra Chaplan Memorial Fund and Dawn Royal Memorial Fund for their generous donations to the Aveni Foundation (www.avenifoundation.org), and to Heather Gordon (heathergordondrawings.com) for graphic illustrations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
