
Research article | DOI: https://doi.org/10.31579/2694-0248/026
University Hospitals Cleveland Medical Center Case Western Reserve University School of Medicine Department of Orthopaedic Trauma Surgery, Cleveland, Ohio 11100 Euclid Ave Cleveland, Ohio 44106.
*Corresponding Author: Kathryn B. Metcalf, University Hospitals Cleveland Medical Center Case Western Reserve University School of Medicine Department of Orthopedic Trauma Surgery, Cleveland, Ohio 11100 Euclid Ave Cleveland, Ohio 44106.
Citation: Kathryn B. Metcalf., Jerry Y. Du., Corina C. Brown., Robert J. Wetzel., John K. Sontich, et al., (2022). Does Aspirin Provide Adequate Chemoprophylaxis for Venous Thromboembolic Events in Operative Pelvic and Acetabular fractures?. J. Clinical Orthopedics and Trauma Care, 4(3); DOI:10.31579/2694-0248/026
Copyright: © 2022 Kathryn B. Metcalf, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 January 2022 | Accepted: 31 January 2022 | Published: 04 February 2022
Keywords: venous thromboembolism; pelvic acetabular
Pelvic and acetabular fractures often result from high-energy mechanisms and represent unique treatment challenges. These fractures commonly occur with concomitant polytraumatic injuries and in the setting of significant medical comorbidities. Pelvic-acetabular trauma injuries are complex, frequently require surgical intervention, and carry a high risk of complications with sequelae leading to poor patient outcomes and large economic health-care burdens.
Pelvic and acetabular fractures often result from high-energy mechanisms and represent unique treatment challenges. These fractures commonly occur with concomitant polytraumatic injuries and in the setting of significant medical comorbidities. Pelvic-acetabular trauma injuries are complex, frequently require surgical intervention, and carry a high risk of complications with sequelae leading to poor patient outcomes and large economic health-care burdens. [1,2]
Development of a venous thromboembolism (VTE) following surgical fixation of pelvic and acetabular fractures is a serious and sometimes life-threatening complication. Previous studies of these complicated injuries have elucidated independent risk factors that predispose the patient to increased risk of PE and deep vein thrombosis (DVT) such as age, associated injuries, injury severity, and time to surgery. [3-6] Additionally, VTE events are associated with significant economic implications. One recent study in hip fracture patients demonstrated that VTE events were an independent reason for a 2-fold increase hospital length of stay and cost. [7] With rates of VTE ranging from 10-30%, coupled with a small but significant rate of pulmonary embolism (PE) in pelvic and acetabular fractures, prevention strategies are critical. [3-5,8,9] In fact, the risk of post-operative VTE is even greater in those fracture patients who receive no chemoprophylactic treatment, with reported rates as high as 40-68%.[10-13]
Although VTE is a known complication, there is limited data and no consensus on optimal thromboprophylactic agents and algorithms following operative fixation of pelvic and acetabular fractures. [8,14,15] There is high variability among different institutions. It is often debated if aspirin is an effective anticoagulation agent that provides adequate thromboprophylaxis in the setting of these complex injuries. The different mechanisms of action of agents play a role in this controversy of optimal thromboprophylaxis. Where aspirin acts via anti-platelet aggregation, the more traditionally used agents, enoxaparin and heparin, activate and accelerate antithrombin III (AT), inactivating thrombin and factor Xa. Although a multitude of anticoagulants are used in the prevention of VTE, the associated risk of bleeding or hematoma development is another important consideration in choice of thromboprophylactic agent. Despite the extensive reports on the effectiveness of various anticoagulants in total joint arthroplasty literature, [16-19] very little data exists regarding these thromboprophylactic medications in the setting of fracture patients, particularly pelvic and acetabular fractures. In fact, to the author’s knowledge no studies evaluating the efficacy of aspirin compared to enoxaparin or heparin in preventing VTE in these complicated injuries is described in the literature.
The objective of this study is to evaluate the efficacy of aspirin in prevention of VTE, including both DVT and PE, compared to the short-acting injectable anticoagulants, enoxaparin and heparin, following operative fixation of pelvic and acetabular fractures. A secondary aim was to evaluate the incidence of hematoma formation between anticoagulants. We anticipated that aspirin would be an efficacious VTE prophylaxis agent and have a lower rate of hematoma development compared to other agents.
After institutional review board (IRB) approval, a retrospective chart review of patients who sustained pelvic ring and acetabular fractures treated with operative fixation was performed. Current Procedural Terminology (CPT) codes identified 163 pelvic or acetabular fractures managed operatively between 2015-2020 at our level 1 trauma center. Patients were included if the were ³18 years of age, received aspirin, enoxaparin, or heparin as their primary anticoagulant, and had a minimum of 6 weeks post operative follow up, for injury or surgically related VTE events occur within a 6 week threshold, as nearly all post-operative VTE occur early within this timeframe. [20,21] Patients were excluded if they were <18>
Three fellowship-trained traumatologists treated all fractures. Surgical approach was dictated by fracture pattern and surgeon preference. The primary team determined treatment with aspirin, enoxaparin, or heparin. Patient demographics, medical comorbidities, and post-operative weight bearing status were accounted for across groups and normalized in a multivariate analysis.
The primary outcome measures were development of DVT or PE within a 6-week post-operative period. Hematoma development was considered a secondary outcome. Hematoma formation was defined by evidence on computed tomography (CT) and a drop in hemoglobin. Patients were treated with aspirin 81 milligrams (mg) twice a day, enoxaparin 40mg daily, or 5,000 units heparin twice a day. Mechanical prophylaxis of ambulation and sequential compressive devices (SCDs) were used in all patients. The rate of VTE and hematoma formation was compared between patients receiving aspirin and short-acting injectables, enoxaparin and heparin. Incidence of VTE and post-operative hematoma was evaluated between these groups.
Other variables reported to affect development of VTE were collected. Age, gender, time to surgery, type of anticoagulant, weight bearing status, past medical history including diabetes mellitus (DM), hypertension (HTN), chronic kidney disease (CKD), coronary artery disease (CAD), body mass index (BMI) smoking status, previous history of DVT, head trauma were assessed as potential risk factors of VTE. Trauma scores such as abbreviated injury scale (AIS) and injury severity scale (ISS), intensive care unit (ICU) length of stay (LOS), hospital LOS, and ventilator time were also assessed as potential confounders. Additionally, in this study both posterior (Kocher-Langerbeck) and anterior (anterior intrapelvic, Pfannenstiel, or ilio-inguinal) approaches were used and evaluated as confounding variables.
Statistical Analysis
Categorical variables are expressed as percentages and continuous variables are expressed as mean ± standard deviation. Continuous variables were found to not be normally distributed by Kolmogorov-Smimov tests. Univariate analysis comparing incidence of confounding variables and complications was performed using Mann-Whitney U test or chi-squared/fisher’s exact tests as appropriate.
Multivariate binary logistic regression models were created for complications that were significantly different based on surgical approach on univariate analysis. Confounding variables with p<0 An a=0.05>
There were 144 pelvic and acetabular fractures that met inclusion criteria. Mean age was 42.2 ± 17.1 years. There were 95 males (66.0%) and 49 females (34.0%). There were 6 patients (4.2%) that developed DVT and 5 patients (3.5%) that developed PE. Two patients developed both (1.4%).
There were 54 patients treated with aspirin (37.5%) and 90 patients treated with heparin or enoxaparin (62.5%). On univariate analysis of complications, there was a significantly lower incidence of hematoma formation in the aspirin cohort (n=3, 5.6% vs. n=19, 21.1%, p =0.015) (Table 1).
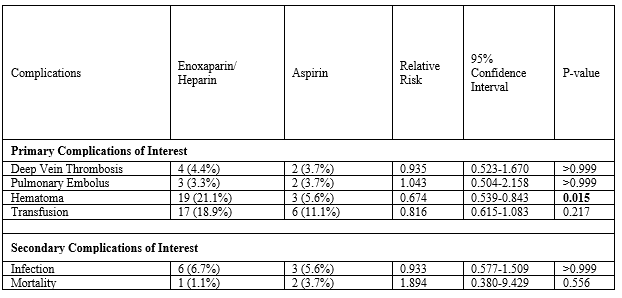
There were no differences in incidence of DVT, PE, or transfusion between cohorts. Similarly, there were no differences in the incidences of infection or mortality.
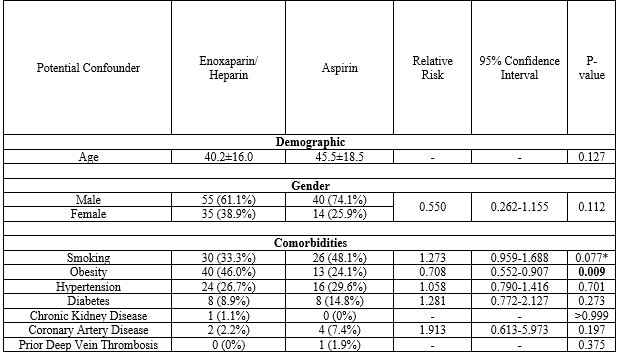
On univariate assessment of potential demographic and comorbidity confounders, the aspirin cohort was found to have a lower incidence of obesity (n=13, 24.1% vs. n=40, 46%, p=0.009) (Table 2).
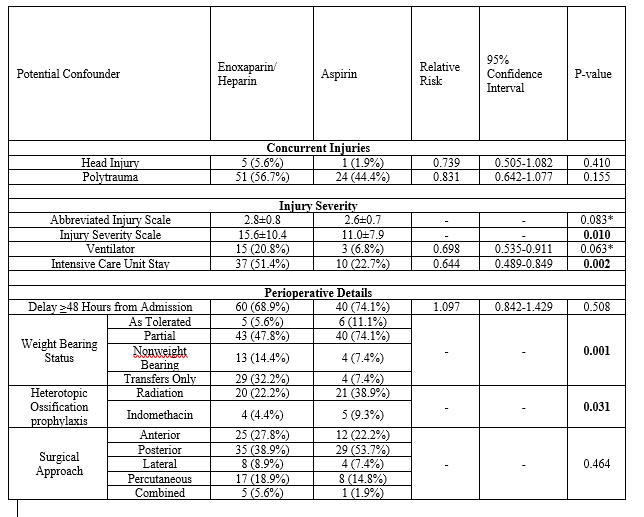
On univariate analysis of potential injury and perioperative confounders, the aspirin cohort was found to have lower ISS (11.0±7.9 vs. 15.6±10.4, p=0.010), lower incidence of ICU stay (n=10, 22.7% vs. n=37, 51.4%, p=0.002), less weight bearing restrictions (p=0.001), and received more heterotopic ossification prophylaxis (p=0.031) (Table 3). Furthermore, there was no difference in rate of DVT or PE based on an anterior or posterior approach (Table 3).
On multivariate analysis of major complications, accounting for the confounding variables found on univariate analysis, there were no significant differences incidence of VTE between aspirin and enoxaparin/heparin cohorts (Table 4).

However, aspirin trended on significance as protective against post-operative hematoma formation (adjusted odds ratio [aOR]: 0.687, 95% Confidence Interval [CI]: 0.015-1.315, [p=0.085]).
Several strategies exist to prevent venous thromboembolism (VTE) in operative pelvic and acetabular fractures, however the current literature lacks consensus on optimal thromboprophylaxis, particularly on the use of aspirin compared to other anticoagulant agents. This study suggests that there is no significant difference in the rate of VTE with aspirin compared to short-acting injectables enoxaparin and heparin and there is a trend towards a lower rate of hematoma associated with the use of aspirin.
Development of postoperative hematoma has been associated with an increased rate of surgical site infection (SSI). [22] Often patients suffering from pelvic trauma are polytraumatized patients and at high risk for complications. The reported rate of surgical site infections occur following operative fixation of pelvic and acetabular fractures is 5-8%.[23,24] The ability to limit infection and recognizing factors that may be protective in these patients is critical since infection and can greatly hinder the recovery of patients and add an unprecedented burden to the patient and the medical system.
Many patients with pelvic and acetabular fractures undergo a long stay in an ICU, are immobilized with weight bearing restrictions and have high ISS scores. Previous studies demonstrate that these factors are associated with increased development of VTE. [6,25] In this study these variables, while noted to be lower in the aspirin cohort, were controlled for in the multivariate analysis to eliminate their confounding effect. Thus, there was no evidence to indicate that aspirin was inferior to enoxaparin or heparin. This study suggests that aspirin provides adequate VTE chemoprophylaxis following operative fixation of pelvic and acetabular fractures.
In patients with pelvic and acetabular fracture, previous studies have noted that early initiation of VTE chemoprophylaxis is a significant preventative measure, [25] but its use must be balanced with the risk for bleeding and development of post-operative hematoma. With aspirin trending towards significance as protective against hematoma, this may represent a favorable option in the appropriate patients.
Additionally, there was no significant association in the risk of VTE events and the approach utilized for the pelvis or acetabulum fractures. We anticipated that the anterior approach would be a risk factor for VTE events due to mobilization and direct manipulation of great vessels that is often required. We theorized that there could be a potential risk that this could increased turbulence and thus increase the risk of a VTE event. However, this was not demonstrated in this study. Another recent study showed that this theoretical risk was not substantiated and that the rate of VTE was not increased in the anterior approach.6 Furthermore, this was a variable that was controlled for in the multivariate analysis. Regardless of approach aspirin appears to be an efficacious chemoprophylactic agent in patients with pelvic and acetabular fractures that undergo operative fixation.
Aspirin as an effective anticoagulation agent has been recognized in the total joint arthroplasty literature. [19] This study suggests that it is also an effective thromboprophylactic medication in pelvic and acetabular fractures and represents certain benefits for patients. The ease of administration compared to enoxaparin and heparin is a substantial consideration. Additionally, the relatively low cost of an over the counter medication is significant. These factors could potentially lead to increased patient compliance post-operatively.
This study is not without limitations. There are inherent limitations given the retrospective nature. Although it represents one of the larger cohorts of pelvic and acetabular fractures in the literature that reviews VTE prophylaxis, a larger population would be beneficial. With this small sample size that showed differences between groups such as less obesity, lower ISS, shorter ICU LOS and less restrictive weightbearing were analyzed using a multivariate regression model. However, a larger cohort examined prospectively would provide greater understanding of the optimal VTE prophylactic protocol. Furthermore, this study only examined aspirin compared to short-acting injectables, enoxaparin and heparin. However in there very few patients were excluded for receiving an alternative anticoagulation regimen for VTE prophylaxis, and thus this may not be a significant limitation. While this study suggests that aspirin is not inferior to other anticoagulants, larger randomized controlled trials are necessary to further determine the optimal anticoagulation agent to reduce the risk of both VTE and postoperative hematoma formation in operative pelvic and acetabular fractures.
This study suggests that aspirin is an acceptable method of VTE thromboprophylaxis with no inferior results to other common anticoagulants used in operative pelvis and acetabular fractures. In fact, aspirin is likely protective against hematoma formation in these injuries, making it potentially advantageous as hematoma increases infection risk and can lead to further complications in patient recovery.
Conflicts of Interest:
There are no conflicts of interest or sources of funding for any of the authors.
Conflicts of Interest and Source of Funding:
Dr. Ochenjele is a paid consultant for Stryker.
Dr. Wetzel is a paid consultant for Stryker, Biocomposites Inc, Bone Solutions Inc, and Medical Advance and receives royalties from Innomed Inc.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
