
Case report | DOI: https://doi.org/10.31579/2578-8868/369
Head of Neurosurgical Department, Juaneda Miramar, Palma de Mallorca, Balearic Islands, Spain
*Corresponding Author: Gonçalo Januário, Juaneda Miramar, Neurosurgical Department, Palma de Mallorca, Balearic Islands, Spain.
Citation: Gonçalo Januário (2025), Duane Syndrome Combined with Intracranial Cisternal Lipoma and Syringomyelia, Case Report and a Review of Literature, J. Neuroscience and Neurological Surgery, 17(4); DOI:10.31579/2578-8868/369
Copyright: © 2025, Gonçalo Januário. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 07 March 2025 | Accepted: 26 March 2025 | Published: 16 April 2025
Keywords: intracranial lipoma; quadrigeminal cistern; duane syndrome; syringomyelia; magnetic resonance imaging
Intracranial lipomas (IL) are very uncommon congenital malformations. Frequently are associated with various brain anomalies as agenesis or dysgenesis of the adjacent structures like corpus callosum or cortical dysplasia.Some IL are asymptomatic, incidentally discovered in brain imaging carried out to any other causes. The most common location is interhemispheric accounting for 45% of cases. In 20-25% they are located in ambient or quadrigeminal cisterns.Duane syndrome (DS) is a congenital type of strabismus. About 80-90% of cases are unilateral and the left eye is more commonly affected. Are there different types of DS and this pathology doesn’t always happen with other conditions, sometimes are associated with hearing disorders, Goldenhar syndrome, Malformations in spine or vertebrae. The patients with this disease may also present other eye-related conditions as cataract, microphthalmos, nystagmus.Differential Diagnosis for DS includes, Okihiro's syndrome, Goldenhar syndrome, Wildervanck syndrome, Moebius Syndrome, Holt-Oram Syndrome, Morning Glory Syndrome, Abducens Nerve Palsy, Brown Syndrome, Marcus Gunn Jaw Winking Syndrome, and Congenital Esotropia.We present a clinical case, very uncommon, in a 12 year old boy with Duane Syndrome that affects the left eye. The patient present also an IL located in the right quadrigeminal cistern. Incidentally, a dorsal syringomyelic lesion was discovered.All of them are uncommon pathologies, an intracranial lipoma with this location, Duane syndrome and thoracic syringomyelia. We did not find any case in the literature that describes the three pathologies in the same patient.
Intracranial lipoma (IL) is a congenital slow-growing, benign tumor made up of adipose tissue. Although they often remain undetected until later in life. Rokitansky was the first author to describe intracranial lipomas in 19th century, 1856. [1] These benign tumors represent less than 0.1% of all intracranial tumors. [2] The most common location of the intracranial lipomas is Interhemispheric accounting for 45% of cases. The other lesion’s locations were clustered in the quadrigeminal/superior cerebellar in 25%, suprasellar/interpeduncular in 14%, cerebellopontine angle in 9%, and sylvian cisterns in 5%. The IL were associated with brain malformations of varying degrees in 55% of cases. An interesting note for potential surgical cases, in 36% of the cases the intracranial vessels and nerves course through the lesions. [3]
They are congenital lesions composed of adipose tissue resulting from abnormal persistence as well as altered differentiation of the primitive embryonic meninges during the development of the subarachnoid cisterns. The altered differentiation of the meningeal tissue during embryogenesis is its most likely origin. This embryologic concept of the development of IL presents a theory to explain the high frequency of callosal and other brain hypoplasias associated with this benign lesion. [4]
Some IL are asymptomatic, incidentally discovered in brain imaging carried out to any other organic cause. Symptoms, if present, are associated with increased intracranial pressure, obstructive hydrocephalus, or seizures. They can manifest with headache, mental dysfunction, and cranial nerve deficits. [5,6,7] Clinical manifestations depends on the location of the lesion and mainly are asymptomatic, represent incidental lesions, discovered on Computed Tomography (CT) or Magnetic Resonance Imaging (MRI), performed for other reason such as head trauma or headaches. The typical findings in both imaging techniques are the presence of a lesion with appearance and characteristics compatible with fat. On CT scan, IL appear as a non-enhancing lesion with uniform fat density, in some cases may exist peripheral calcification. The CT and MRI features are often pathognomonic for intracranial lipomas.7The treatment are manly conservative, and surgical procedure is indicated in situations with cosmetic defects that require resection of the extracranial portion of the lipoma, obstructive hydrocephalus with indication for a cerebrospinal fluid (CSF) diversion procedure or ventriculostomy, uncontrollable seizures.[8] When indicated the resection could be extremely difficult and potentially risky and dangerous. Is especially related with the location of the mass and because the huge adhesion with surrounding brain parenchyma, neurological and vascular structures.[9] Duane retraction syndrome (DRS), also called Stilling–Turk–Duane syndrome, is a congenital eye movement abnormality that present a variable horizontal duction deficits, with narrowing of the palpebral fissure and globe retraction on attempted abduction, occasionally accompanied by upshoot or downshoot.[10] The DRS is a cause of all forms of strabismus in 5% of the cases, it was widely described in the literature as early as the 19th century.[11,12] In 1905 Alexander Duane published a series of 54 cases with DRS, did a description of the clinical features and resume the possible etiopathogenesis and management of this pathology. With the advent and development of neuroimaging, muscle electrophysiology and genetic analysis, there has been greater understanding of this form of strabismus, now considered a congenital cranial dysinnervation disorder (CCDD), giving better insights into the management of this challenging syndrome.[13]
We describe a clinical case of a 12-year-old male child, eutocic delivery with APGAR score of 9 in the first minute and 10 at 5 minutes. Was born with a weight of 3315 kg, a height of 48 cm, and a cranial circumference of 34 cm. Blood group O RH -, with negative direct Coombs. At delivery, a dermolipoma was observed in the left eye and 2 left preauricular appendages, patent external ear pavilions. Hemifacial microstomia (Goldenhar syndrome was subsequently ruled out). No other visible morphological alterations. Considering the identified alterations, he was referred and periodically evaluated by Neonatology, Pediatrics, Ophthalmology, Otorhinolaryngology, Neurology and later by Neurosurgery. In this context, an MRI was performed, where a left intraorbital lesion with fatty content was observed adjacent to the lateral wall of the eyeball and in front of the insertion of the lateral rectus muscle. Small dermoid cyst in the right peripontine cistern, hyperintensity in T1. At one month of age, a routine check-up revealed a head circumference of 45 cm with plagiocephaly, short neck, functional limitation of the left VI PC, eyelid asymmetry, blinking with myoclonus in both eyes when looking up. Occasional episodes lasting a few seconds. The patient has been monitored and periodically evaluated in the neonatal pediatrics department; he has shown active, normal muscle tone, positive suction-search, complete bilateral moro, positive palmoplantar pressure, positive galant test. Convergent strabismus of the left eye. An electroencephalogram was also performed, which showed no abnormalities and was reported as normal for his age. To rule out organic pathology, a cardiac ultrasound was performed: normal, with no cardiac symptoms ever present. A renal ultrasound was also performed, which showed no abnormalities. A genetic study was performed, showing karyotype 46XY, normal (Figure 1).
Figure 1: Karyotype normal, with a 46 XY.
During the follow-up at 8 months of age, the laboratory tests identified a heterozygous C677T mutation (MTHFR gene) and the thyroid study was normal. A coagulation disorder was identified with a homozygous coagulation factor XII mutation.
We highlight the evaluation in the Pediatrics consultation at one year of life, in which the patient presented free crawling, begins walking, social smile, does not point with the finger. Does not close hands in the midline. Poor imitation of movements. Responds to his name. Discrete left superior orbicularis muscle asymmetry. Dermolipoma in the left eye with
paresis of the VI PC. Convergent strabismus in the left eye. Normal ENT evaluation.
An brain MRI was performed during the same period that revealed a well-defined homogenous fat density seen in the midline along the falx cerebri at the level of the vertex. It measured 2.5 x 1.5 x 4 cm in maximum AP x TR x CC [anteroposterior x transverse x craniocaudal] dimensions, likely representing quadrigeminal cistern lipoma. Left intraorbital lesion with fatty content adjacent to the lateral wall of the eyeball. Both lesions showed no changes in dimension or density compared to previous MRIs.
The child’s condition remained stable there was no headache, dizziness, abnormal movements, or seizures. In 2018 repeat brain mri and the findings are substantially similar. Brain morphology within normality for age, including ventricular size. Adequate myelination without evidence of demyelinating foci. Absence of hypoxic residues or ischemic lesions. No disorders in neuronal migration or sulcation are identified. Absence of hemorrhage or signs of intraaxial expansivity. Normal occipitocervical hinge. Distal internal carotid and basilar artery patency. At the level of the right quadrigeminal cistern present a well-defined homogenous fat density. Cerebral tonsils in correct position. At the orbital level, identified a dermolipoma in intimate contact with the nodular conjunctiva of the external face of right eye, therefore extraconal and preseptal lesion. Extrinsic ocular muscles, preserved, without being able to determine denervation phenomena, atrophy compared to the contralateral one. Optic nerves with normal characteristics in this technique (Figure 2).
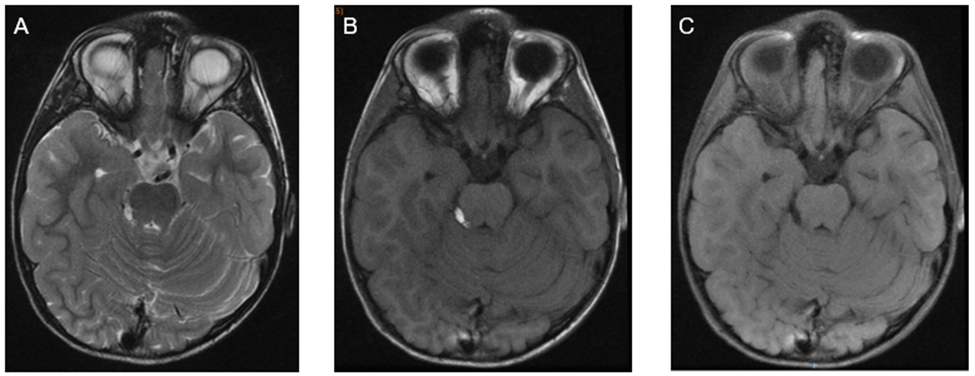
Figure 2: Brain MRI A, B, C axial slices, The images demonstrate a homogeneously oval-shaped, fat-containing suprasellar hypothalamic lesion measuring 11x 5 x 7 mm in the anterior-posterior, transverse, and craniocaudal dimensions, respectively, on the left side. The lesion is hyper intense in T1-weighted images, intermediate to hyperintense in T2-weighted images, and suppressed on fat-saturated images. No internal septation, nodularity, or calcifications are noted. lipomatous lesion in right quadrigeminal cistern 11 mm.
In the dorsal MRI, at the mid-dorsal level, presented a visible ependymal duct, greater degree of dilation, hydrosyringomyelic cavity located between T8-T10. Correctly positioned conus medullaris. Also present disc hypoplasia with congenital fusion T6-T7 and T8-T9 with remaining disc spaces with a more preserved appearance. Absence of signs of instability. No evidence of compressive pathology (Figure 3).
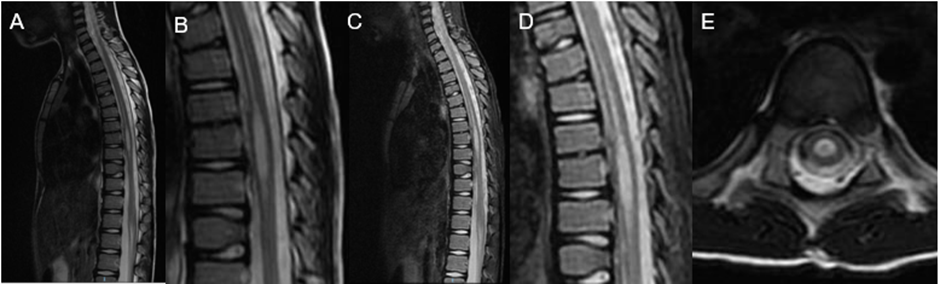
Figure 3: A, B, C, D, sagittal slices T2, E axial T2. Centromedullary syringomyelic cavity from T8 to T11, 4 x 0.4 cm
He has been referred to the rehabilitation department for presenting dorsolumbar kyphotic attitude. With the well-conducted sessions such as daily life activities and sports, he has achieved motor development identical to children of his age, fulfilling items according to his age. Although it is worth highlighting laxity in both hands, difficulty with strength and fine psychomotor skills in the hands but without signs of motor dysfunction.
In the various follow-up consultations in the Pediatrics department, normal psychomotor development was observed, and he completed schooling without problems and without dyslexia. Follow-up and evaluation with Ophthalmology showed significant astigmatism, with normal fundus and retina, normal anterior chamber.
Actually, the patient presented a good cognitive evolution, good verbal and non-verbal development, no dyslexia, great sensitivity and sense of responsibility. He is aware of his pathologies and faces them with joy, resignation, he is a fighter and an example for his family, friends and all those around him.
Below are the latest MRI images of the skull where the already known lesions are maintained without any changes in size or alterations in the different MRI weightings (Figure 4).
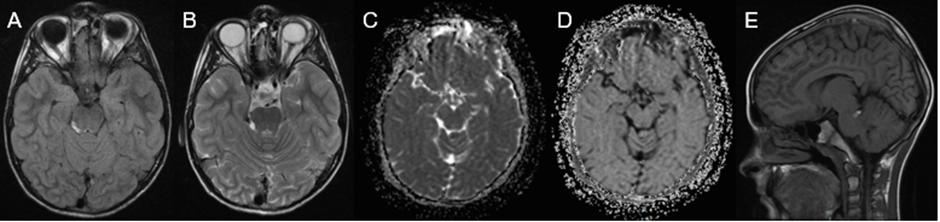
Figure 4: A, B, C, D axial slices T1, T2, ADC, eADC with lipomatous lesion in right quadrigeminal cistern. A- lipomatous lesion in anterolateral right orbit. E, T1 sagittal slice hiperintense lesion in rigth quadrigeminal cistern.
Taking into account his medical history, although he is asymptomatic, I also performed an MRI of the thoracic spine that showed normal kyphosis. Hypoplasia of the intervertebral discs T6-T7 and T8-T9. Rest of the intervertebral discs of normal height and signal intensity. Normal interfacial joints. Free conjunction foramina, of normal size and content. No rachy stenosis is observed. Centro medullary syringomyelic cavity from T8 to T11, 4 x 0.4 cm (CC x T). Regarding previous examination, a slight decrease in its maximum transverse diameter and a slight increase slight decrease in its maximum transverse diameter and a slight increase in its maximum cephalocaudal diameter stands out (previous study of 3.3 x 0.5 cm), (Figure 5). Actually, we maintain the annual follow-up with Brain and Spine MRI. Anticipate testing if the patient fell new symptoms related with the know pathologies.

Figure 5: A, B, C, sagittal slices T2, STIR, D axial T2. Centro medullary syringomyelic cavity from T8 to T11, 4 x 0.4 cm
Intracranial lipomas (IL) are an uncommon congenital pathology that resulting from abnormal differentiation of meningeal tissue during embryonic phases of development. Most IL are small, usually pea-sized, and asymptomatic.[14] The IL are rare malformations that form due to the abnormal persistence of meninx primitiva, which is the mesenchymal tissue that the meninges arise from and differentiate into adipose tissue. These lesions are most commonly idiopathic in origin, and located mainly in the interhemispheric fissure. [15, 16] The symptoms are dependent on the location of the tumors intracranially and how they affect the surrounding brain parenchyma or neurovascular structures. The most common symptoms are headaches, seizures, or vertigo. Most commonly the patients are asymptomatic, and the IL are found as an incidental finding. [17] Diagnosis based on symptoms or clinical data needs to be complemented with neuroimaging studies such as computed tomography or magnetic resonance imaging. Nonetheless, the definitive diagnosis as in all pathologies is achieved exclusively with the histological study. [18,19, 20] Frequently can be identified structural differences at the level of the cell density between benign and malignant lesions. This study propose is determine the ADC role by comprehensively evaluating DWI and histologic features of a wide variety of pathology proven lesions. The final goal of the study is identifying specifically the added value of ADC mapping to conventional 1.5 T MRI to distinguishing the lesions into benign and malignant. In some cases, these two techniques can avoid unnecessary surgical resection and help in management guide. The different conventional sequences are useful for lesion detection. However, the DWI helps to achieve the diagnosis, providing information on the grade and type of the tumor, it also allows monitoring the response to treatment. [21] The surgical approach, for this rare benign disease with frequently slow growing behavior, is generally contraindicated. However, the surgical management has an important role in certain cases, especially in cases with hydrocephalus, uncontrollable epileptic seizures, and bone involvement with cosmetic complications. If was detected seizures, anti-seizure medications are the first line of treatment. In all the cases is recommended maintain the follow up with MRI annually at least in the 5 years following the diagnosis and whenever any symptom related to the presence of the tumor occurs. [22] Duane retraction syndrome (DRS), also called Stilling–Turk–Duane syndrome, is a congenital disease that provoke a eye movement anomaly with variable horizontal duction deficits, palpebral fissure narrowing and globe retraction during adduction, occasionally occur with upshoot or downshoot. Represents 1-5% of all forms of strabismus. [23, 24, 25] In 80% are a sporadic entity, most commonly affecting females, though familial cases have also been noted in 5%–10% of cases. [26] DRS is also more commonly unilateral and affecting more frequently the left eye. [27, 28, 29]
The etiopathogenesis of this condition can be explained by a spectrum of mechanical, innervational, neurologic and genetic abnormalities occurring independently or which influence each other giving rise to patterns of clinical presentations along with a complex set of ocular and systemic anomalies. Until now various theories were proposed to explain the etiology of DRS, many authors related this pathology with mechanical anomalies, innervational anomalies, central nervous system anomalies or the role of genetics. [30] More recently in 1998 was demonstrated the absence of left sixth nerve in a case of unilateral DRS. The authors using high-resolution T1-weighted images on magnetic resonance imaging (MRI). This congenital absence of innervation to the muscles has been found to cause fibrotic changes in the extraocular muscles leading to abnormal motility in DRS, a concept which has evolved over the last decade to be known as congenital cranial dysinnervation disorder (CCDD). [31, 32] In this disease the developmental abnormalities of one or more cranial nerves cause congenital dysinnervation of the cranial muscles. This may be primary due to absence of normal innervation or secondary following aberrant innervations from other cranial nerves. This entity, CCDD, is nonprogressive and may also have associated bony abnormalities. [33]
DRS is a group of entities linked by dysinnervation leading to limited horizontal gaze and globe retraction in attempted abduction. Understanding these mechanisms can help understand the pathogenesis of the presenting features of this syndrome. Globe retraction in adduction, which is a characteristic feature of DRS, is found to be due to tight fibrotic muscles, sometimes with anomalous insertions. Usually, these changes have been observed in the horizontal rectus muscles, as is often noted while operating such patients. DRS is a spectrum of mechanical, innervational, neurologic and genetic abnormalities that influence each other giving rise to patterns of clinical presentations which can be categorized as described below.[34] Various systems of classification were proposed to understand the mechanism and presentation of DRS. Ahluwalia and modified Huber’s classification to include further subgroups in each category described by Huber. Depending upon the alignment in primary gaze, each Huber type was divided into A, B and C, indicating esotropia, exotropia and orthophoria, respectively, thus making it even more relevant clinically and surgically. [35, 36] Huber type I DRS is the most common form of DRS with an earlier presentation, while Huber type II is the least common presentation. Usually, patients with unilateral type I Duane syndrome have esotropia more frequently than exotropia, those with type II have exotropia and those with type III have esotropia and exotropia occurring equally common. Cases of bilateral DRS may have variable presentation depending upon the type of presentation in each eye. The clinical presentation and the common reasons for seeking medical attention in DRS patients include an abnormal head position of the child, one of the eyes appearing smaller than the other due to globe retraction, pseudoptosis in adduction or abnormal eye movements. DRS is present at birth and in early stages may appear only as an abduction deficit. The inelasticity and tightness develops, the globe retraction and limitation of motility may be more pronounced with time. [37] The intelligence of the patients is usually normal in DRS but intellectual disability has been reported in a few cases with borderline intelligence and cases of autism spectrum disorder associated with fetal thalidomide exposure or HOXA1-related syndromes. [38, 39] The management of DRS is a challenge, and surgeons worldwide have their own preferred practices. In general, the surgical plan and aim of strabismus surgery in DRS is usually based on the primary position deviation, the degree of abnormal head posture, the severity of globe retraction and overshoots, degree of limitation of ductions, forced duction testing (FDT), extent of field of binocular single vision. Many authors consider that DRS classification based on primary position deviation as esotropic, exotropic or orthotropic is said to be more relevant than Huber’s classification before planning surgery. The surgical approach could be individualized based on the amount of ocular deviation, abnormal head position, associated globe retraction and overshoots present by the patients. 30 Our patient present also syringomyelia, a neurological disorder in which a fluid-filled cyst (syrinx) forms within the spinal cord. Is a neurologic condition caused by the presence of a fluid-filled cavity within the spinal cord parenchyma or central canal. Is the development of a fluid-filled cyst within the spinal cord. The cyst, which is sometimes called a syrinx, can grow larger over time. The cavity can growth, compress and damage the spinal cord. [40, 41] The etiology of this conditions are related and include conditions that alter the physiologic cerebrospinal fluid (CSF) circulation dynamics. In most cases, it is secondary to spinal subarachnoid space obstruction. This pathology has several possible causes, many cases are associated with a Chiari malformation. [42] Although other causes of syringomyelia include spinal cord tumor, trauma, and post-traumatic or infectious adhesive arachnoiditis. [43, 44] Epidemiological data related with syringomyelia is limited, the prevalence of this pathology is 8.4/100,000 to 0.9/10,000 with ethnic and geographic variation. The age of the majority of the patients in the moment of diagnosis range between 20 to 50 years. [45,46] The syringomyelia may present with sensory symptoms such as pain and temperature insensitivity, it is more commonly found incidentally. The symptoms vary among individuals depending on where the syrinx forms, how large it is, and how long it extends. The symptoms develop slowly over time, worsen over many years, and may occur on one or both sides of the body. The most common symptoms are pain, progressive weakness, stiffness in the back, shoulders, neck, arms or legs, headaches, loss of sensitivity to pain or temperature, especially in the hands, numbness or tingling, loss of balance, loss of bowel and bladder control, sexual disfunction, and scoliosis may be the only symptom in children.[47] For the diagnosis and evaluation of this pathology the magnetic resonance image (MRI) with and without gadolinium contrast is the gold standard technique. The MRI present the relevant anatomy and allows accurate visualization of the syrinx in both sagittal and axial planes. The MRI permit found the location, size, extent of the syrinx cavity and the degree of cerebellar tonsillar ectopia. After diagnosis is recommended study syrinx progression over months or years to report the natural history of syringomyelia. The high use of the MRI for the evaluation of neck or back pain has led to increased detection of syringomyelia. [48] During diagnosis and follow up of this pathology we can also use Dynamic MRI or Cardiac Gated CINE-MRI Flow Study. Permit analyze CSF hydrodynamics non-invasively. It can diagnose CSF velocity/flow disturbance at the foramen magnum particularly in patients with <5mm>
We report a clinical case with uncommon pathologies, the first case report that combine a intracranial lipoma and a Duane retraction syndrome. IL are a congenital rare benign lesions that frequently present a slow growing behavior, the symptoms depend of the location of the lesion, and in many cases are asymptomatic. Actually the MRI are the gold standard image test diagnosis. The surgical management is infrequent and could result in high morbidity/mortality. The surgery should be considered when seizures are related with the tumor and not respond to medical treatment, hydrocephalus caused by the tumor and in those cases with aesthetic changes related to tumor growth. DRS consists of a complex set of ocular and systemic anomalies. It is caused by mechanical, genetic, embryologic and central nervous system anomalies occurring together or as an independent etiology. The management of DRS is a challenge, the surgical procedure must be individualized based on the amount of ocular deviation, abnormal head position, associated globe retraction and overshoots. The surgical treatment in syringomyelia cases is to correct the underlying causative pathophysiology, the treatment strategies are directed toward improving CSF flow dynamics. In the three pathologies is recommended maintain a long term follow up with MRI annually at least in the 5 years following the diagnosis and whenever any symptom related to the presence of the tumor occurs.
To the patient and her parents that gave consent for their clinical history and particularly the images to be used in this paper, and permit the scientific community to learn and know more about this uncommon pathologies.
For this type of study, formal consent is not required. All images are anonymized. Ethical approval is exempted based on the guidelines of the research center at our institution. All the procedures being performed were part of the routine care.
The author report no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
