
Mini Review | DOI: https://doi.org/10.31579/2692-9392/086
1 Travios Air Force Base, CA; David Grant Medical Center, Department of Internal Medicine.
2 Keesler Air Force Base, MS; Keesler Medical Center, Department of Internal Medicine.
3 Keesler Air Force Base, MS; Keesler Medical Center, Department of Internal Medicine, Division of Endocrinology.
*Corresponding Author: Essien Francis, Travios Air Force Base, CA; David Grant Medical Center, Department of Internal Medicine.
Citation: Essien Francis, Jacocks Charles, Elkins Blake, Tate Joshua. (2021) Does Marine Lenhart Syndrome really exist?. Archives of Medical Case Reports and Case Study, 4(5); DOI:10.31579/2692-9392/086
Copyright: © 2021 Essien Francis, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 September 2021 | Accepted: 20 October 2021 | Published: 25 October 2021
Keywords: marine lenhart syndrome (mls); hyperthyroidism; radioiodine therapy; autoantibodies; graves’disease
Primary hyperthyroidism is the result of overproduction of thyroid hormone resulting in the classic symptoms of tachycardia, weight loss, diaphoresis, and hyperdefecation. There are multiple common causes to include Graves’ disease, toxic multinodular goiter, and solitary toxic adenomas. Marine Lenhart Syndrome (MLS) is a rare cause of hyperthyroidism, caused by a coexistence of constitutively active thyroid nodules and Graves’ disease. In the original document of Marine and Lenhart, there is no distinction made between the autoimmune phenomenon of Graves’ disease and the solitary toxic nodule of Plummer’s disease. Rather they are both considered to be the manifestation of the same disease. However, in the current era of radionuclide technology, a clear distinction of MLS can be seen with diffuse uptake in the thyroid gland and focused enhancement in the toxic nodules. Therefore what was previously described as one entity is now distinct as Graves’ disease and Plummer’s disease. It is also becoming increasingly clear within the literature that there is also a new phenomenon of post-radioiodine immunogenic hyperthyroidism in patients with toxic nodules and elevated autoantibodies. Therefore in order to properly treat and manage patients, a new definition of MLS may need to be proposed.
The term Marine Lenhart syndrome (MLS) has been assigned to this presentation with the coexistence of Graves’ disease and toxic adenomas and has become more frequently recognized within the literature [1]. However the text by Marine in 1940 failed to appropriately distinguish these two conditions noting toxic adenoma and immunogenic goiter as one condition [1]. The syndrome as described in 1972 by David Charkes [2] based off the original observations of Marine and Lenhart [3] was defined as patients with Graves’ disease and toxic adenomas that exhibit increased radioiodine uptake with TSH stimulation, appear hypofunctioning in relation to extranodular tissue on RAIU and scan, are poorly responsive to RAI ablation, and exhibit increased radioiodine uptake after RAI ablation therapy [3]. Thus, one of the key distinctions of the toxic adenomas of MLS compared to those autonomous nodules found in Plummer’s disease was their TSH dependence. A recent literature review in 2011 by Biersack suggested that MLS may be a conjoined syndrome; the classical Graves’ disease/toxic adenoma v Graves’ disease post RAI ablation with autonomously functioning thyroid nodules [1]. Examination of the previous definition of toxic adenomas by Plummer defines hyperthyroidism as a disease caused by two separate entities (Toxic adenoma and exophthalmic goiter) [1]. Thus the original term may not apply to what we now know to be two separate diseases and the medical literature needs to be updated to reflect the origin of the joint presentation.
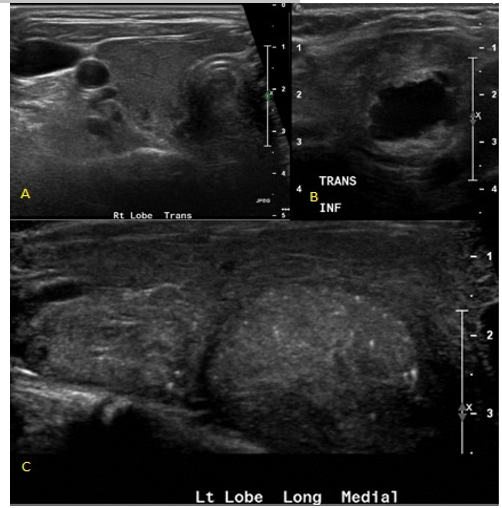
The prevalence of this syndrome has been reported to be between 2.7-4.1% of hyperthyroidism diagnoses [2], though is likely an under recognized cause of hyperthyroidism. Over the last decade there have been multiple case reports published within the literature of the manifestation of autoimmune induced hyperthyroidism following radioiodine therapy in patients with solitary toxic adenomas [1]. Thyrotoxicosis is caused by excess thyroid hormone production which can present with associated clinical findings such as tachycardia, tremor, heat intolerance, hyperdefecation, and weight loss. [2] Laboratory evaluation is typically notable for a low TSH and an elevated FT4. [2] Primary hyperthyroidism is most commonly due to Graves’ disease, accounting for 60-80% of hyperthyroid cases [1,2]. Graves’ disease is characterized by serum antibodies against TSH receptors in correspondence with T cell mediated immunity. Other causes such as Toxic adenomas or toxic multinodular goiters, also known as Plummer’s disease, are a result of several somatic point mutations in the third trans-membrane loop of the TSH receptor leading to autonomous function in absence of TSH [3]. The presence of thyroid nodules coincide with Graves’ disease in 25-30% of patients [2]. Though both disease processes result in thyrotoxicosis, their mechanism of actions are distinct (Figure 1-3 indicate a classical diagnostic image of MLS on both US and RAIU).


The incidence is especially high in those patients with pre-existing autoantibodies which is not unusual [2]. Due to the clonal origin of toxic nodules, activating thyrotropin receptor mutations can be present and amplify the activity of the nodule which leads to increased risk of “post-radioiodine immunogenic hyperthyroidism” [3,4]. However, manifestation of this disorder does not constitute the patient as having MLS when examined from the historical definition established by David Marine and C.H. Lenhart in 1911 [1,2]. Hence there remains controversy regarding formal diagnosis due to variations in imaging techniques, presentation, and onset [5,6]. Thus the definition and diagnostic criteria for Marine Lenhart Syndrome have subsequently undergone multiple revisions.
Recently documented cases of MLS include cases of coexisting Graves’ disease and hyperfunctioning nodules at the time of diagnosis [7-10], cases of Graves’ disease with “cold” nodules at the time of diagnosis that then later were confirmed as hyperfunctioning [11], and cases of development of toxic adenomas years after successful treatment of Graves’ disease [12-13]. This highlights the need for a unified definition of MLS, which was proposed by Neuman et al [7]. These proposed diagnostic criteria included confirmed hyperthyroidism based on thyroid function tests with positive thyroid autoantibodies consistent with Graves’ disease, RAIU scan revealing hyperfunctioning nodules that correspond to nodules seen on ultrasound on a background of diffusely increased radioiodine uptake, and confirmation of the presence of a follicular adenoma or hyperplastic lesion on pathologic analysis [8]. Pathologic analysis is important as there have been cases reported in the literature thus far of MLS patients with the additional finding of papillary thyroid carcinoma identified in an associated nodule with the most recent being published by Mehmet et al of a unique case of papillary thyroid carcinoma in a hyper functioning nodule [14]. This definition also encouraged a transition from using the term “autonomous” nodules to describing them as functional nodules to include the subset of MLS cases with apparent TSH dependence of the associated nodules. In fact, prior proposed definitions included the requirement for the associated nodules to demonstrate TSH dependence [15]. This currently proposed diagnostic criteria allows for inclusion of the multiple identified variants of MLS to include this unique case of nodules that appeared cold on initial RAIU scan but were later confirmed as hyperfunctioning nodules on subsequent scans after completion of RAI ablation without evidence of return to a chemically euthyroid state.
Management of MLS relies on radioactive treatment or surgery with latter being preferred in the case of malignancy, large or symptomatic goiters, moderate to severe orbitopathy and patient preference [8]. Thionamide therapy can be used in select patients, such as those with severe hyperthyroidism or advanced age, to achieve euthyroidism prior to definitive therapy realizing that, although uncommon, hepatotoxicity may occur [8]. Damle et al note that the amount of radioiodine required to relieve the hyperthyroidism in these patients is greater than the corresponding mean, median or mode dose for diffuse toxic goiter thought to be a result of the large size as well as the radio-resistance of the goiters in this disease [16].
Conclusion:
Marine Lenhart Syndrome remains a rare and poorly defined entity that should be considered different both diagnostically and therapeutically from any etiology of thyrotoxicosis in isolation. A broader definition and increased awareness is needed to allow for better understanding and improved treatment guidelines for this syndrome.
All authors discussed the results and contributed to the final manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
