
Research Article | DOI: https://doi.org/10.31579/2692-9406/153
1 Professor, Department of Anaesthesia and Intensive Care, Post Graduate Institute of Medical Education and Research, Chandigarh.
2 Department of Anaesthesia and Intensive Care, Post Graduate Institute of Medical Education and Research, Chandigarh.
3 Department of Anaesthesia and Intensive Care, Post Graduate Institute of Medical Education and Research, Chandigarh.
*Corresponding Author: Neerja Bharti, MD, Professor, Department of Anaesthesia and Intensive Care, Post Graduate Institute of Medical Education and Research, Chandigarh.
Citation: Neerja Bharti, Gurpreet Kaur, Dinesh Sardana, (2023), Dose Response Study of Intrathecal Dexmedetomidine as An Adjunct to Local Anaesthetic in Spinal Blockade for Lower Limb Trauma Surgeries - Randomized Controlled Trial, J. Biomedical Research and Clinical Reviews. 8(2); DOI:10.31579/2692-9406/153
Copyright: © 2023, Neerja Bharti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 May 2023 | Accepted: 18 May 2023 | Published: 25 May 2023
Keywords: adjuvants; dexmedetomidine; postoperative analgesia; spinal anesthesia; orthopedic surgery
Background: Intrathecal dexmedetomidine has been used in different doses as an adjuvant with local anesthetics to provide prolonged postoperative analgesia. This prospective randomized dose response study was conducted to find out the safe and effective dose of intrathecal dexmedetomidine to provide good quality of perioperative analgesia. Methods: Eighty adult patients of lower limb trauma undergoing orthopedic surgery were randomly allocated into four groups. Group B received 0.5% hyperbaric bupivacaine 15 mg with 0.5 ml normal saline while group D3, D5 and D7 received dexmedetomidine 3 µg, 5 µg and 7 µg respectively added to 15 mg 0.5% hyperbaric bupivacaine (total volume 3.5 ml in each group) intrathecally during subarachnoid block. The patients were monitored for onset and duration of block, the time to first rescue analgesia, postoperative pain scores, 24-hour analgesic consumption, hemodynamic parameters, sedation level, and adverse effects. Results: Intrathecal dexmedetomidine significantly reduced the requirement of postoperative analgesia and prolonged the analgesic duration in all three doses (p<0.0001). The duration of postoperative analgesia was significantly longer in D7 group as compared to D3 and D5 groups (p<0.0001). Postoperative pain scores were less in patients receiving dexmedetomidine 5 µg and 7 µg as compared to the control group (p<0.0001). Intrathecal dexmedetomidine significantly shorten the onset times and increased regression times of the sensory and motor blockade in dose dependent manner. The incidence of hypotension was comparable among groups. Dexmedetomidine produced arousable sedation during perioperative period in all 3 doses. No significant adverse effects were reported in any group of patients. Conclusion: Dexmedetomidine produced dose dependent prolongation of spinal blockade and postoperative analgesia in 3, 5 and 7 µg doses as an adjuvant with intrathecal bupivacaine. Intrathecal dexmedetomidine 7 µg can be used safely to provide prolonged postoperative analgesia for lower limb orthopedic procedures in healthy adult patients.
Perioperative pain management is a major challenge for anesthesiologists to improve functional recovery after orthopedic surgeries. There has been a constant struggle to bring out the best possible analgesic technique with least side effects. The subarachnoid block is commonly used for lower limb procedures because of its rapid onset of action and cost-effectiveness. Various adjuvants like opioids, midazolam, ketamine and neostigmine have been added to intrathecal local anesthetics for increasing the duration of post-operative analgesia [1]. However, there use is limited by various adverse effects including pruritus, respiratory depression, urinary retention, post-operative nausea and vomiting.
Dexmedetomidine, a highly selective α2-adrenergic agonist, is rapidly emerging as the choice of additive to spinal anaesthesia in view of its property to provide analgesia without respiratory depression and other opioid related adverse effects [2,3]. In various studies, dexmedetomidine has been found to be more efficacious than fentanyl, morphine and clonidine when used intrathecally with local anesthetics [4-7]. Intrathecal dexmedetomidine has been used in 3, 5, 10 and 15 µg doses in different studies to enhance postoperative analgesia [8-10]. Though increasing the dose of intrathecal dexmedetomidine from 3 to 15 μg prolonged the duration of postoperative analgesia, the risk of adverse effects has also been increased at the same time [11-13]. Hence, there is no clear consensus on the dose of dexmedetomidine to be used with local anesthetics in neuraxial blockade to avoid side effects while ensuring pain free perioperative period. Therefore, this prospective randomized double-blind study was conducted to determine the best effective dose of dexmedetomidine as an adjuvant to intrathecal bupivacaine for providing prolonged and safe postoperative analgesia in patients undergoing lower limb orthopedic surgery.
This prospective randomized double-blinded study was conducted after approved from “Institutional Ethical Committee” and written informed consent from all the participants. We enrolled 80 adult trauma patients, aged 18-65 years, of American Society of Anesthesiologists physical Status I and II undergoing below hip lower limb orthopedic procedures under spinal anesthesia. Patients with history of spine surgery or infection at the site of lumbar puncture, having neurological and psychiatric disturbances, coagulation disorders and those on beta blockers, calcium channel blockers or α2-agonists were excluded. Patients taking opioids or on long term analgesics were also excluded.
The patients were randomly allocated into four groups using computer generated randomization sequence. Group B patients received 0.5% hyperbaric bupivacaine 15 mg with 0.5 ml normal saline while group D3, D5 and D7 patients received dexmedetomidine 3 µg, 5 µg and 7 µg respectively (Dexmedetomidine injection 100 µg/ml) added to 15 mg 0.5% hyperbaric bupivacaine (total volume 3.5 ml in each group) intrathecally during subarachnoid block. The desired dose of dexmedetomidine was drawn up using 1 ml Tuberculin syringe, graduated, 0.01 ml and then diluted with normal saline to 0.5 ml.
Patients were kept fasting for 8 h before procedure and received alprazolam 0.25 mg the night before surgery. The subarachnoid block was performed under all aseptic precautions, in the sitting position at L3-4 or L4-5 interspace using 26-gauge Quincke needle and 3.5 ml drug was administered after aspiration according to the group allocation. The drug solutions were prepared under sterile precautions by an anesthesiologist not involved in further management of the patient. The anesthesiologist who performed the subarachnoid block and monitored the patients during intraoperative and postoperative period was blinded to the group allocation.
All patients received 500 ml normal saline before administration of block followed by 6 ml/kg/hr infusion. A standardized monitoring of ECG, blood pressure (every 5 min), respiration and oxygen saturation was performed. The patients were placed in supine position after block and oxygen was supplemented with face mask.
The level of sensory block was assessed with cold swab every 2 min after intrathecal injection till T10 dermatomal level and every 5 min thereafter until maximum level of sensory block level stabilized. The motor block was assessed using modified Bromage scale (0-3, 0=no motor weakness, 1=inability to raise extended leg, 2=inability to flex knee, 3=inability to flex ankle) at the same time intervals. The time to block T10 sensory level and Bromage scale 3 was recorded (onset times). The duration of surgery, intraoperative blood loss, total requirement of IV fluid and blood transfusion was noted. The regression of sensory and motor block was assessed at every 30 min interval. Intraoperative hypotension, bradycardia or any other complications were recorded and managed accordingly. The hypotension is defined as a mean arterial pressure <60>25
Total 80 patients (20 patient in each group) were recruited during 18 months period; all received intervention and completed the follow up. Demographic characteristics such as age, weight, height, gender, ASA physical status of the patients and the duration of surgery were comparable among groups (table 1).
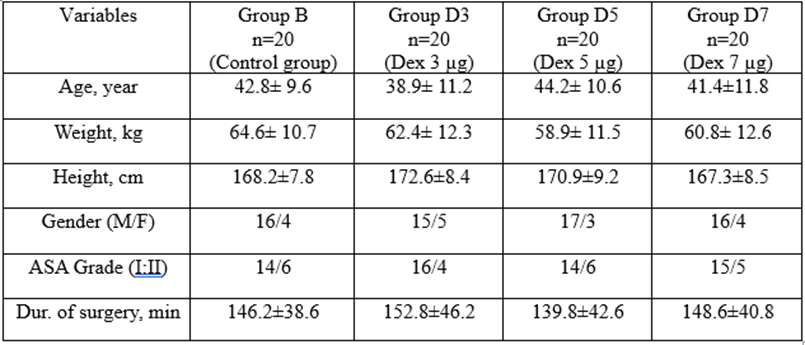
Table 1: Demographic Data
Data presented as mean ± SD or numbers of patient The surgical procedures included in the study were mainly below hip lower limb surgeries, like fixation of fracture femur, tibia or both leg bones, and comparable in all the groups. The onset times of sensory and motor blockade were significantly shorter in group D3, D5 and D7 as compared to group B. The difference was also significant between group D3 and D7 (p,0.001). The duration of sensory and motor block was significantly longer in all 3 dexmedetomidine groups as compared to the control group. The difference was also significant between group D3 and D5, and D5 and D7 for sensory block. However, there was no significant difference between group D5 and D7 for duration of motor block (table 2).
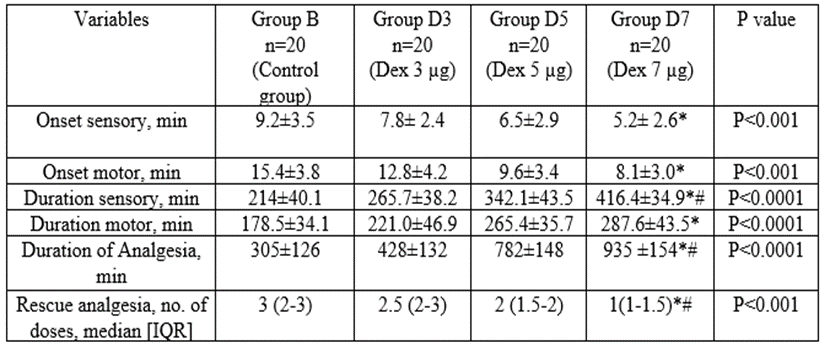
Data presented as mean ± SD or IQR, *p<0>
Table 2: Block characteristics and postoperative analgesia
Intrathecal dexmedetomidine significantly prolonged the time to first rescue analgesia in dose dependent manner with maximum increase was observed in group D7 (table 2). The duration of postoperative analgesia was about 18 hours in this group, and 30% patients did not require any rescue analgesia during 24 postoperative hours. The requirement of rescue analgesia was significantly higher in group B patients (P<0>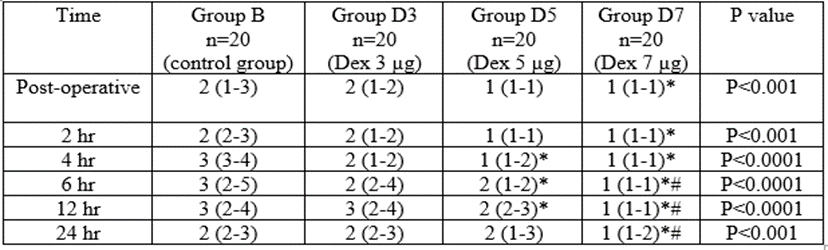
Table 3: Postoperative pain scores
Data presented as median (IQR), *p<0>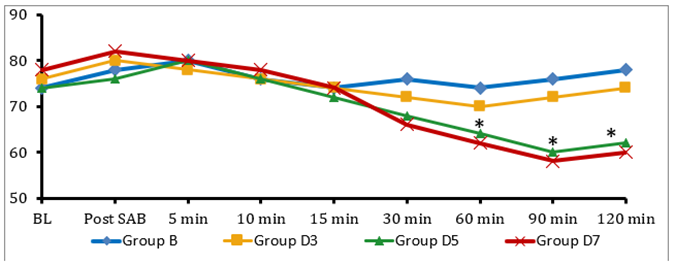
p<0>
Figure 1: Intraoperative heart rate changes among groups
The heart rate was lower in group D5 and D7 as compared to group B and D3, 30 min after spinal anesthesia (figure 2).
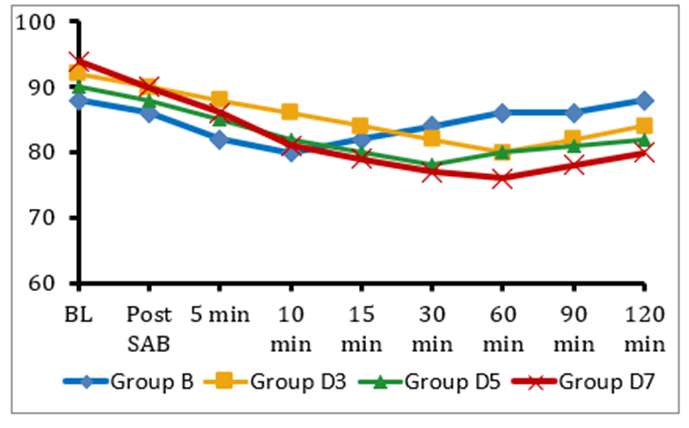
Figure 2: Intraoperative blood pressure (MAP) changes among groups
However, none of the patients had bradycardia (HR<40>
The patients receiving dexmedetomidine had mild sedation during intraoperative period and immediate postoperative period. The average post-operative sedation scores were 1-2 in most of the patients and none of the patients had sedation scores >3 in either group at any point of time (table 4).
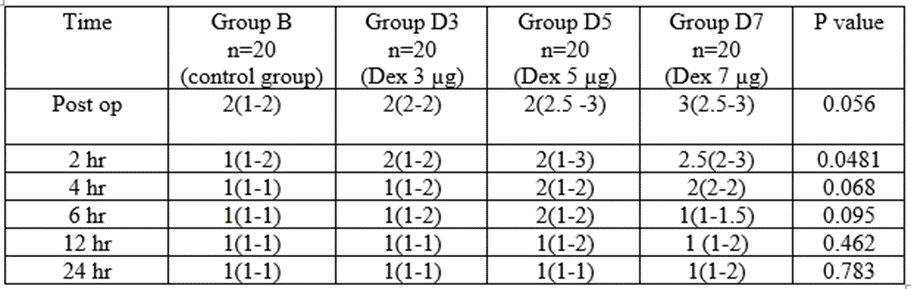
Table 4: Postoperative sedation level
Data presented as median (IQR) Six patients in group B and 2 patients in group D3 had shivering. Three patients in control group and one patient in D3 and D5 group complained of postoperative nausea and vomiting. No neurological adverse effects were observed in any group of patients.
Dexmedetomidine is under evaluation as a neuraxial adjuvant due to its various beneficial effects with lesser side effects. Intrathecal dexmedetomidine produces synergistic effect with local anesthetics and prolongs analgesia by binding and depressing the release of presynaptic C-fiber neurotransmitters and also by hyperpolarization of post-synaptic dorsal horn neurons (14). This anti-nociceptive effect may explain the prolongation of the sensory block while prolongation of motor block may be due to the binding of the drug to motor neurons in the dorsal horn.
In the present study, intrathecal dexmedetomidine significantly prolonged analgesic duration and decreased postoperative pain intensity in all three doses. The effect appears to be dose dependent and more pronounced with the dose of 7 µg. Additionally, neuraxial dexmedetomidine was associated with beneficial alterations in the sensory and motor block characteristics as well as postoperative sedation scores. The incidence of hypotension and bradycardia was not significant with dexmedetomidine being used up to 7 μg doses intrathecally.
In previous studies intrathecal dexmedetomidine has been used in variable doses ranging from 1.5 to 20 μg. Elhamid and Ali [10] compared 1.5 μg with 3 μg and 5 μg doses of dexmedetomidine and find out that 3 μg is the least effective dose to be used in spinal anesthesia. In a study comparing the analgesic efficacy of 3 and 5 μg intrathecal dexmedetomidine in orthopedic patients undergoing lower limb surgeries, the duration of postoperative analgesia was significantly (p,0.001) prolonged in 5 μg dexmedetomidine group as compared to 3 μg group without any increase in adverse effects [15]. In another study, intrathecal dexmedetomidine 5 μg potentiated hyperbaric bupivacaine antinociception by 31% in spinal anaesthesia for patients undergoing cesarean section without significant untoward effects [3]. In a comparative study, 5 μg intrathecal dexmedetomidine as an adjunct to 0.5% bupivacaine produced longer duration of postoperative analgesia than 25 μg fentanyl for lower limb surgical procedures [4]. However, in all these studies, the maximum duration of postoperative analgesia in dexmedetomidine group was around 5-6 hr. Naithani et al [16] reported that 5 μg intrathecal dexmedetomidine did not show much promise in reduction of required analgesic supplementation after surgery.
Intrathecal dexmedetomidine has also been tried in higher doses (up to 15-20 μg) with the main goal of enhancing postoperative analgesia. Though, dose dependent increase in analgesic duration was observed, the incidence of hypotension and bradycardia was also increased [11,12]. Bhure et al [13] compared the effect of 10 and 15 μg intrathecal dexmedetomidine in patients undergoing abdominal hysterectomy under spinal anesthesia and reported dose related increase in hypotension and bradycardia. Elhadary et al [17] also reported high incidence of hypotension in patients receiving 10 μg dexmedetomidine with 0.5% intrathecal bupivacaine for lumber spine surgery. A meta-analysis [12] involving 16 RCTs and 1092 participants reported significantly decreased postoperative pain intensity (P,0.00001) and prolonged analgesic duration (WMD, 6.93 hours; 95% CI, 5.23 to 8.62; P,0.00001) in patients receiving intrathecal dexmedetomidine with increased the risk of bradycardia (OR, 2.68; 95% CI, 1.18 to 6.10; P = 0.02) when used in higher doses (≥10 µg). In the present study administration of intrathecal dexmedetomidine in doses of 7 µg provided around 18 hours of postoperative analgesia without compromising hemodynamic parameters. The longer duration of sensory and motor blockade resulted in better anesthesia and analgesia during intraoperative period. The maximum duration of motor blockade was around 4 hours since administration of the drug which did not influence recovery and rehabilitation protocol.
Intrathecal dexmedetomidine reduces perioperative shivering after neuraxial blockade by regulating the shivering threshold and reducing the contraction of vessels [18]. It suppresses the neuronal conductance, thus decreasing the central thermosensitivity. In a recent meta-analysis, Wang et al [19] demonstrated that intrathecal dexmedetomidine significantly reduces the incidence of intraoperative shivering under spinal anesthesia. We also found significantly reduced incidence of shivering in all dexmedetomidine groups.
Dexmedetomidine usually produces ‘arousable sedation’ without any respiratory depression which may be beneficial for the patient to alleviate anxiety during perioperative period. None of our patient had deep sedation, hypoxia or respiratory depression. Intrathecal dexmedetomidine has been found to be safe when used with local anesthetics in doses of up to 0.2–1 μg/kg [20]. We did not find any neurological adverse effect in any group of patients. The main limitation of this study was that we enrolled healthy adult patients, therefore our results cannot be generalized for elderly patients with cardiovascular morbidities.
In conclusion, addition of dexmedetomidine to intrathecal hyperbaric bupivacaine enhances the quality and onset of subarachnoid block and increases postoperative analgesia in dose dependent manner. Intrathecal dexmedetomidine in doses of 7 μg provided prolonged postoperative analgesia with beneficial alterations in the sensory and motor block characteristics. The incidence of hypotension was not significant. The patients’ had only mild sedation during immediate postoperative period, which did not affect our accelerated rehabilitation protocol, even the patients were more comfortable during physiotherapy due to good pain relief. Therefore, dexmedetomidine can be safely used in 7 μg doses as an adjunct to intrathecal bupivacaine for getting prolonged postoperative analgesia. However, it should be used cautiously in patients with cardiac problems like conduction defects or bradyarrhythmia. Also care should be taken while using this drug dose in high risk and elderly group of patients.
Source of funding and potential conflicts of interest
Authors did not receive any funding from any agency or elsewhere for the study. None of the author had any conflict of interest.
Financial Disclosures – None
Conflict of interest – None
This clinical trial is presented at the National conference of Indian Society of Anesthesiologists.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
