
Case Report | DOI: https://doi.org/10.31579/2834-5142/016
1 Nephrology unit, Hospital De Clínicas, Buenos Aires, Argentina.
2 Nephrology unit, Fresenius Medical Care -Ibagué –Colombia.
3 Department of medicine, Manizales University –Colombia.
4 Hematology unit, Fluminense University -Rio de Janeiro –Brazil.
5 Department of medicine, Cooperativa University-Santa Marta-Colombia.
6 Intensive care unit, Tolima Universito –Colombia.
7 Intesivist Physician - Barranquilla – Colombia.
*Corresponding Author: José Lucas. Daza, Nephrology unit, Hospital De Clínicas, Buenos Aires, Argentina.
Citation: José Lucas. Daza, Yaroslad De La Cruz, John F. Galindo, Gerardo Gutierrez, Luis Puello., et all (2022). Dual Glomerular Lesion in Hiv Patient. International Journal of Clinical Nephrology. 4(1); DOI:10.31579/2834-5142/016
Copyright: © 2022 José Lucas. Daza. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 December 2021 | Accepted: 04 January 2022 | Published: 11 January 2022
Keywords: Covid-19; acute kidney injury; nephrology
HIV-associated nephropathy (HIVAN), the classic kidney disease associated with HIV infection, was first described in 1984 as a complication of AIDS although HIVAN may also occur in patients with less advanced HIV infection or following acute seroconversion Histologically, HIVAN is a collapsing form of focal segmental glomerulosclerosis (FSGS) accompanied by microcystic tubular dilatation and interstitial inflammation. HIV-immune complex kidney disease (HIVICK). Other immune complex diseases may also occur in HIV-infected patients, including IgA nephropathy and postinfectious glomerulonephritis, and are best diagnosed as those specific entities
The pathophysiological mechanism of HIVAN injury is mediated by direct infection of renal epithelial cells by HIV, expression of intrarenal viral genes, and dysregulation of host genes by modulating cell differentiation and the cell cycle. In contrast, kidney disease by HIV immune complexes (HIVICK) involves a different immune mechanism with antibody deposits within glomerular structures. Both entities progressively present different degrees of proteinuria and progressive decrease in the glomerular filtration rate, depending on the commitment or histology suffered by the patient.
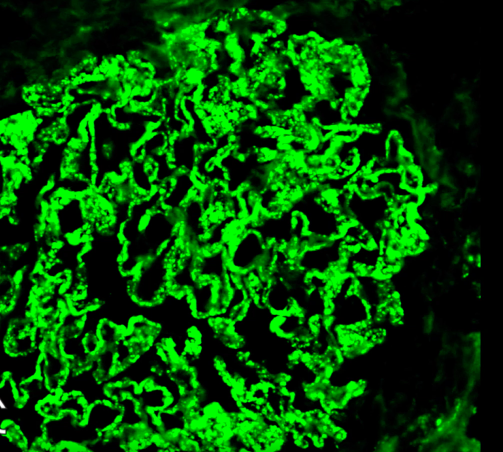
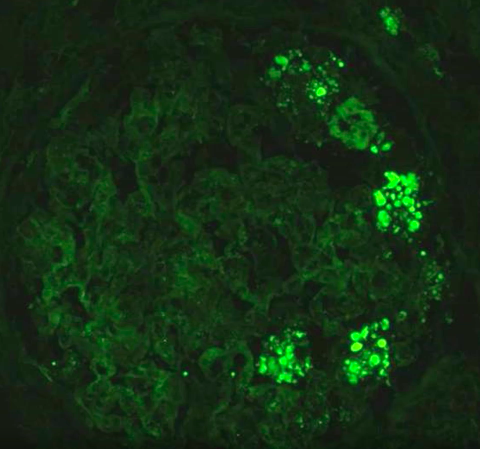
In this case reports patient with clinical picture of 3 months of evolution of temporo-spatial disorientation and alteration of the state of consciousness associated with hyperthermia. We perform neuroimaging without alterations, a lumbar punctures performed with evidence of an infectious process by coconuts + in the GRAM of the cerebrospinal fluid , normochromic normocytic anemia and renal failure , sub nephrotic proteinuria, glomerular hematuria, HIV positive, recount of normal CD4, renal biopsy with diagnosis of immune-mediated glomerulonephritis (IgG and C3), in the immunofluorescence ( HIVICK) and with membrano pattern proliferative and in two glomeruli focal segmental sclerosis collapsing variant ( HIVAN)is observed
Kidney disease is among the leading causes of morbidity and mortality in patients with human immunodeficiency (HIV) [1]. Groups of glomerular diseases that are related to HIV: podocytopathies and those mediated by immune complexes [2].
HIV-associated nephropathy (HIVAN) IS the most frequent podocytopathy and is the most important cause of end- stage renal disease is this population [3], mediated by direct infection of renal epithelial cells by HIV, expression of intrarenal viral genes, and dysregulation of host genes that govern cell differentiation and cell cycle [4].
HIV-immune complex kidney disease (HIVICK) involves a different immune mechanism with antibody deposits within glomerular structures. Both entities lead to proteinuria and progressive decrease in the glomerular filtration rate, although HIV not only has glomerular involvement but also vascular, interstitial involvement, we will focus on glomerular involvemen [5], (SEE TABLE 1)
In this paper we report a case of a Latino patient with HIV had immune-complex mediated glomerular disease (HIVICK) plus a collapsing glomerulopathy (HIVAN) with normal CD4 cell count.




It presents in the emergency department male of 72 years with behavioral alterations of 3 months of evolution, associated with hyperthermia in the last week. On physical examination he with PA 150/100 mmHg, neurologically responds to simple commands, and has disorientation in time and space. In the laboratory with Hematocrit 27%, Hemoglobin 8.7 mg/dl, white blood cells 6370 cel/ul (CD4 795 cel/ul), platelets 222000 cel /ul, ureic nitrogen 57 mg /dl, creatinine 2.03 md /dl. A simple brain CT scan is performed without alterations and lumbar puncture with normal opening pressure, cerebrospinal fluid with 120 cells/ul (70% monocities’), glucose 48 mg/dl, (glycemia 124 mg/dl) , proteins 40 mg/dl, gram with coconuts (+) , HIV rapid test (+), viral load 69,780 copies 8log 4.8), urinary sediment with density 1012mOsm/L, Ph 5, proteinuria 4+, 30-40 dysmorphic red blood cells (> 5
HIVAN/HIVICK are the most frequent forms of kidney disease directly related to HIV infection, HIVAN usually occurs in patients with advanced disease with low CD4 count, with massive proteinuria and progressive renal failure, and HIVICK are several the spectrum of diseases associated with immune complexes such as membranous nephropathy , glomerulus nephritis with proliferative membrane pattern, in this patient had coexistence of dual glomerular lesion, it is an infrequent case of two histopathological patterns of glomerulopathies in relation to HIV simultaneously in the context of a patient with recent diagnosis of retrovirus infection and normal CD4 count. In the world literature there are few reported cases of both histopathological findings together and with the characteristics of infect-immunological profile presented in our case
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
